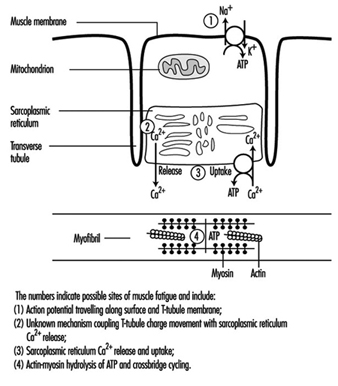
Physical activity may increase muscle strength and working capa-city through changes such as growth in muscle volume and increased metabolic capacity. Different activity patterns cause a variety of biochemical and morphological adaptations in the muscles. In general, a tissue must be active to remain capable of living. Inactivity causes atrophy, especially in muscle tissue. Sports medicine and scientific investigations have shown that various training regimes can produce very specific muscular changes. Strength training, which places strong forces on the muscles, increases the number of contractile filaments (myofibrils) and the volume of the sarcoplasmic reticulum (see figure 1). High-intensity exercise increases muscular enzyme activity. The fractions of glycolytic and oxidative enzymes are closely related to the work intensity. In addition, prolonged intense exercise increases the capillary density.
Figure 1. A diagrammatic representation of the major components of a muscle cell involved in excitation-contraction coupling as well as the site for ATP production, the mitochondrion.
Sometimes, too much exercise can induce muscle soreness, a phenomenon well known to everyone who has demanded muscular performance beyond his or her capacity. When a muscle is overused, first deteriorating processes set in, which are followed by reparative processes. If sufficient time for repair is allowed, the muscle tissue may end up with increased capacities. Prolonged overuse with insufficient time for repair, on the other hand, causes fatigue and impairs muscle performance. Such prolonged overuse may induce chronic degenerative changes in the muscles.
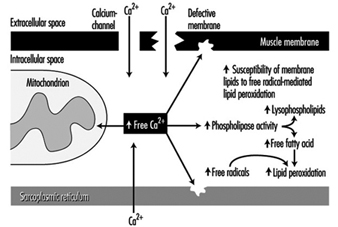
Other aspects of muscle use and misuse include the motor control patterns for various work tasks, which depend on force level, rate of force development, type of contraction, duration and the precision of the muscle task (Sjøgaard et al. 1995). Individual muscle fibres are “recruited” for these tasks, and some recruitment patterns may induce a high load on individual motor units even when the load on the muscle as a whole is small. Extensive recruitment of a particular motor unit will inevitably induce fatigue; and occupational muscle pain and injury may follow and could easily be related to the fatigue caused by insufficient muscle blood flow and intramuscular biochemical changes due to this high demand (Edwards 1988). High muscle tissue pressures may also impede muscle blood flow, which can reduce the ability of essential chemicals to reach the muscles, as well as the ability of the blood to remove waste products; this can cause energy crises in the muscles. Exercise can induce calcium to accumulate, and free radical formation may also promote degenerative processes such as the breakdown of muscle membrane and the impairment of normal metabolism (mitochondrial energy turnover) (figure 2). These processes may ultimately lead to degenerative changes in the muscle tissue itself. Fibres with marked degenerative characteristics have been found more frequently in muscle biopsies from patients with work-related chronic muscle pain (myalgia) than in normal subjects. Interestingly, the degenerated muscle fibres thus identified are “slow twitch fibres”, which connect with low-threshold motor nerves. These are the nerves normally recruited at low sustained forces, not high force related tasks. The perception of fatigue and pain may play an important role in preventing muscle injury. Protective mechanisms induce the muscles to relax and recover in order to regain strength (Sjøgaard 1990). If such biofeedback from the peripheral tissues is ignored, the fatigue and pain may eventually result in chronic pain.
Figure 2. A blow-up of the muscle membrane and structures inside the muscle in figure 2. The chain of events in the pathogenesis of calcium () induced damage in muscle cells is illustrated
Sometimes, after frequent overuse, various normal cellular chemical substances may not only cause pain themselves but may increase the response of muscular receptors to other stimuli, thereby lowering the threshold of activation (Mense 1993). The nerves which carry the signals from the muscles to the brain (sensory afferents) may thus be sensitized over time, which means that a given dose of substances which cause pain elicit a stronger excitation response. That is, the threshold of activation is reduced and smaller exposures may cause larger responses. Interestingly, the cells which normally serve as pain receptors (nociceptors) in uninjured tissue are silent, but these nerves may also develop ongoing pain activity which can persist even after the cause of the pain has terminated. This effect may explain chronic states of pain which are present after the initial injury has healed. When pain persists after healing, the original morphological changes in the soft tissues may be difficult to identify, even if the primary or initial cause of the pain is located in these peripheral tissues. Thus, the real “cause” of the pain may be impossible to trace.
Risk Factors and Preventive Strategies
Work-related risk factors of muscle disorders include repetition, force, static load, posture, precision, visual demand and vibration. Inappropriate work/rest cycles may be a potential risk factor for musculoskeletal disorders if sufficient recovery periods are not allowed before the next working period, thus never affording enough time for physiological rest. Environmental, sociocultural or personal factors may also play a role. Musculoskeletal disorders are multifactorial, and, in general, simple cause-effect relationships are difficult to detect. It is, however, important to document the extent to which occupational factors can be causally related to the disorders, since, only in the case of causality, the elimination or minimization of the exposure will help prevent the disorders. Of course, different preventive strategies must be implemented depending on the type of work task. In the case of high-intensity work the aim is to reduce force and work intensity, while for monotonous repetitive work it is more important to induce variation in the work. In short, the aim is optimization of the exposure.
Occupational Diseases
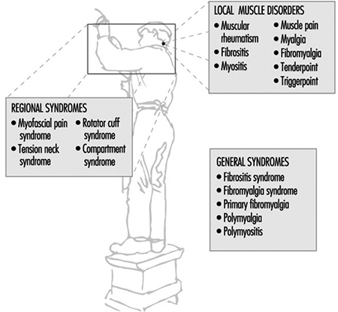
Work-related muscle pain is reported most frequently in the neck and shoulder area, the forearm and the low back. Although it is a major cause of sick-leave there is much confusion with regard to classifying the pain and specifying diagnostic criteria. Common terms which are used are given in three categories (see figure 3).
Figure 3. Classification of muscle diseases.
When muscular pain is assumed to be work-related, it can be classified into one of the following disorders:
- Occupational cervicobrachial disorders (OCD)
- Repetition strain injury (RSI)
- Cumulative trauma disorders (CTD)
- Overuse (injury) syndrome
- Work-related neck and upper-limb disorders.
The taxonomy of the work-related neck and upper-limb disorders clearly demonstrates that the aetiology includes external mechanical loads, which may well occur in the work place. Besides disorders in the muscle tissue itself, this category includes also disorders in other soft tissues of the musculoskeletal system. Of note is, that the diagnostic criteria may not allow to identify the location of the disorder specifically to one of these soft tissues. In fact it is likely that morphological changes at the musculo-tendinous junctions are related to the perception of muscle pain. This advocates the term fibromyalgia to be used among local muscle disorders. (See figure 3)
Unfortunately, different terms are used for essentially the same medical condition. In recent years, the international scientific community has focused increasingly on classification and diagnostic criteria for musculoskeletal disorders. A distinction is made between generalized and local or regional pain (Yunus 1993). Fibromyalgia syndrome is a generalized pain condition but is not considered to be work related. On the other hand, localized pain disorders are likely to be associated with specific work tasks. Myofascial pain syndrome, tension neck and rotator cuff syndrome are localized pain disorders that can be considered as work-related diseases.
