Rationale
Occupational settings are appropriate sites for the furtherance of such health-related aims as assessment, education, counseling and health promotion in general. From a public policy perspective, worksites provide an efficient locus for activities such as these, involving as they often do a far-ranging aggregation of individuals. Moreover, most workers are in a predictable work location for a significant portion of time almost every week. The worksite is usually a controlled environment, where individuals or groups can be exposed to educational programming or receive counseling without the distractions of a home setting or the often hurried atmosphere of a medical setting.
Health is an enabling function, that is to say, one that permits individuals to pursue other goals, including successful performance in their work roles. Employers have a vested interest in maximizing health because of its tight linkage with productivity at work, as to both quantity and quality. Thus, reducing the occurrence and burden of diseases that lead to absences, disability or sub-par job performance is a goal that warrants a high priority and considerable investment. Worker organizations, established to improve the welfare of members, also have an inherent interest in sponsoring programs that can improve health status and quality of life.
Sponsorship
Sponsorship by employers usually includes full or partial financial support of the program. However, some employers may support only planning or arranging for the actual health promotion activities for which individual workers must pay. Employer-sponsored programs sometimes provide employee incentives for participation, program completion, or successfully changing health habits. Incentives may include time off from work, financial rewards for participation or results, or recognition of achievement in reaching health-related goals. In unionized industries, particularly where workers are scattered among smaller workplaces too small to mount a program, health promotion programs may be designed and delivered by the labor organization. Although sponsorship of health education and counseling programs by employers or worker organizations commonly involves programs delivered at the worksite, they may take place in whole or in part at facilities in the community, whether run by government, non-profit-making or for-profit organizations.
Financial sponsorship needs to be complemented by employer commitment, on the part of top management and of middle management as well. Every employer organization has many priorities. If health promotion is to be viewed as one of these, it must be actively and visibly supported by senior management, both financially and by means of continuing to pay attention to the program, including the emphasizing of its importance in addressing employees, stockholders, senior managers and even the outside investment community.
Confidentiality and Privacy
While employee health is an important determinant of productivity and of the vitality of work organizations, health in itself is a personal matter. An employer or worker organization that wishes to provide health education and counseling must build into the programs procedures to ensure confidentiality and privacy. The willingness of employees to volunteer for work-related health education and counseling programs requires that employees feel that private health information will not be revealed to others without their permission. Of particular concern to workers and their representatives is that information obtained from health improvement programs not be utilized in any way in assessment of job performance or in managerial decisions about hiring, firing or advancement.
Needs Assessment
Program planning usually begins with a needs assessment. An employee survey is often performed to obtain information on such matters as: (a) self-reported frequency of health habits (e.g., smoking, physical activity, nutrition), (b) other health risks such as stress, hypertension, hypercholesterolemia, and diabetes, (c) personal priorities for risk reduction and health improvement, (d) attitude toward alternative program configurations, (e) preferred sites for health promotion programming, (f) willingness to participate in programmatic activities, and sometimes, (g) willingness to pay a portion of the cost. Surveys may also cover attitudes toward existing or potential employer policies, such as smoking bans or offering more nutritionally healthful fare in workplace vending machines or cafeterias.
The needs assessment sometimes includes analysis of the health problems of the employed group through examination of medical department clinical files, health care records, disability and worker’s compensation claims, and absenteeism records. Such analyses provide general epidemiological information on the prevalence and cost of different health problems, both somatic and psychological, allowing assessment of prevention opportunities from both the programmatic and financial point of view.
Program Structure
Results of needs assessments are considered in light of available monetary and human resources, past program experience, regulatory requirements and the nature of the workforce. Some of the key elements of a program plan that need to be clearly defined during a planning process are listed in figure 1. One of the key decisions is identifying effective modalities to reach the target population(s). For example, for a widely dispersed workforce, community-based programming or programming via telephone and mail may be the most feasible and cost-effective choice. Another important decision is whether to include, as some programmers do, retirees and spouses and children of employees in addition to the employees themselves.
Figure 1. Elements of a health promotion programme plan.

Responsibility for a worksite health promotion program can fall to any of a number of pre-existing departments, including the following: the medical or employee health unit; human resources and personnel; training; administration; fitness; employee assistance and others; or a separate health promotion department may be established. This choice is often very important to program success. A department with strong interest in doing its best for its clients, an appropriate knowledge base, good working relationships with other parts of the organization and the confidence of senior and line management has a very high likelihood of success in organizational terms. Employees’ attitudes toward the department in which the program is placed and their confidence in its integrity with particular reference to confidentiality of personal information may influence their acceptance of the program.
Topics
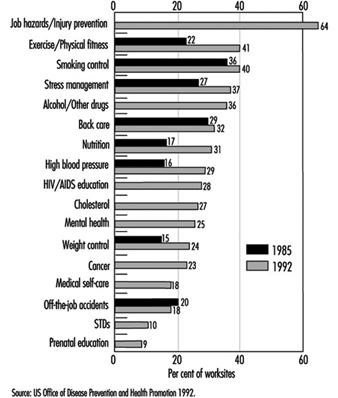
The frequency with which diverse health promotion topics is addressed based on surveys of private employers with 50 or more employees is shown in Figure 2. A review of results from comparable surveys in 1985 and 1992 reveals substantial increases in most areas. Overall in 1985, 66% of the worksites had at least one activity, whereas in 1992, 81% had one or more. Areas with the largest increases were those to do with exercise and physical fitness, nutrition, high blood pressure and weight control. Several topic areas queried for the first time in 1992 showed relatively high frequencies, including AIDS education, cholesterol, mental health and job hazards and injury prevention. Symptomatic of the expansion of areas of interest, the 1992 survey found that 36% of worksites provided education or other programs for abuse of alcohol and other drugs, 28% for AIDS, 10% for prevention of sexually-transmitted diseases, and 9% for prenatal education.
Figure 2. Health promotion information or activities offered by subject, 1985 and 1992.
A broad topic category increasingly included within worksite health promotion programming (16% of worksites in 1992) is health care mediated by self-help programs. Common to these programs are materials that address ways in which to treat minor health problems and to apply simple rules for judging the seriousness of various signs and symptoms in order to decide whether it may be advisable to seek professional help and with what degree of urgency.
Creating better-informed consumers of health care services is an allied program objective, and includes educating them such as how to choose a physician, what questions to ask the doctor, the pros and cons of alternative treatment strategies, how to decide whether and where to have a recommended diagnostic or therapeutic procedure, non-traditional therapies and patients’ rights.
Health Assessments
Regardless of mission, size and target population, multidimensional assessments of health are commonly administered to participating employees during the initial stages of the program and at periodic intervals thereafter. Data systematically collected usually cover health habits, health status, simple physiological measures, such as blood pressure and lipid profile, and (less commonly) health attitudes, the social dimensions of health, the use of preventive services, safety practices and family history. Computerized outputs, fed back to individual employees and aggregated for program planning, monitoring and evaluation, usually provide some absolute or relative risk estimates, which range from the absolute risk of having a heart attack during the ensuing ten-year period (or how an individual’s quantifiable risk of having a heart attack compares to the average risk for individuals of the same age and sex) to qualitative ratings of health and risks on a scale from poor to excellent. Individual recommendations are also commonly provided. For example, regular physical activity would be recommended for sedentary individuals, and more social contacts for an individual without frequent contact with family or friends.
Health assessments may be systematically offered at the time of hire or in association with specific programs, and thereafter at fixed intervals or with periodicity defined by age, sex and health risk status.
Counseling
Another common element of most programs is counseling to effect changes in such deleterious health habits as smoking, poor nutritional practices or high-risk sexual behavior. Effective methods exist to assist individuals to increase their motivation and readiness to make changes in their health habits, to help them along in the actual process of making changes, and to minimize backsliding, often termed recidivism. Group sessions led by a health professional or lay person with special training are often used to help individuals make changes, while the peer support to be found in the workplace can enhance results in areas such as smoking cessation or physical activity.
Health education for workers may include topics that can positively influence the health of other family members. For example, education might include programming on healthy pregnancy, the importance of breast feeding, parenting skills, and how to effectively cope with the health care and related needs of older relatives. Effective counseling avoids stigmatizing program participants who have difficulty making changes or who decide against making recommended lifestyle changes.
Workers with Special Needs
A significant proportion of a working population, particularly if it includes many older workers, will have one or more chronic conditions, such as diabetes, arthritis, depression, asthma or low back pain. In addition, a substantial subpopulation will be considered at high risk for a serious future health problem, for example cardiovascular disease due to elevation of risk factors such as total serum cholesterol, high blood pressure, smoking, significant obesity or high levels of stress.
These populations may account for a disproportionate amount of health services utilization, health benefits costs and lost productivity, but these effects can be attenuated through prevention efforts. Therefore, education and counseling programs targeted at these conditions and risks have become increasingly common. Such programs often utilize a specially trained nurse (or less commonly, a health educator or nutritionist) to help these individuals make and maintain necessary behavioral changes and work more closely with their primary care physician to utilize appropriate medical measures, especially as regards the use of pharmaceutical agents.
Program Providers
Providers of employer-sponsored or worker-sponsored health promotion programming are varied. In larger organizations, particularly with significant geographic concentrations of employees, existing full- or part-time personnel may be the principal program staff—nurses, health educators, psychologists, exercise physiologists and others. Staffing can also come from outside providers, individual consultants or organizations providing personnel in a wide range of disciplines. Organizations offering these services include hospitals, voluntary organizations (e.g., the American Heart Association); for-profit health promotion companies offering health screening, fitness, stress management, nutrition and other programs; and managed care organizations. Program materials may also come from any of these sources or they may be developed internally. Worker organizations sometimes develop their own programs for their members, or may provide some health promotion services in partnership with the employer.
Many education and training programs have been established to prepare both students and health professionals to plan, implement and evaluate worksite health promotion programs. Many universities offer courses in these subjects and some have a special “worksite health promotion” major or area of specialization. A large number of continuing education courses on how to work in a corporate setting, program management and advances in techniques are offered by public and private educational institutions as well as professional organizations. To be effective, providers must understand the specific context, constraints and attitudes associated with employment settings. In planning and implementing programs they should take into account policies specific to the type of employment and worksite, as well as the relevant labor relations issues, work schedules, formal and informal organizational structures, not to mention the corporate culture, norms and expectations.
Technology
Applicable technologies range from self-help materials that include traditional books, pamphlets, audiotapes or videotapes to programmed learning software and interactive videodiscs. Most programs involve interpersonal contact through groups such as classes, conferences and seminars or through individual education and counseling with an onsite provider, by telephone or even via computer link. Self-help groups may also be utilized.
Computer-based data collection systems are essential for program efficiency, serving a variety of management functions—budgeting and use of resources, scheduling, individual tracking, and both process and outcome evaluation. Other technologies could include such sophisticated modalities as a direct bio-computer linkage to record physiological measures—blood pressure or visual acuity for instance—or even the subject’s participation in the program itself (e.g., attendance at a fitness facility). Hand-held computer-based learning aids are being tested to assess their ability to enhance behavioral change.
Evaluation
Evaluation efforts run the gamut from anecdotal comments from employees to complex methodologies that justify publication in peer-reviewed journals. Evaluations may be directed towards a wide variety of processes and outcomes. For example, a process evaluation could assess how the program was implemented, how many employees participated and what they thought of it. Outcome evaluations may target changes in health status, such as the frequency or level of a health risk factor, whether self-reported (e.g., level of exercise) or objectively evaluated (e.g., hypertension). An evaluation may focus upon economic changes such as the use and cost of health care services or upon absenteeism or disability, whether this may be related to the job or not.
Evaluations may cover only program participants or they may cover all at-risk employees. The former sort of evaluation can answer questions relating to the efficacy of a given intervention but the latter answers the more important question as to the effectiveness with which risk factors in an entire population may have been reduced. While many evaluations focus on efforts to change a single risk factor, others address the simultaneous effects of multicomponent interventions. A review of 48 published studies assessing outcomes of comprehensive health promotion and disease prevention in the worksite found that 47 reported one or more positive health outcomes (Pelletier 1991). Many of these studies have significant weaknesses in design, methodology or analysis. Nonetheless, their near-unanimity with respect to positive findings, and the optimistic results of the best designed studies, suggest that real effects are in the desired direction. What is less clear is the reproducibility of effects in replicated programs, how long the initially observed effects endure, and whether their statistical significance translates into clinical significance. In addition, evidence of effectiveness is much stronger for some risk factors, such as smoking and hypertension, than for physical activity, nutritional practices and mental health factors, including stress.
Trends
Worksite health promotion programs are expanding beyond the traditional topics of controlling alcohol and drug abuse, nutrition, weight control, smoking cessation, exercise and stress management. Today, activities generally cover a wider variety of health topics, ranging from healthy pregnancy or the menopause to living with chronic health conditions such as arthritis, depression or diabetes. Increased emphasis is being placed on aspects of good mental health. For example, under the rubric of employer-sponsored programs may appear courses or other activities such as “improving interpersonal communications”, “building self-esteem”, “improving personal productivity at work and home”, or “overcoming depression”.
Another trend is to provide a wider range of health information and counseling opportunities. Individual and group counseling may be supplemented with peer counseling, computer-based learning, and use of interactive videodiscs. Recognition of multiple learning styles has led to a broader array of delivery modes to increase efficiency with a better match between individual learning styles and preferences and instructional approaches. Offering this diversity of approaches allows individuals to choose the setting, intensity and educational form that best fits their learning habits.
Today, health education and counseling are being increasingly offered to employees of larger organizations, including those who may work at distant locations with few co-workers and those that work at home. Delivery via mail and phone, when possible, can facilitate this broader reach. The advantage of these modes of program delivery is greater equity, with field staff employees not disadvantaged compared to their home office counterparts. One cost of greater equity is sometimes reduced interpersonal contact with health professionals on health promotion issues.
Healthy Policies
Recognition is increasing that organizational policy and social norms are important determinants of health and of the effectiveness of health improvement efforts. For example, limiting or banning smoking at the workplace can yield substantial declines in per capita cigarette consumption among smoking workers. A policy that alcoholic beverages will not be served at company functions lays out behavioral expectations for employees. Providing food that is low in fat and high in complex carbohydrates in the company cafeteria is another opportunity to help employees improve their health.
However, there is also concern that healthful organizational policies or expressed social normative beliefs about what constitutes good health may stigmatize individuals who wish to engage in certain unhealthy habits, such as smoking, or those who have a strong genetic predisposition to an unhealthy state, such as obesity. It is not surprising that most programs have higher participation rates by employees with “healthy” habits and lower risks.
Integration with Other Programs
The promotion of health has many facets. It appears that growing efforts are being made to seek a closer integration among health education and counseling, ergonomics, employee assistance programs, and particular health-oriented benefits like screening and fitness plans. In countries where employers can design their own health benefit plans or can supplement a government plan with defined benefits, many are offering clinical preventive services benefits, particularly screening and health-enhancing benefits such as membership in community health and fitness facilities. Tax policies that permit employers to deduct these employee benefits from taxes provide strong financial incentives for their adoption.
Ergonomic design is an important determinant of worker health and involves more than just the physical fit of the employee to the tools employed on the job. Attention should be directed to the overall fit of the individual to his or her tasks and to the overall working environment. For example, a healthful job environment requires a good match between job autonomy and responsibility and effective adaptations among individual work style, family needs and the flexibility of work requirements. Nor should the relationship between work stresses and individual coping capacities be left out of this account. In addition, health can be promoted by having workers, individually and in groups, help mould job content in ways that contribute to feelings of self-efficacy and achievement.
Employee assistance programs, which generically speaking include employer-sponsored professionally directed activities that provide assessment, counseling and referral to any employee for personal problems, should have close ties with other health promoting programs, functioning as a referral source for the depressed, the overstressed and the preoccupied. In return, employee assistance programs can refer appropriate workers to employer-sponsored stress management programs, to physical fitness programs that help relieve depression, to nutritional programs for those overweight, underweight, or simply with bad nutrition, and to self-help groups for those who lack social support.
Conclusion
Worksite health promotion has come of age owing largely to incentives for employer investment, positive reported results for most programs, and increasing acceptance of worksite health promotion as an essential part of a comprehensive benefit plan. Its scope has broadened considerably, reflecting a more encompassing definition of health and an understanding of the determinants of individual and family health.
Well-developed approaches to program planning and implementation exist, as does a cadre of well-trained health professionals to staff programs and a wide variety of materials and delivery vehicles. Program success depends on individualizing any program to the corporate culture and to the health promotion opportunities and organizational constraints of a particular worksite. Results of most evaluations have supported movement toward stated program objectives, but more evaluations using scientifically valid designs and methods are needed.