- You are here:
-
Home

-
Part V. Psychosocial and Organizational Factors
-
Psychosocial and Organizational Factors
- Factors Intrinsic to the Job

Factors Intrinsic to the Job
Person–Environment Fit
Person–environment fit (PE) theory offers a framework for assessing and predicting how characteristics of the employee and the work environment jointly determine worker well-being and, in the light of this knowledge, how a model for identifying points of preventive intervention may be elaborated. Several PE fit formulations have been proposed, the most widely known ones being those of Dawis and Lofquist (1984); French, Rodgers and Cobb (1974); Levi (1972); McGrath (1976); and Pervin (1967). The theory of French and colleagues, illustrated in figure 1, may be used to discuss the conceptual components of PE fit theory and their implications for research and application.
Figure 1. Schematic of French, Rogers and Cobb's theory of person-environment (PE) fit
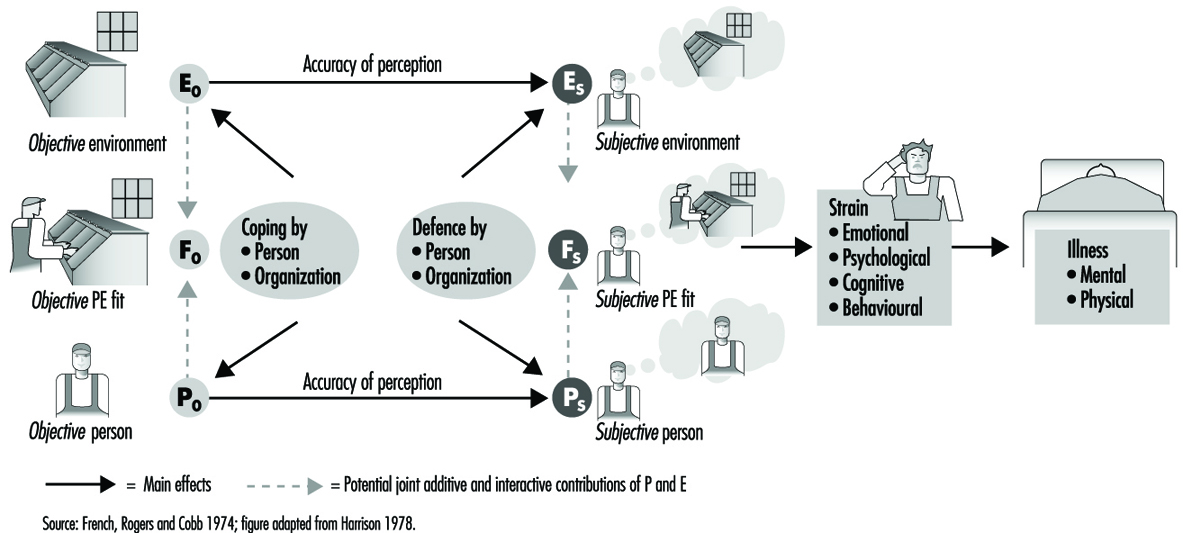
Poor PE fit can be viewed from the perspectives of the employee’s needs (needs–supplies fit) as well as the job–environment’s demands (demands–abilities fit). The term needs–supplies fit refers to the degree to which employee needs, such as the need to use skills and abilities, are met by the work environment’s supplies and opportunities to satisfy those needs. Demands–abilities fit refers to the degree to which the job’s demands are met by the employee’s skills and abilities. These two types of fit can overlap. For example, work overload may leave the employer’s demands unmet as well as threaten the employee’s need to satisfy others.
Conceptualizing Person (P) and Environment (E)
Characteristics of the person (P) include needs as well as abilities. Characteristics of the environment (E) include supplies and opportunities for meeting the employee’s needs as well as demands which are made on the employee’s abilities. In order to assess the degree to which P equals (or fits), exceeds, or is less than E, the theory requires that P and E be measured along commensurate dimensions. Ideally, P and E should be measured on equal interval scales with true zero points. For example, one could assess PE fit on workload for a data-entry operator in terms of both the number of data-entry keystrokes per minute demanded by the job (E) and the employee’s keystroke speed (P). As a less ideal alternative, investigators often use Likert type scales. For example, one could assess how much the employee wants to control the work pace (P) and how much control is provided by the job’s technology (E) by using a rating scale, where a value of 1 corresponds to no control, or almost no control and a value of 5 corresponds to complete control.
Distinguishing Subjective from Objective Fit
Subjective fit (FS) refers to the employee’s perceptions of P and E, whereas objective fit (FO) refers to assessments that are, in theory, free of subjective bias and error. In practice, there is always measurement error, so that it is impossible to construct truly objective measures. Consequently, many researchers prefer to create a working distinction between subjective and objective fit, referring to measures of objective fit as ones which are relatively, rather than absolutely, immune to sources of bias and error. For example, one can assess objective PE fit on keystroke ability by examining the fit between a count of required keystrokes per minute in the actual workload assigned to the employee (EO) and the employee’s ability as assessed on an objective-type test of keystroke ability (PO). Subjective PE fit might be assessed by asking the employee to estimate per minute keystroke ability (PS) and the number of keystrokes per minute demanded by the job (ES).
Given the challenges of objective measurement, most tests of PE fit theory have used only subjective measures of P and E (for an exception, see Chatman 1991). These measures have tapped a variety of dimensions including fit on responsibility for the work and well-being of other persons, job complexity, quantitative workload and role ambiguity.
Dynamic Properties of the PE Fit Model
Figure 1 depicts objective fit influencing subjective fit which, in turn, has direct effects on well-being. Well-being is broken down into responses called strains, which serve as risk factors for subsequent illness. These strains can involve emotional (e.g., depression, anxiety), physiological (e.g., serum cholesterol, blood pressure), cognitive (e.g., low self-evaluation, attributions of blame to self or others), as well as behavioural responses (e.g., aggression, changes in lifestyle, drug and alcohol use).
According to the model, levels of and changes in objective fit, whether due to planned intervention or otherwise, are not always perceived accurately by the employee, so that discrepancies arise between objective and subjective fit. Thus, employees can perceive good fit as well as poor fit when, objectively, such is not the case.
Inaccurate employee perceptions can arise from two sources. One source is the organization, which, unintentionally or by design (Schlenker 1980), may provide the employee with inadequate information regarding the environment and the employee. The other source is the employee. The employee might fail to access available information or might defensively distort objective information about what the job requires or about his or her abilities and needs — Taylor (1991) cites such an example.
French, Rodgers and Cobb (1974) use the concept of defences to refer to employee processes for distorting the components of subjective fit, PS and ES, without changing the commensurate components of objective fit, PO and EO. By extension, the organization can also engage in defensive processes—for example, cover-ups, denial or exaggeration—aimed at modifying employee perceptions of subjective fit without concomitantly modifying objective fit.
The concept of coping is, by contrast, reserved for responses and processes that aim to alter and, in particular, improve objective fit. The employee can attempt to cope by improving objective skills (PO) or by changing objective job demands and resources (EO) such as through a change of jobs or assigned responsibilities. By extension, the organization can also apply coping strategies to improve objective PE fit. For example, organizations can make changes in selection and promotion strategies, in training and in job design to alter EO and PO.
The distinctions between coping and defence on the one hand and objective and subjective fit on the other can lead to an array of practical and scientific questions regarding the consequences of using coping and defence and the methods for distinguishing between effects of coping and effects of defence on PE fit. By derivation from the theory, sound answers to such questions require sound measures of objective as well as subjective PE fit.
Statistical Models
PE fit can have non-linear relations with psychological strain. Figure 2 presents a U-shaped curve as an illustration. The lowest level of psychological strain on the curve occurs when employee and job characteristics fit each other (P = E). Strain increases as the employee’s abilities or needs respectively fall short of the job’s demands or resources (P
Figure 2. Hypothetical U-shaped relation of person-environment fit to psychological strain

Efficacy of the Model
A variety of different approaches to the measurement of PE fit demonstrate the model’s potential for predicting well-being and performance. For example, careful statistical modelling found that PE fit explained about 6% more variance in job satisfaction than was explained by measures of P or E alone (Edwards and Harrison 1993). In a series of seven studies of accountants measuring PE fit using a card-sort method, high-performers had higher correlations between P and E (average r = 0.47) than low performers (average r = 0.26; Caldwell and O’Reilly 1990). P was assessed as the employee’s knowledge, skills and abilities (KSAs), and E was assessed as the commensurate KSAs required by the job. Poor PE fit between the accountant’s values and the firm’s also served to predict employee turnover (Chatman 1991).
Workload
Workload and Brain Function
Knowledge about human needs, abilities and constraints provides guidelines for shaping psychosocial work conditions so as to reduce stress and improve occupational health (Frankenhaeuser 1989). Brain research and behavioural research have identified the conditions under which people perform well and the conditions under which performance deteriorates. When the total inflow of impressions from the outside world falls below a critical level and work demands are too low, people tend to become inattentive and bored and to lose their initiative. Under conditions of excessive stimulus flow and too high demands, people lose their ability to integrate messages, thought processes become fragmented and judgement is impaired. This inverted U-relationship between workload and brain function is a fundamental biological principle with wide applications in working life. Stated in terms of efficiency at different workloads, it means that the optimal level of mental functioning is located at the midpoint of a scale ranging from very low to very high work demands. Within this middle zone the degree of challenge is “just right”, and the human brain functions efficiently. The location of the optimal zone varies among different people, but the crucial point is that large groups spend their lives outside the optimal zone that would provide opportunities for them to develop their full potential. Their abilities are constantly either underutilized or overtaxed.
A distinction should be made between quantitative overload, which means too much work within a given time period, and qualitative underload, which means that tasks are too repetitive, lacking variety and challenge (Levi, Frankenhaeuser and Gardell 1986).
Research has identified criteria for “healthy work” (Frankenhaeuser and Johansson 1986; Karasek and Theorell 1990). These criteria emphasize that workers should be given the opportunity to: (a) influence and control their work; (b) understand their contribution in a wider context; (c) experience a sense of togetherness and belonging at their place of work; and (d) develop their own abilities and vocational skill by continuous learning.
Monitoring Bodily Responses at Work
People are challenged by different work demands whose nature and strength are appraised via the brain. The appraisal process involves a weighing, as it were, of the severity of the demands against one’s own coping abilities. Any situation which is perceived as a threat or challenge requiring compensatory effort is accompanied by the transmission of signals from the brain to the adrenal medulla, which responds with an output of the catecholamines epinephrine and norepinephrine. These stress hormones make us mentally alert and physically fit. In the event that the situation induces feelings of uncertainty and helplessness, the brain messages also travel to the adrenal cortex, which secretes cortisol, a hormone which plays an important part in the body’s immune defence (Frankenhaeuser 1986).
With the development of biochemical techniques that permit the determination of exceedingly small amounts of hormones in blood, urine and saliva, stress hormones have come to play an increasingly important role in research on working life. In the short term, a rise in stress hormones is often beneficial and seldom a threat to health. But in the longer term, the picture may include damaging effects (Henry and Stephens 1977; Steptoe 1981). Frequent or long-lasting elevations of stress-hormone levels in the course of daily life may result in structural changes in the blood vessels which, in turn, may lead to cardiovascular disease. In other words, consistently high levels of stress hormones should be regarded as warning signals, telling us that the person may be under excessive pressure.
Biomedical recording techniques permit the monitoring of bodily responses at the workplace without interfering with the worker’s activities. Using such ambulatory-monitoring techniques, one can find out what makes the blood pressure rise, the heart beat faster, the muscles tense up. These are important pieces of information which, together with stress-hormone assays, have helped in identifying both aversive and protective factors related to job content and work organization. Thus, when searching the work environment for harmful and protective factors, one can use the people themselves as “measuring rods”. This is one way in which the study of human stress and coping may contribute to intervention and prevention at the workplace (Frankenhaeuser et al. 1989; Frankenhaeuser 1991).
Personal Control as a “Buffer”
Data from both epidemiological and experimental studies support the notion that personal control and decision latitude are important “buffering” factors which help people to simultaneously work hard, enjoy their jobs and remain healthy (Karasek and Theorell 1990). The chance of exercising control may “buffer” stress in two ways: first, by increasing job satisfaction, thus reducing bodily stress responses, and secondly, by helping people develop an active, participatory work role. A job that allows the worker to use his or her skills to the full will increase self-esteem. Such jobs, while demanding and taxing, may help to develop competencies that aid in coping with heavy workloads.
The pattern of stress hormones varies with the interplay of positive versus negative emotional responses evoked by the situation. When demands are experienced as a positive and manageable challenge, the adrenaline output is typically high, whereas the cortisol-producing system is put to rest. When negative feelings and uncertainty dominate, both cortisol and adrenaline increase. This would imply that the total load on the body, the “cost of achievement”, will be lower during demanding, enjoyable work than during less demanding but tedious work, and it would seem that the fact that cortisol tends to be low in controllable situations could account for the positive health effects of personal control. Such a neuroendocrine mechanism could explain the epidemiological data obtained from national surveys in different countries which show that high job demands and work overload have adverse health consequences mainly when combined with low control over job-related decisions (Frankenhaeuser 1991; Karasek and Theorell 1990; Levi, Frankenhaeuser and Gardell 1986).
Total Workload of Women and Men
In order to assess the relative workloads associated with men’s and women’s different life situations, it is necessary to modify the concept of work so as to include the notion of total workload, that is, the combined load of demands related to paid and unpaid work. This includes all forms of productive activities defined as “all the things that people do that contribute to the goods and services that other people use and value” (Kahn 1991). Thus, a person’s total workload includes regular employment and overtime at work as well as housework, child care, care of elderly and sick relatives and work in voluntary organizations and unions. According to this definition, employed women have a higher workload than men at all ages and all occupational levels (Frankenhaeuser 1993a, 1993b and 1996; Kahn 1991).
The fact that the division of labour between spouses in the home has remained the same, while the employment situation of women has changed radically, has led to a heavy workload for women, with little opportunity for them to relax in the evenings (Frankenhaeuser et al. 1989). Until a better insight has been gained into the causal links between workload, stress and health, it will remain necessary to regard prolonged stress responses, displayed in particular by women at the managerial level, as warning signals of possible long-term health risks (Frankenhaeuser, Lundberg and Chesney 1991).
Hours of Work
Introduction
The patterning and duration of the hours a person works are a very important aspect of his or her experience of the work situation. Most workers feel that they are paid for their time rather than explicitly for their efforts, and thus the transaction between the worker and the employer is one of exchanging time for money. Thus, the quality of the time being exchanged is a very important part of the equation. Time that has high value because of its importance to the worker in terms of allowing sleep, interaction with family and friends and participation in community events may be more highly prized, and thus require extra financial compensation, as compared to normal “day work” time when many of the worker’s friends and family members are themselves at work or at school. The balance of the transaction can also be changed by making the time spent at work more congenial to the worker, for example, by improving working conditions. The commute to and from work is unavailable to the worker for recreation, so this time too must be considered as “grey time” (Knauth et al. 1983) and therefore a “cost” to the worker. Thus, measures such as compressed workweeks, which reduce the number of commuting trips taken per week, or flexitime, which reduces the commute time by allowing the worker to avoid the rush hour, are again likely to change the balance.
Background Literature
As Kogi (1991) has remarked, there is a general trend in both manufacturing and service industries towards greater flexibility in the temporal programming of work. There are a number of reasons for this trend, including the high cost of capital equipment, consumer demand for around-the-clock service, legislative pressure to reduce the length of the workweek and (in some societies such as the United States and Australia) taxation pressure on the employer to have as few different employees as possible. For many employees, the conventional “9 to 5” or “8 to 4”, Monday through Friday workweek is a thing of the past, either because of new work systems or because of the large amounts of excessive overtime required.
Kogi notes that while the benefits to the employer of such flexibility are quite clear in allowing extended business hours, accommodation of market demand and greater management flexibility, the benefits to the worker may be less certain. Unless the flexible schedule involves elements of choice for workers with respect to their particular hours of work, flexibility can often mean disruptions in their biological clocks and domestic situations. Extended work shifts may also lead to fatigue, compromising safety and productivity, as well as to increased exposure to chemical hazards.
Biological Disruptions due to Abnormal Work Hours
Human biology is specifically oriented towards wakefulness during daylight and sleep at night. Any work schedule which requires late evening or all-night wakefulness as a result of compressed workweeks, mandatory overtime or shiftwork will lead, therefore, to disruptions of the biological clock (Monk and Folkard 1992). These disruptions can be assessed by measuring workers’ “circadian rhythms”, which comprise regular fluctuations over the 24 hours in vital signs, blood and urine composition, mood and performance efficiency over the 24-hour period (Aschoff 1981). The measure used most often in shiftwork studies has been body temperature, which, under normal conditions, shows a clear rhythm with a peak at about 2000 hours, a trough at about 0500 hours and a difference of about 0.7°C. between the two. After an abrupt change in routine, the amplitude (size) of the rhythm diminishes and the phase (timing) of the rhythm is slow to adjust to the new schedule. Until the adjustment process is complete, sleep is disrupted and daytime mood and performance efficiency are impaired. These symptoms can be regarded as the shiftwork equivalent of jet-lag and can be extremely long lasting (Knauth and Rutenfranz 1976).
Abnormal work hours can also lead to poor health. Although it has proved difficult to precisely quantify the exact size of the effect, it appears that, in addition to sleep disorders, gastrointestinal disorders (including peptic ulcers) and cardiovascular disease can be more frequently found in shift workers (and former shift workers) than in day workers (Scott and LaDou 1990). There is also some preliminary evidence for increased incidence of psychiatric symptoms (Cole, Loving and Kripke 1990).
Social Disruptions due to Abnormal Work Hours
Not only human biology, but also human society, opposes those who work abnormal hours. Unlike the nocturnal sleep of the majority, which is carefully protected by strict taboos against loud noise and telephone use at night, the late wakening, day-sleeping and napping that are required by those working abnormal work hours is only grudgingly tolerated by society. Evening and weekend community events can also be denied to these people, leading to feelings of alienation.
It is with the family, however, that the social disruptions of abnormal work hours may be the most devastating. For the worker, the family roles of parent, caregiver, social companion and sexual partner can all be severely compromised by abnormal work hours, leading to marital disharmony and problems with children (Colligan and Rosa 1990). Moreover, the worker’s attempts to rectify, or to avoid, such social problems may result in a decrease in sleep time, thus leading to poor alertness and compromised safety and productivity.
Suggested Solutions
Just as the problems of abnormal work hours are multifaceted, so too must be the solutions to those problems. The primary areas to be addressed should include:
- selection and education of the worker
- selection of the most appropriate work schedule or roster
- improvement of the work environment.
Selection and education of the worker should involve identification and counselling of those persons likely to experience difficulties with abnormal or extended work hours (e.g., older workers and those with high sleep needs, extensive domestic workloads or long commutes). Education in circadian and sleep hygiene principles and family counselling should also be made available (Monk and Folkard 1992). Education is an extremely powerful tool in helping those with abnormal work hours to cope, and in reassuring them about why they may be experiencing problems. Selection of the most appropriate schedule should begin with a decision as to whether abnormal work hours are actually needed at all. For example, night work may in many cases be done better at a different time of day (Knauth and Rutenfranz 1982). Consideration should be also be given to the schedule best suited to the work situation, bearing in mind the nature of the work and the demographics of the workforce. Improvement of the work environment may involve raising illumination levels and providing adequate canteen facilities at night.
Conclusions
The particular pattern of work hours chosen for an employee can represent a significant challenge to his or her biology, domestic situation and role in the community. Informed decisions should be made, incorporating a study of the demands of the work situation and the demographics of the workforce. Any changes in hours of work should be preceded by detailed investigation and consultation with the employees and followed by evaluation studies.
Environmental Design
Overview
In this article, the links between the physical features of the workplace and occupational health are examined. Workplace design is concerned with a variety of physical conditions within work environments that can be objectively observed or recorded and modified through architectural, interior design and site planning interventions. For the purposes of this discussion, occupational health is broadly construed to encompass multiple facets of workers’ physical, mental and social well-being (World Health Organization 1984). Thus, a broad array of health outcomes is examined, including employee satisfaction and morale, work-group cohesion, stress reduction, illness and injury prevention, as well as environmental supports for health promotion at the worksite.
Empirical evidence for the links between workplace design and occupational health is reviewed below. This review, highlighting the health effects of specific design features, must be qualified in certain respects. First, from an ecological perspective, worksites function as complex systems comprised of multiple social and physical environmental conditions, which jointly influence employee well-being (Levi 1992; Moos 1986; Stokols 1992). Thus, the health consequences of environmental conditions are often cumulative and sometimes involve complex mediated and moderated relationships among the sociophysical environment, personal resources and dispositions (Oldham and Fried 1987; Smith 1987; Stellman and Henifin 1983). Moreover, enduring qualities of people-environment transaction, such as the degree to which employees perceive their work situation to be controllable, socially supportive and compatible with their particular needs and abilities, may have a more pervasive influence on occupational health than any single facet of workplace design (Caplan 1983; Karasek and Theorell 1990; Parkes 1989; Repetti 1993; Sauter, Hurrell and Cooper 1989). The research findings reviewed should be interpreted in light of these caveats.
Research Findings
The relationships between worksite design and occupational health can be considered at several levels of analysis, including the:
- physical arrangement of employees’ immediate work area
- ambient environmental qualities of the work area
- physical organization of buildings that comprise a particular workplace
- exterior amenities and site planning of those facilities.
Previous research has focused primarily on the first and second levels, while giving less attention to the third and fourth levels of workplace design.
Physical features of the immediate work area
The immediate work area extends from the core of an employee’s desk or workstation to the physical enclosure or imaginary boundary surrounding his or her work space. Several features of the immediate work area have been found to influence employee well-being. The degree of physical enclosure surrounding one’s desk or workstation, for example, has been shown in several studies to be positively related to the employee’s perception of privacy, satisfaction with the work environment and overall job satisfaction (Brill, Margulis and Konar 1984; Hedge 1986; Marans and Yan 1989; Oldham 1988; Sundstrom 1986; Wineman 1986). Moreover, “open-plan” (low enclosure) work areas have been linked to more negative social climates in work groups (Moos 1986) and more frequent reports of headaches among employees (Hedge 1986). It is important to note, however, that the potential health effects of workstation enclosure may depend on the type of work being performed (e.g., confidential versus non-confidential, team versus individualized tasks; see Brill, Margulis and Konar 1984), job status (Sundstrom 1986), levels of social density adjacent to one’s work area (Oldham and Fried 1987), and workers’ needs for privacy and stimulation screening (Oldham 1988).
A number of studies have shown that the presence of windows in the employees’ immediate work areas (especially windows that afford views of natural or landscaped settings), exposure to indoor natural elements (e.g., potted plants, pictures of wilderness settings), and opportunities to personalize the decor of one’s office or workstation are associated with higher levels of environmental and job satisfaction and lower levels of stress (Brill, Margulis and Konar 1984; Goodrich 1986; Kaplan and Kaplan 1989; Steele 1986; Sundstrom 1986). Providing employees with localized controls over acoustic, lighting and ventilation conditions within their work areas has been linked to higher levels of environmental satisfaction and lower levels of stress in some studies (Becker 1990; Hedge 1991; Vischer 1989). Finally, several research programmes have documented the health benefits associated with employees’ use of adjustable, ergonomically sound furniture and equipment; these benefits include reduced rates of eyestrain and of repetitive motion injuries and lower back pain (Dainoff and Dainoff 1986; Grandjean 1987; Smith 1987).
Ambient environmental qualities of the work area
Ambient environmental conditions originate from outside the worker’s immediate work area. These pervasive qualities of the worksite influence the comfort and well-being of employees whose work spaces are located within a common region (e.g., a suite of offices located on one floor of a building). Examples of ambient environmental qualities include levels of noise, speech privacy, social density, illumination and air quality—conditions that are typically present within a particular portion of the worksite. Several studies have documented the adverse health impacts of chronic noise disturbance and low levels of speech privacy in the workplace, including elevated levels of physiological and psychological stress and reduced levels of job satisfaction (Brill, Margulis and Konar 1984; Canter 1983; Klitzman and Stellman 1989; Stellman and Henifin 1983; Sundstrom 1986; Sutton and Rafaeli 1987). High levels of social density in the immediate vicinity of one’s work area have also been linked with elevated stress levels and reduced job satisfaction (Oldham 1988; Oldham and Fried 1987; Oldham and Rotchford 1983).
Health consequences of office lighting and ventilation systems have been observed as well. In one study, lensed indirect fluorescent uplighting was associated with higher levels of employee satisfaction and reduced eyestrain, in comparison with traditional fluorescent downlighting (Hedge 1991). Positive effects of natural lighting on employees’ satisfaction with the workplace also have been reported (Brill, Margulis and Konar 1984; Goodrich 1986; Vischer and Mees 1991). In another study, office workers exposed to chilled-air ventilation systems evidenced higher rates of upper-respiratory problems and physical symptoms of “sick building syndrome” than those whose buildings were equipped with natural or mechanical (non-chilled, non-humidified) ventilation systems (Burge et al. 1987; Hedge 1991).
Features of the ambient environment that have been found to enhance the social climate and cohesiveness of work groups include the provision of team-oriented spaces adjacent to individualized offices and workstations (Becker 1990; Brill, Margulis and Konar 1984; Steele 1986; Stone and Luchetti 1985) and visible symbols of corporate and team identity displayed within lobbies, corridors, conference rooms, lounges and other collectively used areas of the worksite (Becker 1990; Danko, Eshelman and Hedge 1990; Ornstein 1990; Steele 1986).
Overall organization of buildings and facilities
This level of design encompasses the interior physical features of work facilities that extend throughout an entire building, many of which are not immediately experienced within an employee’s own work space or within those adjacent to it. For example, enhancing the structural integrity and fire-resistance of buildings, and designing stairwells, corridors and factories to prevent injuries, are essential strategies for promoting worksite safety and health (Archea and Connell 1986; Danko, Eshelman and Hedge 1990). Building layouts that are consistent with the adjacency needs of closely interacting units within an organization can improve coordination and cohesion among work groups (Becker 1990; Brill, Margulis and Konar 1984; Sundstrom and Altman 1989). The provision of physical fitness facilities at the worksite has been found to be an effective strategy for enhancing employees’ health practices and stress management (O’Donnell and Harris 1994). Finally, the presence of legible signs and wayfinding aids, attractive lounge and dining areas, and child-care facilities at the worksite have been identified as design strategies that enhance employees’ job satisfaction and stress management (Becker 1990; Brill, Margulis and Konar 1984; Danko, Eshelman and Hedge 1990; Steele 1986; Stellman and Henifin 1983; Vischer 1989).
Exterior amenities and site planning
Exterior environmental conditions adjacent to the worksite may also carry health consequences. One study reported an association between employees’ access to landscaped, outdoor recreational areas and reduced levels of job stress (Kaplan and Kaplan 1989). Other researchers have suggested that the geographic location and site planning of the worksite can influence the mental and physical well-being of workers to the extent that they afford greater access to parking and public transit, restaurants and retail services, good regional air quality and the avoidance of violent or otherwise unsafe areas in the surrounding neighbourhood (Danko, Eshelman and Hedge 1990; Michelson 1985; Vischer and Mees 1991). However, the health benefits of these design strategies have not yet been evaluated in empirical studies.
Directions for Future Research
Prior studies of environmental design and occupational health reflect certain limitations and suggest several issues for future investigation. First, earlier research has emphasized the health effects of specific design features (e.g., workstation enclosure, furnishings, lighting systems), while neglecting the joint influence of physical, interpersonal and organizational factors on well-being. Yet the health benefits of improved environmental design may be moderated by the social climate and organizational qualities (as moderated, for example, by a participative versus non-participative structure) of the workplace (Becker 1990; Parkes 1989; Klitzman and Stellman 1989; Sommer 1983; Steele 1986). The interactive links between physical design features, employee characteristics, social conditions at work and occupational health, therefore, warrant greater attention in subsequent studies (Levi 1992; Moos 1986; Stokols 1992). At the same time, an important challenge for future research is to clarify the operational definitions of particular design features (e.g., the “open plan” office), which have varied widely in earlier studies (Brill, Margulis and Konar 1984; Marans and Yan 1989; Wineman 1986).
Secondly, employee characteristics such as job status, gender and dispositional styles have been found to mediate the health consequences of worksite design (Burge et al. 1987; Oldham 1988; Hedge 1986; Sundstrom 1986). Yet, it is often difficult to disentangle the separate effects of environmental features and individual differences (these differences may have to do with, for example, workstation enclosures, comfortable furnishings, and job status) because of ecological correlations among these variables (Klitzman and Stellman 1989). Future studies should incorporate experimental techniques and sampling strategies that permit an assessment of the main and interactive effects of personal and environmental factors on occupational health. Moreover, specialized design and ergonomic criteria to enhance the health of diverse and vulnerable employee groups (e.g., disabled, elderly and single-parent female workers) remain to be developed in future research (Michelson 1985; Ornstein 1990; Steinfeld 1986).
Thirdly, prior research on the health outcomes of worksite design has relied heavily on survey methods to assess employees’ perceptions of both their work environments and health status, placing certain constraints (for example, “common method variance”) on the interpretation of data (Klitzman and Stellman 1989; Oldham and Rotchford 1983). Furthermore, the majority of these studies have used cross-sectional rather than longitudinal research designs, the latter incorporating comparative assessments of intervention and control groups. Future studies should emphasize both field-experimental research designs and multi-method strategies that combine survey techniques with more objective observations and recordings of environmental conditions, medical exams and physiological measures.
Finally, the health consequences of building organization, exterior amenities and site-planning decisions have received considerably less attention in prior studies than those associated with the more immediate, ambient qualities of employees’ work areas. The health relevance of both proximal and remote aspects of workplace design should be examined more closely in future research.
Role of Workplace Design in Illness Prevention and Health Promotion
Several environmental design resources and their potential health benefits are summarized in table 1, based on the preceding review of research findings. These resources are grouped according to the four levels of design noted above and emphasize physical features of work settings that have been empirically linked to improved mental, physical and social health outcomes (especially those found at levels 1 and 2), or have been identified as theoretically plausible leverage points for enhancing employee well-being (e.g., several of the features subsumed under levels 3 and 4).
Table 1. Workplace design resources and potential health benefits
| Levels of environmental design | Environmental design features of the workplace | Emotional, social and physical health outcomes |
| Immediate work area | Physical enclosure of the work area Adjustable furniture and equipment Localized controls of acoustics, lighting and ventilation Natural elements and personalized decor Presence of windows in work area |
Enhanced privacy and job satisfaction Reduced eyestrain and repetitive-strain and lower-back injuries Enhanced comfort and stress reduction Enhanced sense of identity and involvement at the workplace Job satisfaction and stress reduction |
| Ambient qualities of the work area |
Speech privacy and noise control Comfortable levels of social density Good mix of private and team spaces Symbols of corporate and team identity Natural, task, and lensed indirect lighting Natural ventilation vs. chilled-air systems |
Lower physiological, emotional stress Lower physiological, emotional stress Improved social climate, cohesion Improved social climate, cohesion Reduced eyestrain, enhanced satisfaction Lower rates of respiratory problems |
| Building organization | Adjacencies among interacting units Legible signage and wayfinding aids Injury-resistant architecture Attractive lounge and food areas onsite Availability of worksite child care Physical fitness facilities onsite |
Enhanced coordination and cohesion Reduced confusion and distress Lower rates of unintentional injuries Enhanced satisfaction with job, worksite Employee convenience, stress reduction Improved health practices, lower stress |
| Exterior amenities and site planning |
Availability of outside recreation areas Access to parking and public transit Proximity to restaurants and stores Good air quality in surrounding area Low levels of neighbourhood violence |
Enhanced cohesion, stress reduction Employee convenience, stress reduction Employee convenience, stress reduction Improved respiratory health Reduced rates of intentional injuries |
The incorporation of these resources into the design of work environments should, ideally, be combined with organizational and facilities management policies that maximize the health- promoting qualities of the workplace. These corporate policies include:
- the designation of worksites as “smoke-free” (Fielding and Phenow 1988)
- the specification and use of non-toxic, ergonomically sound furnishings and equipment (Danko, Eshelman and Hedge 1990)
- managerial support for employees’ personalization of their workspace (Becker 1990; Brill, Margulis and Konar 1984; Sommer 1983; Steele 1986)
- job designs that prevent health problems linked with computer-based work and repetitive tasks (Hackman and Oldham 1980; Sauter, Hurrell and Cooper 1989; Smith and Sainfort 1989)
- the provision of employee training programmes in the areas of ergonomics and occupational safety and health (Levy and Wegman 1988)
- incentive programmes to encourage employees’ use of physical fitness facilities and compliance with injury prevention protocols (O’Donnell and Harris 1994)
- flexitime, telecommuting, job-sharing and ride-sharing programmes to enhance workers’ effectiveness in residential and corporate settings (Michelson 1985; Ornstein 1990; Parkes 1989; Stokols and Novaco 1981)
- the involvement of employees in the planning of worksite relocations, renovations and related organizational developments (Becker 1990; Brill, Margulis and Konar 1984; Danko, Eshelman and Hedge 1990; Miller and Monge 1986; Sommer 1983; Steele 1986; Stokols et al. 1990).
Organizational efforts to enhance employee well-being are likely to be more effective to the extent that they combine complementary strategies of environmental design and facilities management, rather than relying exclusively on either one of these approaches.
Ergonomic Factors
The purpose of this article is to afford the reader an understanding of how ergonomic conditions can affect the psychosocial aspects of working, employee satisfaction with the work environment, and employee health and well-being. The major thesis is that, with respect to physical surroundings, job demands and technological factors, improper design of the work environment and job activities can cause adverse employee perceptions, psychological stress and health problems (Smith and Sainfort 1989; Cooper and Marshall 1976).
Industrial ergonomics is the science of fitting the work environment and job activities to the capabilities, dimensions and needs of people. Ergonomics deals with the physical work environment, tools and technology design, workstation design, job demands and physiological and biomechanical loading on the body. Its goal is to increase the degree of fit among the employees, the environments in which they work, their tools and their job demands. When the fit is poor, stress and health problems can occur. The many relationships between the demands of the job and psychological distress are discussed elsewhere in this chapter as well as in Smith and Sainfort (1989), in which a definition is given of the balance theory of job stress and job design. Balance is the use of different aspects of job design to counteract job stressors. The concept of job balance is important in the examination of ergonomic considerations and health. For instance, the discomforts and disorders produced by poor ergonomic conditions can make an individual more susceptible to job stress and psychological disorders, or can intensify the somatic effects of job stress.
As spelled out by Smith and Sainfort (1989), there are various sources of job stress, including
- job demands such as high workload and work pace
- poor job content factors that produce boredom and lack of meaningfulness
- limited job control or decision latitude
- organizational policies and procedures that alienate the workforce
- supervisory style affecting participation and socialization
- environmental contamination
- technology factors
- ergonomic conditions.
Smith (1987) and Cooper and Marshall (1976) discuss the characteristics of the workplace that can cause psychological stress. These include improper workload, heavy work pressure, hostile environment, role ambiguity, lack of challenging tasks, cognitive overload, poor supervisory relations, lack of task control or decision-making authority, poor relationship with other employees and lack of social support from supervisors, fellow employees and family.
Adverse ergonomic characteristics of work can cause visual, muscular and psychological disturbances such as visual fatigue, eye strain, sore eyes, headaches, fatigue, muscle soreness, cumulative trauma disorders, back disorders, psychological tension, anxiety and depression. Sometimes these effects are temporary and may disappear when the individual is removed from work or given an opportunity to rest at work, or when the design of the work environment is improved. When exposure to poor ergonomic conditions is chronic, then the effects can become permanent. Visual and muscular disturbances, and aches and pains can induce anxiety in employees. The result may be psychological stress or an exacerbation of the stress effects of other adverse working conditions that cause stress. Visual and musculoskeletal disorders that lead to a loss of function and disability can lead to anxiety, depression, anger and melancholy. There is a synergistic relationship among the disorders caused by ergonomic misfit, so that a circular effect is created in which visual or muscular discomfort generates more psychological stress, which then leads to a greater sensitivity in pain perception in the eyes and muscles, which leads to more stress and so on.
Smith and Sainfort (1989) have defined five elements of the work system that are significant in the design of work that relate to the causes and control of stress. These are: (1) the person; (2) the physical work environment; (3) tasks; (4) technology; and (5) work organization. All but the person are discussed.
Physical Work Environment
The physical work environment produces sensory demands which affect an employee’s ability to see, hear and touch properly, and includes such features as air quality, temperature and humidity. In addition, noise is one of the most prominent of the ergonomic conditions that produce stress (Cohen and Spacapan 1983). When physical working conditions produce a “poor fit” with employees’ needs and capabilities, generalized fatigue, sensory fatigue and performance frustration are the result. Such conditions can lead to psychological stress (Grandjean 1968).
Technology and Workstation Factors
Various aspects of technology have proved troublesome for employees, including incompatible controls and displays, poor response characteristics of controls, displays with poor sensory sensitivity, difficulty in operating characteristics of the technology, equipment that impairs employee performance and equipment breakdowns (Sanders and McCormick 1993; Smith et al. 1992a). Research has shown that employees with such problems report more physical and psychological stress (Smith and Sainfort 1989; Sauter, Dainoff and Smith 1990).
Tasks
Two very critical ergonomic task factors that have been tied to job stress are heavy workloads and work pressure (Cooper and Smith 1985). Too much or too little work produces stress, as does unwanted overtime work. When employees must work under time pressure, for example, to meet deadlines or when the workload is unrelentingly high, then stress is also high. Other critical task factors that have been tied to stress are machine pacing of the work process, a lack of cognitive content of the job tasks and low task control. From an ergonomic perspective, workloads should be established using scientific methods of time and motion evaluation (ILO 1986), and not be set by other criteria such as economic need to recover capital investment or by the capacity of the technology.
Organizational Factors
Three ergonomic aspects of the management of the work process have been identified as conditions that can lead to employee psychological stress. These are shift work, machine-paced work or assembly-line work, and unwanted overtime (Smith 1987). Shift work has been shown to disrupt biological rhythms and basic physiological functioning (Tepas and Monk 1987; Monk and Tepas 1985). Machine-paced work or assembly-line work that produces short-cycle tasks with little cognitive content and low employee control over the process leads to stress (Sauter, Hurrell and Cooper 1989). Unwanted overtime can lead to employee fatigue and to adverse psychological reactions such as anger and mood disturbances (Smith 1987). Machine-paced work, unwanted overtime and perceived lack of control over work activities have also been linked to mass psychogenic illness (Colligan 1985).
Autonomy and Control
Autonomy and job control are concepts with a long history in the study of work and health. Autonomy—the extent to which workers can exercise discretion in how they perform their work—is most closely associated with theories that are concerned with the challenge of designing work so that it is intrinsically motivating, satisfying and conducive to physical and mental well-being. In virtually all such theories, the concept of autonomy plays a central role. The term control (defined below) is generally understood to have a broader meaning than autonomy. In fact, one could consider autonomy to be a specialized form of the more general concept of control. Because control is the more inclusive term, it will be used throughout the remainder of this article.
Throughout the 1980s, the concept of control formed the core of perhaps the most influential theory of occupational stress (see, for example, the review of the work stress literature by Ganster and Schaubroeck 1991b). This theory, usually known as the Job Decision Latitude Model (Karasek 1979) stimulated many large-scale epidemiological studies that investigated the joint effects of control in conjunction with a variety of demanding work conditions on worker health. Though there has been some controversy regarding the exact way that control might help determine health outcomes, epidemiologists and organizational psychologists have come to regard control as a critical variable that should be given serious consideration in any investigation of psychosocial work stress conditions. Concern for the possible detrimental effects of low worker control was so high, for example, that in 1987 the National Institute for Occupational Safety and Health (NIOSH) of the United States organized a special workshop of authorities from epidemiology, psychophysiology, and industrial and organizational psychology to critically review the evidence concerning the impact of control on worker health and well-being. This workshop eventually culminated in the comprehensive volume Job Control and Worker Health (Sauter, Hurrell and Cooper 1989) that provides a discussion of the global research efforts on control. Such widespread acknowledgement of the role of control in worker well-being also had an impact on governmental policy, with the Swedish Work Environment Act (Ministry of Labour 1987) stating that “the aim must be for work to be arranged in such a way so that the employee himself can influence his work situation”. In the remainder of this article I summarize the research evidence on work control with the goal of providing the occupational health and safety specialist with the following:
- a discussion of aspects of worker control that might be important
- guidelines about how to assess job control in the worksite
- ideas on how to intervene so as to reduce the deleterious effects of low worker control.
First, what exactly is meant by the term control? In its broadest sense it refers to workers’ ability to actually influence what happens in their work environment. Moreover, this ability to influence the work setting should be considered in light of the worker’s goals. The term refers to the ability to influence matters that are relevant to one’s personal goals. This emphasis on being able to influence the work environment distinguishes control from the related concept of predictability. The latter refers to one’s being able to anticipate what demands will be made on oneself, for example, but does not imply any ability to alter those demands. Lack of predictability constitutes a source of stress in its own right, particularly when it produces a high level of ambiguity about what performance strategies one ought to adopt to perform effectively or if one even has a secure future with the employer. Another distinction that should be made is that between control and the more inclusive concept of job complexity. Early conceptualizations of control considered it together with such aspects of work as skill level and availability of social interaction. Our discussion here discriminates control from these other domains of job complexity.
One can consider mechanisms by which workers can exercise control and the domains over which that control can apply. One way that workers can exercise control is by making decisions as individuals. These decisions can be about what tasks to complete, the order of those tasks, and the standards and processes to follow in completing those tasks, to name but a few. The worker might also have some collective control either through representation or by social action with co-workers. In terms of domains, control might apply to such matters as the work pace, the amount and timing of interaction with others, the physical work environment (lighting, noise and privacy), scheduling of vacations or even matters of policy at the worksite. Finally, one can distinguish between objective and subjective control. One might, for example, have the ability to choose one’s work pace but not be aware of it. Similarly, one might believe that one can influence policies in the workplace even though this influence is essentially nil.
How can the occupational health and safety specialist assess the level of control in a work situation? As recorded in the literature, basically two approaches have been taken. One approach has been to make an occupational-level determination of control. In this case every worker in a given occupation would be considered to have the same level of control, as it is assumed to be determined by the nature of the occupation itself. The disadvantage to this approach, of course, is that one cannot obtain much insight as to how workers are faring in a particular worksite, where their control might have been determined as much by their employer’s policies and practices as by their occupational status. The more common approach is to survey workers about their subjective perceptions of control. A number of psychometrically sound measures have been developed for this purpose and are readily available. The NIOSH control scale (McLaney and Hurrell 1988), for example, consists of sixteen questions and provides assessments of control in the domains of task, decision, resources and physical environment. Such scales can easily be incorporated into an assessment of worker safety and health concerns.
Is control a significant determinant of worker safety and health? This question has driven many large-scale research efforts since at least 1985. Since most of these studies have consisted of non- experimental field surveys in which control was not purposely manipulated, the evidence can only show a systematic correlation between control and health and safety outcome variables. The lack of experimental evidence prevents us from making direct causal assertions, but the correlational evidence is quite consistent in showing that workers with lower levels of control suffer more from mental and physical health complaints. The evidence is strongly suggestive, then, that increasing worker control constitutes a viable strategy for improving the health and welfare of workers. A more controversial question is whether control interacts with other sources of psychosocial stress to determine health outcomes. That is, will high control levels counteract the deleterious effects of other job demands? This is an intriguing question, for, if true, it suggests that the ill effects of high workloads, for example, can be negated by increasing worker control with no corresponding need to lower workload demands. The evidence is clearly mixed on this question, however. About as many investigators have reported such interaction effects as have not. Thus, control should not be considered a panacea that will cure the problems brought on by other psychosocial stressors.
Work by organizational researchers suggests that increasing worker control can significantly improve health and well-being. Moreover, it is relatively easy to make a diagnosis of low worker control through the use of brief survey measures. How can the health and safety specialist intervene, then, to increase worker control levels? As there are many domains of control, there are many ways to increase workplace control. These range from providing opportunities for workers to participate in decisions that affect them to the fundamental redesign of jobs. What is clearly important is that control domains be targeted that are relevant to the primary goals of the workers and that fit the situational demands. These domains can probably best be determined by involving workers in joint diagnosis and problem-solving sessions. It should be noted, however, that the kinds of changes in the workplace that in many cases are necessary to achieve real gains in control involve fundamental changes in management systems and policies. Increasing control might be as simple as providing a switch that allows machine-paced workers to control their pace, but it is just as likely to involve important changes in the decision-making authority of workers. Thus, organizational decision makers must usually be full and active supporters of control enhancing interventions.
Work Pacing
In this article, the reasons machine-pacing is utilized in the workplace are reviewed. Furthermore, a classification of machine-paced work, information on the impact of machine-paced work on well-being and methodologies by which the effects can be alleviated or reduced, are set forth.
Benefits of Machine-Paced Work
The effective utilization of machine-paced work has the following benefits for an organization:
- It increases customer satisfaction: for example, it provides speedier service in drive-in restaurants when a number of stations are assigned to serve the customers sequentially.
- It reduces overhead cost through economic use of high technology, reduction of stock set aside for processing, reduction in factory floor space and reduction in supervisory costs.
- It reduces direct costs through reduced training time, lower hourly wages and high production return per unit of wages.
- It contributes to national productivity through provision of employment for unskilled workers and reduction in the production costs of goods and services.
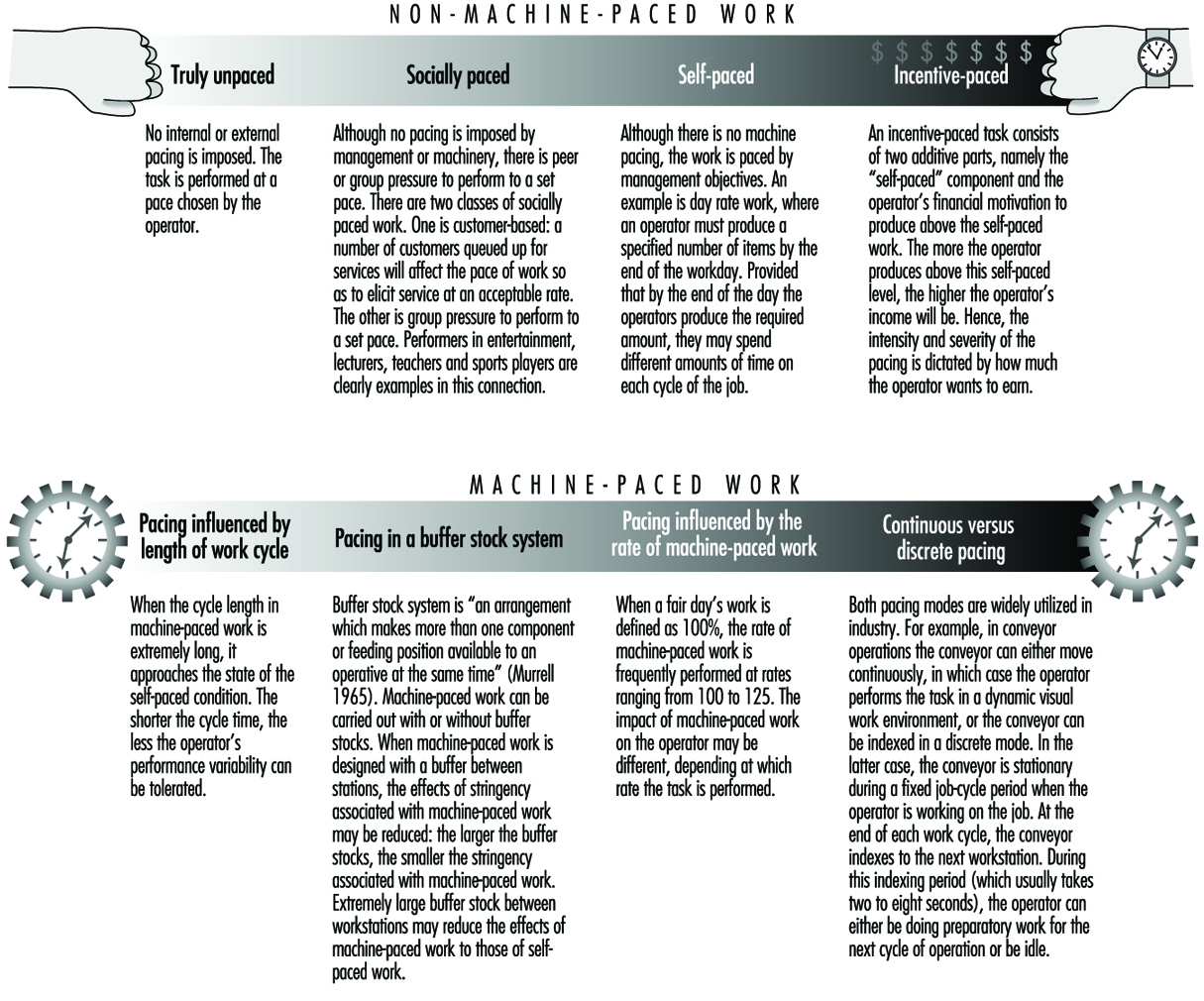
Classification of Machine-Paced Work
A classification of paced work is provided in figure 1.
Figure 1. The Job Stress Model of the National Institute for Occupational Safety and Health (NIOSH)
Effect of Machine-Paced Work on Well-Being
Machine-paced research has been carried out in laboratory settings, in industry (by case studies and controlled experiments) and by epidemiological studies (Salvendy 1981).
An analysis was performed of 85 studies dealing with machine-paced and self-paced work, of which 48% were laboratory studies, 30% industrial, 14% review studies, 4% combined laboratory and industrial, and 4% conceptual studies (Burke and Salvendy 1981). Of the 103 variables used in these studies, 41% were physiological, 32% were performance variables and 27% psychological. From this analysis, the following practical implications were derived for the use of machine-paced versus self-paced work arrangements :
- Tasks with high cognitive or perceptual load should be administered under self-paced as opposed to machine-paced conditions.
- To reduce error and low productivity, jobs should be allocated according to the worker’s personality and capacities.
- Intelligent, shrewd, creative and self-sufficient operators prefer to work on self-paced rather than machine-paced tasks. (See table 1 for more complete psychological profiles.)
- Workers should be encouraged to select a workload capacity which is optimum for them in any given situation.
- To maintain a high activation level (or the required level for performing the task), the work sessions should be interrupted by rest periods or by other types of work. This type of break should be implemented before the onset of deactivation.
- Maximal work speeds are not economical and can result in workers’ becoming overstrained when they continue to work excessively fast for a long time. On the other hand, too low a speed may also be detrimental to workers’ performance.
In studying industrial workers for an entire year in our experimentally controlled situation, in which over 50 million data points were collected, it was shown that 45% of the labour force prefers self-paced work, 45% prefers machine-paced work, and 10% does not like work of any type (Salvendy1976).
Table 1. Psychological profiles of operators who prefer self-paced and machine-paced work
|
Machine-paced work |
Self-paced work |
|
Less intelligent |
More intelligent |
|
Humble |
Assertive |
|
Practical |
Imaginative |
|
Forthright |
Shrewd |
|
Group-dependent |
Self-sufficient |
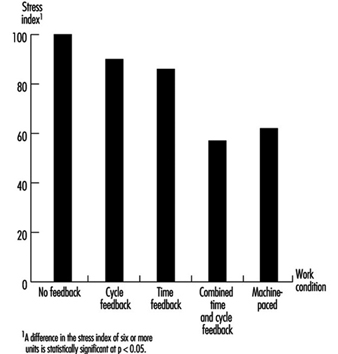
Uncertainty is the most significant contributor to stress and can be effectively managed by performance feedback (see figure 2) (Salvendy and Knight 1983).
Figure 2. Effects of performance feedback on reduction of stress
Electronic Work Monitoring
The computerization of work has made possible the development of a new approach to work monitoring called electronic performance monitoring (EPM). EPM has been defined as the “computerized collection, storage, analysis, and reporting of information about employees’ activities on a continuous basis” (USOTA 1987). Although banned in many European countries, electronic performance monitoring is increasing throughout the world on account of intense competitive pressures to improve productivity in a global economy.
EPM has changed the psychosocial work environment. This application of computer technology has significant implications for work supervision, workload demands, performance appraisal, performance feedback, rewards, fairness and privacy. As a result, occupational health researchers, worker representatives, government agencies and the public news media have expressed concern about the stress-health effects of electronic performance monitoring (USOTA 1987).
Traditional approaches to work monitoring include direct observation of work behaviours, examination of work samples, review of progress reports and analysis of performance measures (Larson and Callahan 1990). Historically, employers have always attempted to improve on these methods of monitoring worker performance. Considered as part of a continuing monitoring effort across the years, then, EPM is not a new development. What is new, however, is the use of EPM, particularly in office and service work, to capture employee performance on a second-by-second, keystroke-by-keystroke basis so that work management in the form of corrective action, performance feedback, delivery of incentive pay, or disciplinary measures can be taken at any time (Smith 1988). In effect, the human supervisor is being replaced by an electronic supervisor.
EPM is used in office work such as word processing and data entry to monitor keystroke production and error rates. Airline reservation clerks and directory assistance operators are monitored by computers to determine how long it takes to service customers and to measure the time interval between calls. EPM also is used in more traditional economic sectors. Freight haulers, for example, are using computers to monitor driver speed and fuel consumption, and tire manufacturers are electronically monitoring the productivity of rubber workers. In sum, EPM is used to establish performance standards, track employee performance, compare actual performance with predetermined standards and administer incentive pay programmes based on these standards (USOTA 1987).
Advocates of EPM assert that continuous electronic work monitoring is essential to high performance and productivity in the contemporary workplace. It is argued that EPM enables managers and supervisors to organize and control human, material and financial resources. Specifically, EPM provides for:
- increased control over performance variability
- increased objectivity and timeliness of performance evaluation and feedback
- efficient management of large office and customer service operations through the electronic supervision of work, and
- establishment and enforcement of performance standards (for example, number of forms processed per hour).
Supporters of electronic monitoring also claim that, from the worker’s perspective, there are several benefits. Electronic monitoring, for example, can provide regular feedback of work performance, which enables workers to take corrective action when necessary. It also satisfies the worker’s need for self-evaluation and reduces performance uncertainty.
Despite the possible benefits of EPM, there is concern that certain monitoring practices are abusive and constitute an invasion of employee privacy (USOTA 1987). Privacy has become an issue particularly when workers do not know when or how often they are being monitored. Since work organizations often do not share performance data with workers, a related privacy issue is whether workers should have access to their own performance records or the right to question possible wrong information.
Workers also have raised objections to the manner in which monitoring systems have been implemented (Smith, Carayon and Miezio 1986; Westin 1986). In some workplaces, monitoring is perceived as an unfair labour practice when it is used to measure individual, as opposed to group, performance. In particular, workers have taken exception to the use of monitoring to enforce compliance with performance standards that impose excessive workload demands. Electronic monitoring also can make the work process more impersonal by replacing a human supervisor with an electronic supervisor. In addition, the overemphasis on increased production may encourage workers to compete instead of cooperate with one another.
Various theoretical paradigms have been postulated to account for the possible stress-health effects of EPM (Amick and Smith 1992; Schleifer and Shell 1992; Smith et al. 1992b). A fundamental assumption made by many of these models is that EPM indirectly influences stress-health outcomes by intensifying workload demands, diminishing job control and reducing social support. In effect, EPM mediates changes in the psychosocial work environment that result in an imbalance between the demands of the job and the worker’s resources to adapt.
The impact of EPM on the psychosocial work environment is felt at three levels of the work system: the organization-technology interface, the job-technology interface and the human-technology interface (Amick and Smith 1992). The extent of work system transformation and the subsequent implications for stress outcomes are contingent upon the inherent characteristics of the EPM process; that is, the type of information gathered, the method of gathering the information and the use of the information (Carayon 1993). These EPM characteristics can interact with various job design factors and increase stress-health risks.
An alternative theoretical perspective views EPM as a stressor that directly results in strain independent of other job-design stress factors (Smith et al. 1992b; Carayon 1994). EPM, for example, can generate fear and tension as a result of workers being constantly watched by “Big Brother”. EPM also may be perceived by workers as an invasion of privacy that is highly threatening.
With respect to the stress effects of EPM, empirical evidence obtained from controlled laboratory experiments indicates that EPM can produce mood disturbances (Aiello and Shao 1993; Schleifer, Galinsky and Pan 1995) and hyperventilatory stress reactions (Schleifer and Ley 1994). Field studies have also reported that EPM alters job-design stress factors (for example, workload), which, in turn, generate tension or anxiety together with depression (Smith, Carayon and Miezio 1986; Ditecco et al. 1992; Smith et al. 1992b; Carayon 1994). In addition, EPM is associated with symptoms of musculoskeletal discomfort among telecommunication workers and data-entry office workers (Smith et al. 1992b; Sauter et al. 1993; Schleifer, Galinsky and Pan 1995).
The use of EPM to enforce compliance with performance standards is perhaps one of the most stressful aspects of this approach to work monitoring (Schleifer and Shell 1992). Under these conditions, it may be useful to adjust performance standards with a stress allowance (Schleifer and Shell 1992): a stress allowance would be applied to the normal cycle time, as is the case with other more conventional work allowances such as rest breaks and machine delays. Particularly among workers who have difficulty meeting EPM performance standards, a stress allowance would optimize workload demands and promote well-being by balancing the productivity benefits of electronic performance monitoring against the stress effects of this approach to work monitoring.
Beyond the question of how to minimize or prevent the possible stress-health effects of EPM, a more fundamental issue is whether this “Tayloristic” approach to work monitoring has any utility in the modern workplace. Work organizations are increasingly utilizing sociotechnical work-design methods, “total quality management” practices, participative work groups, and organizational, as opposed to individual, measures of performance. As a result, electronic work monitoring of individual workers on a continuous basis may have no place in high-performance work systems. In this regard, it is interesting to note that those countries (for example, Sweden and Germany) that have banned EPM are the same countries which have most readily embraced the principles and practices associated with high-performance work systems.
Role Clarity and Role Overload
Roles represent sets of behaviours that are expected of employees. To understand how organizational roles develop, it is particularly informative to see the process through the eyes of a new employee. Starting with the first day on the job, a new employee is presented with considerable information designed to communicate the organization’s role expectations. Some of this information is presented formally through a written job description and regular communications with one’s supervisor. Hackman (1992), however, states that workers also receive a variety of informal communications (termed discretionary stimuli) designed to shape their organizational roles. For example, a junior school faculty member who is too vocal during a departmental meeting may receive looks of disapproval from more senior colleagues. Such looks are subtle, but communicate much about what is expected of a junior colleague.
Ideally, the process of defining each employee’s role should proceed such that each employee is clear about his or her role. Unfortunately, this is often not the case and employees experience a lack of role clarity or, as it is commonly called, role ambiguity. According to Breaugh and Colihan (1994), employees are often unclear about how to do their jobs, when certain tasks should be performed and the criteria by which their performance will be judged. In some cases, it is simply difficult to provide an employee with a crystal-clear picture of his or her role. For example, when a job is relatively new, it is still “evolving” within the organization. Furthermore, in many jobs the individual employee has tremendous flexibility regarding how to get the job done. This is particularly true of highly complex jobs. In many other cases, however, role ambiguity is simply due to poor communication between either supervisors and subordinates or among members of work groups.
Another problem that can arise when role-related information is communicated to employees is role overload. That is, the role consists of too many responsibilities for an employee to handle in a reasonable amount of time. Role overload can occur for a number of reasons. In some occupations, role overload is the norm. For example, physicians in training experience tremendous role overload, largely as preparation for the demands of medical practice. In other cases, it is due to temporary circumstances. For example, if someone leaves an organization, the roles of other employees may need to be temporarily expanded to make up for the missing worker’s absence. In other instances, organizations may not anticipate the demands of the roles they create, or the nature of an employee’s role may change over time. Finally, it is also possible that an employee may voluntarily take on too many role responsibilities.
What are the consequences to workers in circumstances characterized by either role ambiguity, role overload or role clarity? Years of research on role ambiguity has shown that it is a noxious state which is associated with negative psychological, physical and behavioural outcomes (Jackson and Schuler 1985). That is, workers who perceive role ambiguity in their jobs tend to be dissatisfied with their work, anxious, tense, report high numbers of somatic complaints, tend to be absent from work and may leave their jobs. The most common correlates of role overload tend to be physical and emotional exhaustion. In addition, epidemiological research has shown that overloaded individuals (as measured by work hours) may be at greater risk for coronary heart disease. In considering the effects of both role ambiguity and role overload, it must be kept in mind that most studies are cross-sectional (measuring role stressors and outcomes at one point in time) and have examined self-reported outcomes. Thus, inferences about causality must be somewhat tentative.
Given the negative effects of role ambiguity and role overload, it is important for organizations to minimize, if not eliminate, these stressors. Since role ambiguity, in many cases, is due to poor communication, it is necessary to take steps to communicate role requirements more effectively. French and Bell (1990), in a book entitled Organization Development, describe interventions such as responsibility charting, role analysis and role negotiation. (For a recent example of the application of responsibility charting, see Schaubroeck et al. 1993). Each of these is designed to make employees’ role requirements explicit and well defined. In addition, these interventions allow employees input into the process of defining their roles.
When role requirements are made explicit, it may also be revealed that role responsibilities are not equitably distributed among employees. Thus, the previously mentioned interventions may also prevent role overload. In addition, organizations should keep up to date regarding individuals’ role responsibilities by reviewing job descriptions and carrying out job analyses (Levine 1983). It may also help to encourage employees to be realistic about the number of role responsibilities they can handle. In some cases, employees who are under pressure to take on too much may need to be more assertive when negotiating role responsibilities.
As a final comment, it must be remembered that role ambiguity and role overload are subjective states. Thus, efforts to reduce these stressors must consider individual differences. Some workers may in fact enjoy the challenge of these stressors. Others, however, may find them aversive. If this is the case, organizations have a moral, legal and financial interest in keeping these stressors at manageable levels.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."