- You are here:
-
Home

-
Contents
-
Part III. Management & Policy
-
Resources, Institutional, Structural and Legal
- Regional and National Examples

Regional and National Examples
Occupational Health and Safety: The European Union
The European Union (EU) today exercises a major influence on worldwide health and safety law and policy. In 1995, the Union comprised the following Member States: Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Luxembourg, Netherlands, Portugal, Spain, Sweden and the United Kingdom. It will probably expand in years to come.
The forerunner of the Union, the European Community, was created in the 1950s by three treaties: The European Coal and Steel Community Treaty (ECSC) signed in Paris in 1951, and the European Economic Community (EEC) and European Atomic Energy Community (EAEC) Treaties signed in Rome in 1957. The European Union was formed with the entry into force of the Maastricht Treaty (concluded in 1989) on 1 January 1992.
The Community has four institutions, namely, the Commission, the Council, the Parliament and the European Court of Justice. They derive their powers from the treaties.
The Structures
The Commission
The Commission is the Community’s executive body. It is responsible for initiating, proposing and implementing Community policy, and if a Member State fails to fulfil its obligations under the treaties, the Commission can take proceedings against that Member State in the European Court of Justice.
It is composed of seventeen members appointed by the governments of Member States for a renewable four-year period. Each Commissioner is responsible for a portfolio and has authority over one or more Directorates General. One such Directorate General, DG V, is concerned with Employment, Industrial Relations and Social Affairs, and it is from within this Directorate General (DG V/F) that health and safety and public health policies are both initiated and proposed. The Commission is assisted in its health and safety law and policy-making role by the Advisory Committee on Safety, Hygiene and Health Protection at Work and the European Foundation for the Improvement of Living and Working Conditions.
Advisory Committee on Safety, Hygiene and Health Protection at Work
The Advisory Committee was established in 1974 and is chaired by the Commissioner responsible for the Directorate-General for Employment, Industrial Relations and Social Affairs. It consists of 96 full members: two representatives each of government, trade unions, and employers’ organizations from each Member State.
The role of the Advisory Committee is to “assist the Commission in the preparation and implementation of activities in the fields of safety, hygiene and health protection at work”. Because of its constitution and membership, the Advisory Committee is much more important and pro-active than its title suggests, so that, over the years, it has had a significant influence on strategic policy development, acting alongside the European Parliament and the Economic and Social Committee. More specifically, the Committee is responsible for the following matters within its general frame of reference:
- conducting exchanges of views and experience regarding existing or planned regulations
- contributing towards the development of a common approach to problems existing in the fields of safety, hygiene and health protection at work and towards the choice of Community priorities as well as measures necessary for implementing them
- drawing the Commission’s attention to areas in which there is an apparent need for the acquisition of new knowledge and for the implementation of appropriate educational and research projects
- defining, within the framework of Community action programmes, and in cooperation with the Mines Safety and Health Commission, (i) the criteria and aims of the campaign against the risk of accidents at work and health hazards within the undertaking; and (ii) methods enabling undertakings and their employees to evaluate and to improve the level of protection
- contributing towards keeping national administrations, trade unions and employers’ organizations informed of Community measures in order to facilitate their cooperation and to encourage initiatives promoted by them aiming at exchanges of experience and at laying down codes of practice
- submitting opinions on proposals for directives and on all measures proposed by the Commission which are of relevance to health and safety at work.
In addition to these functions, the Committee prepares an annual report, which the Commission then forwards to the Council, the Parliament and the Economic and Social Committee.
The Dublin Foundation
The European Foundation for the Improvement of Living and Working Conditions, located in Dublin, was established in 1975 as a specialized, autonomous Community body. The Foundation is primarily engaged in applied research in the areas of social policy, the application of new technologies, and the improvement and protection of the environment, in an effort to identify, cope with and forestall problems in the working environment.
European Agency for Health and Safety at the Workplace
The European Council has recently established the European Agency for Health and Safety at the Workplace in Bilbao, Spain, which is responsible for collating and disseminating information in its sector of activities. It will also organize training courses, supply technical and scientific support to the Commission and forge close links with specialized national bodies. The agency will also organize a network system with a view to exchanging information and experiences between Member States.
The European Parliament
The European Parliament exercises an increasingly important consultative role during the Community’s legislative process, controls a part of the Community’s budget jointly with the Council, approves Community Association agreements with non-member countries and treaties for the accession of new Member States, and is the Community’s supervisory body.
The Economic and Social Committee
The Economic and Social Committee is an advisory and consultative body which is required to give its opinion on a range of social and vocational issues, including health and safety at work. The Committee draws its membership from three main groups: employers, workers and an independant group comprising members with a wide spectrum of interests including professional, business, farming, the cooperative movement and consumer affairs.
Legal Instruments
There are four main instruments available to the Community legislator. Article 189 of the EEC Treaty as amended provides that “In order to carry out their task and in accordance with the provisions of this Treaty, the European Parliament acting jointly with the Council and the Commission shall make regulations and issue directives, take decisions, make recommendations or deliver opinions.”
Regulations
It is stated that “A regulation shall have general application. It shall be binding in its entirety and directly applicable in all Member States.” Regulations are directly enforceable in Member States. There is no need for further implementation. Indeed, it is not permissible for legislatures to consider them with a view to that end. In the field of health and safety at work, regulations are rare and those that have been made are administrative in nature.
Directives and decisions
It is stated that “A directive shall be binding, as to the result to be achieved, upon each Member State to which it is addressed, but shall leave to the national authorities the choice of form and methods.” Directives are instructions to Member States to enact laws to achieve an end result. In practice, directives are used mainly to bring about the harmonization or approximation of national laws in accordance with Article 100. They are therefore the most appropriate and commonly used instruments for occupational health and safety matters. In relation to decisions, it is stated that “A decision shall be binding in its entirety upon those to whom it is addressed.”
Recommendations and opinions
Recommendations and opinions have no binding force but are indicative of policy stances.
Policy
The European Communities made a decision in the mid-1980s to press ahead strongly with harmonization measures in the field of health and safety. Various reasons have been put forward to explain the developing importance of this area, of which four may be considered to be significant.
First, it is said that common health and safety standards assist economic integration, since products cannot circulate freely within the Community if prices for similar items differ in various Member States because of variable health and safety costs imposed on business. Second, 10 million people a year are the victims of, and 8,000 people a year die from, workplace accidents (out of a workforce which numbered 138 million people in 1994). These grim statistics give rise to an estimated bill of ECU 26,000 million paid in compensation for occupational accidents and diseases annually, whilst in Britain alone the National Audit Office in their Report Enforcing Health and Safety in the Workplace estimated that the cost of accidents to industry and the taxpayer is £10 billion per year. It is argued that a reduction of the human, social and economic costs of accidents and ill-health borne by this workforce will not only bring about a huge financial saving but will also bring about a significant increase in the quality of life for the whole Community. Third, the introduction of more efficient work practices is said to bring with it increased productivity, lower operational costs and better industrial relations.
Finally, it is argued that the regulation of certain risks, such as those arising from massive explosions, should be harmonized at a supranational level because of the scale of resource costs and (an echo of the first reason canvassed above) because any disparity in the substance and application of such provisions produces distortions of competition and affects product prices.
Much impetus was given to this programme by the campaign organized by the Commission in collaboration with the twelve Member States in the European Year of Health and Safety, which took place during the 12-month period commencing 1 March 1992. This campaign sought to reach the whole of the Community’s working population, particularly targeting high-risk industries and small and medium-sized enterprises.
Each of the founding treaties laid the basis for new health and safety laws. The EEC Treaty, for example, contains two provisions which are, in part at least, devoted to the promotion of health and safety, namely articles 117 and 118.
Community Charter of the Fundamental Social Rights of Workers
To meet the challenge, a comprehensive programme of measures was proposed by the Commission in 1987 and adopted by the Council in the following year. This programme contained a series of health and safety measures grouped under the headings of safety and ergonomics, health and hygiene, information and training, initiatives concerning small and medium enterprises, and social dialogue. Added impetus to these policies was provided by the Community Charter of the Fundamental Social Rights of Workers, adopted in Strasbourg in December 1989 by 11 of the 12 Member States (the United Kingdom abstained).
The Social Charter, as agreed in December 1989, covers 12 categories of “fundamental social rights” among them are several of practical relevance here:
- Improvement of living and working conditions. There should be improvement in working conditions, particularly in terms of limits on working time. particular mention is made of the need for improved conditions for workers on part-time or seasonal contracts and so on.
- Social protection. Workers, including the unemployed, should receive adequate social protection and social security benefits.
- Information, consultation and participation for workers. This should apply especially in multinational companies and in particular at times of restructuring, redundancies or the introduction of new technology.
- Health protection and safety at the workplace.
- Protection of children and adolescents. The minimum employment age should be no lower than the minimum school-leaving age, and in any case not lower than 15 years. The hours which those aged under 18 can work should be limited, and they should not generally work at night.
- Elderly persons. Workers should be assured of resources providing a decent standard of living upon retirement. Others should have sufficient resources and appropriate medical and social assistance.
- Disabled people. All disabled people should have additional help towards social and professional integration.
Member States are given responsibility in accordance with national practices for guaranteeing the rights in the Charter and implementing the necessary measures, and the Commission is asked to submit proposals on areas within its competence.
Since 1989, it has become clear that within the Community as a whole there is much support for the Social Charter. Undoubtedly, Member States are anxious to show that workers, children and older workers should benefit from the Community as well as shareholders and managers.
The 1989 Framework Directive
The principles in the Commission’s health and safety programme were set out in another “Framework Directive” (89/391/EEC) on the introduction of measures to encourage improvements in the safety and health of workers at work. This makes a significant step forward from the approach witnessed in the earlier “Framework Directive” of 1980. In particular, the 1989 Directive, while endorsing and adopting the approach of “self-assessment”, also sought to establish a variety of basic duties, especially for the employer. Furthermore, the promotion of “social dialogue” in the field of health and safety at work was explicitly incorporated into detailed provisions in the 1989 Directive, introducing significant requirements for information, consultation and participation for workers and their representatives at the workplace. This 1989 Directive required compliance by 31 December 1992.
The Directive contains re-stated general principles concerning, in particular, the prevention of occupational risks, the protection of safety and health and the informing, consultation and training of workers and their representatives, as well as principles concerning the implementation of such measures. This measure constituted a first attempt to provide an overall complement to the technical harmonization directives designed to complete the internal market. The 1989 Directive also brought within its scope the provisions of the 1980 Framework Directive on risks arising from use at work of chemical, physical and biological agents. It parallels the ILO Convention concerning Occupational Safety and Health, 1981 (No. 155) and its accompanying Recommendation (No. 161).
The overall objectives of the 1989 Directive may be summarized as being:
- humanization of the working environment
- accident prevention and health protection at the workplace
- to encourage information, dialogue and balanced participation on safety and health by means of procedures and instruments
- to promote throughout the Community, the harmonious development of economic activities, a continuous and balanced expansion and an accelerated rise in the standard of living
- to encourage the increasing participation of management and labour in decisions and initiatives
- to establish the same level of health protection for workers in all undertakings, including small and medium-sized enterprises, and to fulfil the single market requirements of the Single European Act 1986; and
- the gradual replacement of national legislation by Community legislation.
General duties placed upon the employer include duties of awareness, duties to take direct action to ensure safety and health, duties of strategic planning to avoid risks to safety and health, duties to train and direct the workforce, duties to inform, consult and involve the workforce, and duties of recording and notification.
The Directive provided similar safeguards for small and medium-sized enterprises. It is stated, for example, that the size of the undertaking and/or establishment is a relevant matter in relation to determining the sufficiency of resources for dealing with the organization of protective and preventive measures. It is also a factor to be considered in relation to obligations concerning first aid, fire fighting and evacuation of workers. Furthermore, the Directive included a power for differential requirements to be imposed upon varying sizes of undertakings as regards documentation to be provided. Finally, in relation to the provision of information, it is stated that national measures “may take account, inter alia, of the size of the undertaking and/or establishment”.
Under the umbrella of the 1989 Directive, a number of individual directives have also been adopted. In particular, “daughter” directives have been adopted on minimum safety and health requirements for the workplace, for the use of work equipment, for the use of personal protective equipment, for the manual handling of loads, and for work with display screen equipment.
The following Directives have also been adopted:
- Council Directive of 20 December 1993 concerning the minimum safety and health requirements for work on board fishing vessels (93/103/EEC)
- Council Directive of 12 October 1993 amending Directive 90/679/EEC on the protection of workers from risks related to exposure to biological agents at work (93/88/EEC)
- Council Directive of 3 December 1992 on the minimum requirements for improving the safety and health protection of workers in surface and underground mineral-extracting industries (92/104/EEC)
- Council Directive of 3 November 1992 on the minimum requirements for improving the safety and health protection of workers in mineral-extracting industries that involve drilling (92/91/EEC)
- Council Directive of 19 October 1992 on the introduction of measures to encourage improvements in the safety and health at work of pregnant workers and workers who have recently given birth or who are breast-feeding (92/85/EEC)
- Council Directive of 24 June 1992 on the minimum requirements for the provision of safety and/or health signs at work (92/58/EEC)
- Council Directive of 24 June 1992 on the implementation of minimum safety and health requirements at temporary or mobile construction sites (92/57/EEC)
- Council Directive of 31 March 1992 on the minimum safety and health requirements for improved medical treatment on board vessels (92/29/EEC)
- Council Directive of 23 April 1990 on the contained use of genetically modified micro-organisms. (90/219/ EEC)
Since the passage of the Maastricht Treaty, further measures have been passed, namely: a Recommendation on a European schedule of industrial diseases; a directive on asbestos; a directive on safety and health signs at the workplace; a directive on medical assistance on board vessels; directives on health and safety protection in the extractive industries; and a directive introducing measures to promote improvements in the travel conditions of workers with motor disabilities.
The Single Market
The original Article 100 has been replaced by a new provision in the Treaty of European Union. The new Article 100 ensures that the European Parliament and the Economic and Social Committee must be consulted in all cases and not simply when the implementation of a directive would involve the amendment of legislation in one or more Member States.
Legislation Guaranteeing Benefits for Workers in China
The occupational safety and health of workers has been an important aspect of legislation laid down in the form of the Labour Law promulgated in July 1994. To urge enterprises into the market system, and in the meantime to protect the rights of labourers, in-depth reforms in the system of labour contracts and wage distribution and in social security have been major priorities in the government agenda. Establishing a uniform welfare umbrella for all workers regardless of the ownership of the enterprises is one of the goals, which also include unemployment coverage, retirement pension systems, and occupational disease and injuries compensation insurance. The Labour Law requires that all employers pay a social security contribution for their workers. Part of the legislation, the draft of the Occupational Disease Prevention and Control Law, will be an area of the Labour Law to which major attention has been devoted in order to regulate the behaviour and define the responsibilities of employers in controlling occupational hazards, while at the same time giving more rights to workers in protecting their own health.
Cooperation Between Governmental Agencies and the All-China Federation of Trade Unions in Policy Making and Legislation Enforcement
The Ministry of Public Health (MOPH), the Ministry of Labour (MOL), and the All-China Federation of Trade Unions (ACFTU) have a long history of cooperation. Many important policies and activities have resulted from their joint efforts.
The current division of responsibility between the MOPH and the MOL in occupational safety and health is as follows:
- From the preventive medical point of view, the MOPH oversees industrial hygiene and occupational health, enforcing national health inspection.
- The focus of the MOL is on engineering the control of occupational hazards and on the organization of labour, as well as overseeing occupational safety and health and enforcing national labour inspection (figure 1) (MOPH and MOL 1986).
Figure 1. Governmental organization and division of responsibility for occupational health and safety
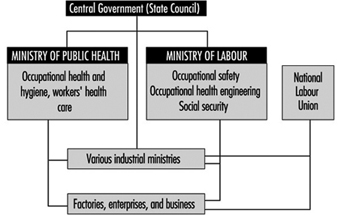
It is difficult to draw a line between the responsibilities of the MOPH and the MOL. It is expected that further cooperation will focus on enhancing enforcement of occupational safety and health regulations.
The ACFTU has been increasingly involved in safeguarding workers’ rights. One of the important tasks of the ACFTU is to promote the establishment of trade unions in foreign-funded enterprises. Only 12% of overseas-funded enterprises have established unions.
Case Study: Exposure Standards in Russia
Comparison of the Philosophical Bases of Maximum Allowable Concentrations (MACs) and Threshold Limit Values (TLVs)
Rapid development of chemistry and wide usage of chemical products require specific toxicological studies and hazards evaluation with regard to long-term and combined effects of chemical substances. The setting of standards for chemicals in the working environment is being conducted by occupational hygienists in many countries of the world. Experience on the matter has been accumulated in international and multilateral organizations such as the International Labour Organization, the World Health Organization, the United Nations Environment Programme, the Food and Agriculture Organization and the European Union.
Much has been done in this field by Russian and American scientists. In 1922 studies were launched in Russia to set up standards for chemicals in the air of indoor work areas, and the first maximum allowable concentration (MAC) value for sulphur-containing gas was adopted. By 1930 only 12 MAC values were established, whereas by 1960 their number reached 181.
The American Conference of Governmental Industrial Hygienists (ACGIH) started its work in 1938, and the first threshold limit values (TLVs) list was published in 1946 for 144 substances. The TLVs are to be interpreted and used only by the specialists in this field. If a TLV has been included in the safety standards (the so-called standards of national consensus) and the federal standards, it becomes legal.
At present more than 1,500 MAC values have been adopted for workplace air in Russia. More than 550 TLVs for chemical substances have been recommended in the United States.
Analysis of hygienic standards made in 1980–81 showed that 220 chemicals of the MAC list (Russia) and the TLV list (United States) had the following differences: from two- to fivefold differences were found in 48 substances (22%), 42 substances had five- to ten-fold differences, and 69% substances (31%) had more than ten-fold differences. Ten per cent of the recommended TLVs were 50 times higher than the MAC values for the same substances. The MAC values, in turn, were higher than the TLVs for 16 substances.
The largest divergence of standards occurs in the class of chlorinated hydrocarbons. Analysis of the TLV list adopted in 1989–90 showed a trend toward a reduction of the earlier recommended TLVs compared with the MAC values for chlorinated hydrocarbons and some solvents. Differences among the TLVs and the MACs for the majority of metal aerosols, metalloids, and their compounds were insignificant. The divergences for irritant gases were also slight. The TLVs for lead, manganese and tellurium compared with their MAC analogues disagreed 15, 16 and 10 times, respectively. The differences for acetic aldehyde and formaldehyde were the most extreme—36 and 6 times, respectively. In general, the MAC values adopted in Russia are lower than the TLVs recommended in the United States.
These divergences are explained by the principles used in the development of hygienic standards in the two countries and by the way of these standards are applied to protect workers’ health.
A MAC is a hygienic standard used in Russia to denote a concentration of a harmful substance in the air of the workplace which will not cause, in the course of work for eight hours daily or for any other period of time (but not more than 41 hours per week throughout the working life of an individual), any disease or deviation in the health status as detectable by the available methods of investigation, during the working life or during the subsequent life of the present and next generations. Thus, the concept used in defining the MAC does not allow for any adverse effect on a worker or his or her progeny. The MAC is a safe concentration.
A TLV is the concentration (in air) of a material to which most workers can be exposed daily without adverse effect. These values are established (and revised annually) by the ACGIH and are time-weighted concentrations for a seven- or eight-hour workday and 40-hour workweek. For most materials the value may be exceeded, to a certain extent, provided there are compensatory periods of exposure below the value during the workday (or in some cases the week). For a few materials (mainly those that produce a rapid response) the limit is given as ceiling concentration (i.e., a maximum allowable concentration) that should never be exceeded. The ACGIH states that TLVs should be used as guides in the control of health hazards, and are not fine lines between safe and dangerous concentrations, nor are they a relative index of toxicity.
The TLV definition also contains the principle of inadmissibility of harmful impact. However, it does not cover all of the working population, and it is admitted that a small percentage of workers may manifest health changes or even occupational pathologies. Thus TLVs are not safe for all workers.
According to ILO and WHO experts, these divergences are the result of different scientific approaches to a number of interrelated factors including the definition of an adverse health effect. Therefore, different initial approaches for the control of chemical hazards lead to different methodological principles, essential points of which are presented below.
The main principles of setting hygienic standards for dangerous substances in the air of workplaces in Russia compared with those in the United States are summarized in table 1. Of special importance is the theoretical concept of the threshold, the basic difference between the Russian and the American specialists that underlies their approaches to setting standards. Russia accepts the concept of a threshold for all types of dangerous effects of chemical substances.
Table 1. A comparison of some ideological bases for Russian and American standards
|
Russia (MACs) |
United States (TLVs) |
|
Threshold nature of all kinds of adverse effects. Changes of specific and non-specific factors regarding the criteria of harmful impact are evaluated. |
No recognition of threshold for mutagens and some carcinogens. Changes of specific and non-specific factors depending on “dose-effect ”and “dose-response” relationship are evaluated. |
|
Priority of medical and biological factors over technological and economic criteria. |
Technological and economic criteria prevail. |
|
Prospective toxicological assessment and interpretation of standards before the commercialization of chemical products. |
Retrospective setting of standards. |
However, the recognition of a threshold for some types of effects requires the distinction between injurious and non-injurious effects produced by chemical substances. Consequently, the threshold of unhealthy effects established in Russia is the minimal concentration (dose) of a chemical that causes changes beyond the limits of physiological adaptive responses or produces latent (temporarily compensated) pathologies. In addition, various statistical, metabolic, and toxico-kinetic criteria of adverse effects of chemicals are used to differentiate between the processes of physiological adaptation and pathological compensation. Pathomorphological changes and narcotic symptoms of earliest impairment have been suggested in the United States for the identification of injurious and non-injurious effects. It means that more sensitive methods have been chosen for the toxicity evaluation in Russia than those in the United States. This, therefore, explains the generally lower levels of MACs compared to TLVs. When the detection criteria for injurious and non-injurious effects of chemicals are close or practically coincide, as in the case of irritant gases, the differences in standards are not so significant.
The evolution of toxicology has put into practice new methods for the identification of minor changes in tissues. These are enzyme induction in the smooth endoplastic reticular hepatic tissue and reversible hypertrophy of the liver. These changes may appear after exposure to low concentrations of many chemical substances. Some researchers consider these to be adaptive reactions, while others interpret them as early impairments. Today, one of the most difficult tasks of toxicology is obtaining data that show whether enzyme disturbances, nervous system disorders and changes in behavioural responses are the result of deteriorated physiological functions. This would make it possible to predict more serious and/or irreversible impairments in case of long-term exposure to dangerous substances.
Special emphasis is placed on the differences in the sensitivity of methods used for the establishment of MACs and TLVs. Very sensitive methods of conditioned reflexes applied to studies of the nervous system in Russia have been found to be the main cause of divergences between the MACs and the TLVs. However, the use of this method in the process of hygienic standardization is not obligatory. Numerous methods of different sensitivities are normally used for the developing of a hygienic standard.
A great number of studies conducted in the United States in connection with the setting-up of exposure limits are aimed at examining the transformation of industrial compounds in the human body (routes of exposure, circulation, metabolism, removal, etc.). Methods of chemical analysis used to establish the values of TLVs and MACs also cause divergences due to their different selectivities, accuracies and sensitivities. An important element usually taken into consideration by OSHA in the standardization process in the United States is the “technical attainability” of a standard by industry. As a result, some standards are recommended on a basis of the lowest presently existing concentrations.
MAC values in Russia are established on a basis of the prevalence of medico-biological characteristics, whereas the technological attainability of a standard is practically ignored. This partly explains lower MAC values for some chemical substances.
In Russia MAC values are assessed in toxicological studies before a substance is authorized for industrial use. A tentative safe exposure level is established during the laboratory synthesis of a chemical. The MAC value is established after animal experiments, at the design stage of the industrial process. The correction of the MAC value is carried out after evaluation of working conditions and workers’ health when the substance is used in industry. Most of the safe levels of exposure in Russia have been recommended after experiments on animals.
In the United States a final standard is established after a chemical substance has been introduced in industry, because the values of permissible levels of exposure are based on the assessment of health. As long as the differences of principle between the MACs and the TLVs remain, it is unlikely to expect the convergence of these standards in the near future. However, there is a trend towards the reduction of some TLVs that makes this not so impossible as it may seem.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."