- You are here:
-
Home

-
Contents (2)
-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
-
Storage
- Yassi, Annalee

Grady-van den Nieuwboer, Joke J.H.
Address: Roessingh Rehabilitation Centre, Haaksbergen
Country: Netherlands
Past position(s): Lecturer of Physical Ergonomics and Research Staff Member, Ergonomics Department, University Twente te Enschede, Netherlands; Ad Interim Manager of the OT Department of the Rehabilitation Centre "het Roessingh"; Enschede, Netherlands; Consultant in design for the disabled; Project Manager Research, IRON Instituut voor Research, Ontwikkeling en Nascholing;
Education: BSc, 1972, Dutch Institute for Occupational Therapy, Amsterdam; MSc, 1989, University of Groningen
Areas of interest: Technical design and aids; rehabilitation
Workers with Special Needs
Designing for Disabled Persons is Designing for Everyone
There are so many products on the market that readily reveal their unfitness for the general population of users. What evaluation should one make of a doorway too narrow to comfortably accommodate a stout person or pregnant woman? Shall its physical design be faulted if it satisfies all relevant tests of mechanical function? Certainly such users cannot be regarded as disabled in any physical sense, since they may be in a state of perfect health. Some products need considerable handling before one can force them to perform as desired—certain inexpensive can openers come, not altogether trivially, to mind. Yet a healthy person who may experience difficulty operating such devices need not be considered disabled. A designer who successfully incorporates considerations of human interaction with the product enhances the functional utility of his or her design. In the absence of good functional design, people with a minor disability may find themselves in the position of being severely hampered. It is thus the user-machine interface that determines the value of design for all users.
It is a truism to remind oneself that technology exists to serve human beings; its use is to enlarge their own capabilities. For disabled persons, this enlargement has to be taken some steps further. For instance in the 1980s, a good deal of attention was paid to the design of kitchens for disabled people. The experience gained in this work penetrated design features for “normal” kitchens; the disabled person in this sense may be considered a pioneer. Occupationally-induced impairments and disabilities—one has but to consider the musculoskeletal and other complaints suffered by those confined to sedentary tasks so common in the new workplace—similarly call for design efforts aimed not only also preventing the recurrence of such conditions, but at the development of user-compatible technology adapted to the needs of workers already affected by work-related disorders.
The Broader Average Person
The designer should not focus on a small, unrepresentative population. Among certain groups it is most unwise to entertain assumptions concerning similarities among them. For example, a worker injured in a certain way as an adult may not necessarily be anthropometrically quite so different from an otherwise comparable, healthy person, and may be considered as part of the broad average. A young child so injured will display a considerably different anthropometry as an adult since his muscular and mechanical development will be steadily and sequentially influenced by preceding growth stages. (No conclusions as to comparability as adults ought to be ventured as regards the two cases. They must be regarded as two distinct, specific groups, only the one being included among the broad average.) But as one strives for a design suitable for, say, 90% of the population, one should exert fractionally greater pains to increase this margin to, say, 95%, the point being that in this way the need for design for specific groups can be reduced.
Another way to approach design for the broader average population is to produce two products, each one designed roughly to fit the two percentile extremes of human differences. Two sizes of chair, for instance, might be built, the one with brackets allowing it to be adjusted in height from 38 to 46 cm, and the other one from 46 to 54 cm; two sizes of pliers already exist, one fitting larger and average sizes of men’s hands and the other fitting average women’s hands and hands of smaller men.
It would be a well-advised company policy to reserve annually a modest amount of money to have worksites analysed and made more suitable for workers, a move that would prevent illness and disability due to excessive physical load. It also increases the motivation of workers when they understand that management is actively trying to improve their work environment, and more impressively so when elaborate measures sometimes have to be undertaken: thorough work analysis, the construction of mock-ups, anthropometrical measurements, and even the specific design of units for the workers. In a certain company, in fact, the conclusion was that the units should be redesigned at every worksite because they caused physical overload in the form of too much standing, there were unsuitable dimensions associated with the seated positions, and there were other deficiencies as well.
Costs, Benefits and Usability of Design
Cost/benefit analyses are developed by ergonomists in order to gain insight into the results of ergonomic policies other than those that are economic. In the present day, evaluation in the industrial and commercial realms includes the negative or positive impact of a policy on the worker.
Methods of evaluating quality and usability are currently the subject of active research. The Rehabilitation Technology Useability Model (RTUM), as shown in figure 1, can be utilized as a model for evaluating the usability of a product within rehabilitation technology and to illuminate the various aspects of the product which determine its usability.
Figure 1. The Rehabilitation Technology Useability Model (RTUM)
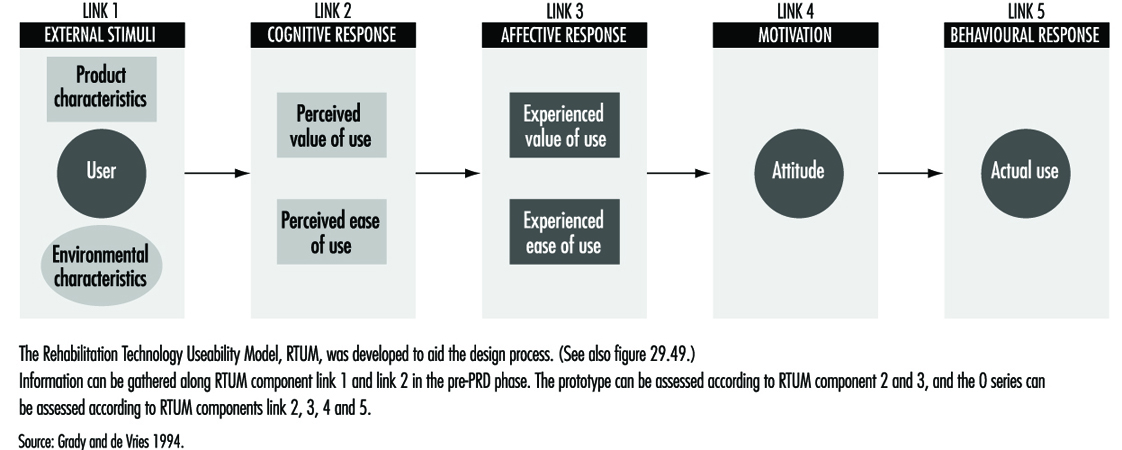
From the strictly economic point of view, the costs of creating a system in which a given task can be performed or in which a certain product can be made can be specified; it scarcely needs mentioning that in these terms each company is interested in a maximum return on its investment. But how can the real costs of task performance and product manufacturing in relation to financial investment be determined when one takes into account the varying exertions of workers’ physical, cognitive and mental systems? In fact, the judging of human performance itself is, among other factors, based on the workers’ perception of what has to be done, their view of their own value in doing it, and their opinion of the company. It is actually the intrinsic satisfaction with work that is the norm of value in this context, and this satisfaction, together with the aims of the company, constitute one’s reason for performing. Worker well-being and performance are thus based on a wide spectrum of experiences, associations and perceptions that determine attitudes towards work and the ultimate quality of performance—an understanding upon which the RTUM model is predicated.
If one does not accept this view, it becomes necessary to regard investment only in relation to doubtful and unspecified results. If ergonomists and physicians wish to improve the work environment of disabled people—to produce more from machine operations and enhance the usability of the tools used—they will encounter difficulties in finding ways to justify the financial investment. Typically, such justification has been sought in savings realized by prevention of injury and illness due to work. But if the costs of illness have been borne not by the company but by the state, they become financially invisible, so to speak, and are not seen as work-related.
Nevertheless, the awareness that investment in a healthy working environment is money well spent has been growing with the recognition that the “social” costs of incapacities are translatable in terms of ultimate costs to a country’s economy, and that value is lost when a potential worker is sitting about at home making no contribution to society. Investing in a workplace (in terms of adapting a work station or providing special tools or perhaps even help in personal hygiene) can not only reward a person with job satisfaction but can help make him or her self-sufficient and independent of social assistance.
Cost/benefit analyses can be carried out in order to determine whether special intervention in the workplace is justified for disabled persons. The following factors represent sources of data that would form the object of such analyses:
1. Personnel
- Absence. Will the disabled worker have a satisfactory attendance record?
- Is it likely that extra costs may be incurred for special task instruction?
- Are personnel changes called for? Their costs must be considered also.
- Can accident compensation rates be expected to increase?
2. Safety
- Will the job being considered for the disabled worker involve safety regulations?
- Will special safety regulations be involved?
- Is the work characterized by a considerable frequency of accidents or near accidents?
3. Medical
- As regards the worker whose disability is being examined with a view to his or her re-entry into the workplace, the nature and seriousness of the incapacity must be assessed.
- The extent of the disabled worker’s absence must also be taken into account.
- What is the character and frequency of the worker’s “minor” symptoms, and how are they to be dealt with? Can the future development of related “minor” illnesses capable of hampering the worker’s efficiency be foreseen?
As concerns time lost from work, these calculations can be made in terms of wages, overhead, compensation and lost production. The sort of analyses just described represents a rational approach by which an organization can arrive at an informed decision as to whether a disabled worker is better off back on the job and whether the organization itself will gain by his or her return to work.
In the preceding discussion, designing for the broader population has received a focus of attention heightened by emphasis on specific design in relation to usability and the costs and benefits of such design. It is still a difficult task to make the needed calculations, including all relevant factors, but at present, research efforts are continuing that incorporate modelling methods in their techniques. In some countries, for example the Netherlands and Germany, government policy is making companies more responsible for job-related personal harm; fundamental changes in regulatory policies and insurance structures are, clearly, to be expected to result from trends of this sort. It has already become a more or less settled policy in these countries that a worker who suffers a disabling accident at work should be provided with an adapted work station or be able to perform other work within the company, a policy that has made the treatment of the disabled a genuine achievement in the humane treatment of the worker.
Workers with Limited Functional Capacity
Whether design is aimed at the disabled or at the broader average, it is hindered by a scarcity of research data. Handicapped people have been the subjects of virtually no research efforts. Therefore, in order to set up a product requirements document, or PRD, a specific empirical research study will have to be undertaken in order to gather that data by observation and measurement.
In gathering the information needed about the disabled worker or user it is necessary to consider not only the current functional status of the disabled person, but to make the attempt to foresee whatever changes might be the result of the progression of a chronic condition. This kind of information can, in fact, be elicited from the worker directly, or a medical specialist can supply it.
In designing, for instance, a work action to which data about the worker’s physical strength is relevant, the designer will not choose as a specification the maximum strength which the disabled person can exert, but will take into account any possible diminution in strength that a progression in the worker’s condition might bring about. Thus the worker will be enabled to continue to use the machines and tools adapted or designed for him or at the work station.
Furthermore, designers should avoid designs that involve manipulations of the human body at the far extremes of, say, the range of motion of a body part, but should accommodate their designs to the middle ranges. A simple but very common illustration of this principle follows. A very common part of the drawers of kitchen and office cabinets and desks is a handle that has the form of a little shelf under which one places the fingers, exerting upward and forward force to open the drawer. This manoeuvre requires 180 degrees of supination (with the palm of the hand up) in the wrist—the maximum point for the range of this sort of motion of the wrist. This state of affairs may present no difficulty for a healthy person, provided that the drawer can be opened with a light force and is not awkwardly situated, but makes for strain when the action of the drawer is tight or when the full 180-degree supination is not possible, and is a needless burden on a disabled person. A simple solution—a vertically placed handle—would be mechanically far more efficient and more easily manipulated by a larger portion of the population.
Physical Functioning Ability
In what follows, the three chief areas of limitation in physical functional ability, as defined by the locomotion system, the neurological system and the energy system, will be discussed. Designers will gain some insight into the nature of user/worker constraints in considering the following basic principles of bodily functions.
The locomotion system. This consists of the bones, joints, connective tissues and muscles. The nature of the joint structure determines the range of motion possible. A knee joint, for example, shows a different degree of movement and stability than the joint of the hip or the shoulder. These varying joint characteristics determine the actions possible to the arms, hands, feet, and so on. There are also different types of muscle; it is the type of muscle, whether the muscle passes over one or two joints, and the location of the muscle that determines, for a given body part, the direction of its movement, its speed, and the strength which it is capable of exerting.
The fact that this direction, speed and strength can be characterized and calculated is of great importance in design. For disabled people, one has to take it into account that the “normal” locations of muscles have been disturbed and that the range of motion in joints has been changed. In an amputation, for instance, a muscle may function only partly, or its location may have changed, so that one has to examine the physical ability of the patient carefully to establish what functions remain and how reliable they may be. A case history follows.
A 40-year-old carpenter lost his thumb and the third finger of his right hand in an accident. In an effort to restore the carpenter’s capacity for work, a surgeon removed one of the patient’s great toes and he replaced the missing thumb with it. After a period of rehabilitation, the carpenter returned to work but found it impossible to do sustained work for more than three to four hours. His tools were studied and found to be unfitted to the “abnormal” structure of his hand. The rehabilitation specialist, examining the “redesigned” hand from the point of view of its new functional ability and form was able to have new tools designed that were more appropriate and usable with respect to the altered hand. The load on the worker’s hand, previously too heavy, was now within a usable range, and he regained his ability to continue work for a longer time.
The neurological system. The neurological system can be compared to a very sophisticated control room, complete with data collectors, whose purpose it is to initiate and govern one’s movements and actions by interpreting information relating to those aspects of the body’s components relating to position and mechanical, chemical and other states. This system incorporates not only a feedback system (e.g., pain) that provides for corrective measures, but a “feed-forward” capability which expresses itself anticipatorily so as to maintain a state of equilibrium. Consider the case of a worker who reflexively acts so as to restore a posture in order to protect himself from a fall or from contact with dangerous machine parts.
In disabled persons, the physiological processing of information can be impaired. Both the feedback and the feed-forward mechanisms of visually impaired people are weakened or absent, and the same is true, on an acoustic level, among the hearing-impaired. Furthermore the important governing circuits are interactive. Sound signals have an effect on the equilibrium of a person in conjunction with proprioceptive circuits that situate our bodies in space, so to speak, via data gathered from muscles and joints, with the further help of visual signals. The brain can function to overcome quite drastic deficiencies in these systems, correcting for errors in the coding of information and “filling in” missing information. Beyond certain limits, to be sure, incapacity supervenes. Two case histories follow.
Case 1. A 36-year-old woman suffered a lesion of the spinal cord due to an automobile accident. She is able to sit up without assistance and can move a wheelchair manually. Her trunk is stable. The feeling in her legs is gone, however; this defect includes an inability to sense temperature changes.
She has a sitting workplace at home (the kitchen is designed to allow her to work in a seated position). The safety measure has been taken of installing a sink in a position sufficiently isolated that the risk of burning her legs with hot water is minimized, since her inability to process temperature information in the legs leaves her vulnerable to being unaware of being burned.
Case 2. A five-year-old boy whose left side was paralysed was being bathed by his mother. The doorbell rang, the mother left the boy alone to go to the front door, and the boy, turning on the hot-water tap, suffered burns. For safety reasons, the bath should have been equipped with a thermostat (preferably one that the boy could not have overridden).
The energy system. When the human body has to perform physical labour, physiological changes, notably in the form of interactions in the muscle cells, take place, albeit relatively inefficiently. The human “motor” converts only about 25% of its energy supply to mechanical activity, the remainder of the energy representing thermal losses. The human body is therefore not especially suited to heavy physical labour. Exhaustion sets in after a certain time, and if heavy labour has to be performed, reserve energy sources are drawn upon. These sources of reserve energy are always used whenever work is carried out very rapidly, is started suddenly (without a warm-up period) or involves heavy exertion.
The human organism obtains energy aerobically (via oxygen in the bloodstream) and anaerobically (after depleting aerobic oxygen, it calls upon small, but important reserve units of energy stored in muscle tissue). The need for fresh air supplies in the workplace naturally draws the focus of discussion of oxygen usage toward the aerobic side, working conditions that are strenuous enough to call forth anaerobic processes on a regular basis being extraordinarily uncommon in most workplaces, at least in the developed countries. The availability of atmospheric oxygen, which relates so directly to human aerobic functioning, is a function of several conditions:
- Ambient air pressure (approximately 760 torr, or 21.33 kPa at sea level). High-altitude task performance can be profoundly affected by oxygen deficiency and is a prime consideration for workers in such conditions.
- For workers doing heavy labour, ventilation is necessary to ensure refreshment of the air supply, allowing the volume of air respired per minute to be increased.
- Ambient oxygen makes its way into the bloodstream via the alveoli by diffusion. At higher blood pressures, the diffusion surface is enlarged and thereby the oxygen capacity of the blood.
- An increase in oxygen diffusion to the tissues causes an increase of the diffusion surface and consequently of the oxygen level.
- People with certain heart problems suffer when, with increased cardiac output (together with the oxygen level), the blood circulation changes in favour of the muscles.
- By contrast with oxygen, because of the large reserves of glucose, and especially fat, the energy source (“fuel”) need not be continuously delivered from the outside. In heavy labour, it is merely glucose, with its high energy value, that is used. With lighter work, fat is called upon, at a rate varying with the individual. A brief, general case history follows.
A person suffering from asthma or bronchitis, both of which are diseases affecting the lungs, causes the worker severe limitation in his or her work. The work assignment of this worker should be analysed with respect to factors such as physical load. The environment should be analysed as well: clean ambient air will contribute substantially to workers’ well-being. Furthermore, the workload should be balanced through the day, avoiding peak loads.
Specific Design
In some cases, however, there is still a need for specific design, or design for very small groups. Such a need arises when the tasks to be performed and the difficulties a disabled person is experiencing are excessively large. If the needed specific requirements cannot be made with the available products on the market (even with adaptations), specific design is the answer. Whether this sort of solution may be costly or cheap (and aside from humanitarian issues) it must be nonetheless regarded in the light of workability and support to the firm’s viability. A specially designed worksite is worthwhile economically only when the disabled worker can look forward to working there for years and when the work he or she does is, in production terms, an asset to the company. When this is not the case, although the worker may indeed insist upon his or her right to the job, a sense of realism should prevail. Such touchy problems should be approached in a spirit of seeking a solution by cooperative endeavours at communication.
The advantages of specific design are as follows:
- The design is custom made: it fits the problems to be solved to perfection.
- The worker so served can return to work and a life of social participation.
- The worker can be self-sufficient, independent of welfare.
- The costs of any personnel changes that the alternative might involve are avoided.
The disadvantages of specific design are:
- The design is unlikely to be used for even one other person, let alone a larger group.
- Specific design is often costly.
- Specifically designed products must often be handmade; savings owing to mass methods are most often not realizable.
Case 1. For example, there is the case of a receptionist in a wheelchair who had a speech problem. Her speech difficulty made for rather slow conversations. While the firm remained small, no problems arose and she continued to work there for years. But when the firm enlarged, her disabilities began to make themselves problematic. She had to speak more rapidly and to move about considerably faster; she could not cope with the new demands. However, solutions to her troubles were sought and reduced themselves to two alternatives: special technical equipment might be installed so that the deficiencies that degraded the quality of some of her tasks could be compensated for, or she could simply choose a set of tasks involving a more desk-bound workload. She chose the latter course and still works for the same company.
Case 2. A young man, whose profession was the production of technical drawings, suffered a high level spinal cord lesion due to diving in shallow waters. His injury is severe enough for him to require help with all his daily activities. Nevertheless, with the help of a computer-aided design (CAD) software, he continues to be able make his living at technical drawing and lives, financially independent, with his partner. His work space is a study adapted for his needs and he works for a firm with which he communicates by computer, phone and fax. To operate his personal computer, he had to have certain adaptations made to the keyboard. But with these technical assets he can earn a living and provide for himself.
The approach for specific design is not different from other design as described above. The only insurmountable problem that may arise during a design project is that the design objective cannot be achieved on purely technical grounds—in other words, it can’t be done. For example, a person suffering from Parkinson’s disease is prone, at a certain stage in the progression of his or her condition, to fall over backwards. An aid which would prevent such an eventuality would of course represent the desired solution, but the state of the art is not such that such a device can yet be built.
System Ergonomic Design and Workers with Special Physical Needs
One can treat bodily impairment by medically intervening to restore the damaged function, but the treatment of a disability, or deficiency in the ability to perform tasks, can involve measures far less developed in comparison with medical expertise. As far as the necessity of treating a disability is concerned, the severity of the handicap strongly influences such a decision. But given that treatment is called for, however, the following means, taken singly or in combination, form the choices available to the designer or manager:
- leaving out a task
- compensating for a worker’s deficiency in performing a task element by using a machine or another person’s help
- differentiation of the task order, that is, dividing the task into more manageable subtasks
- modification of the tools used in the task
- special design of tools and machines.
From the specific ergonomic point of view, treatment of a disability includes the following:
- modification of the task
- modification of a tool
- design of new tools or new machines.
The issue of efficacy is always the point of departure in the modification of tools or machines, and is often related to the costs devoted to the modification in question, the technical features to be addressed, and the functional changes to be embodied in the new design. Comfort and attractiveness are qualities that by no means deserve to be neglected among these other characteristics.
The next consideration relating to design changes to be made to a tool or machine is whether the device is one already designed for general use (in which case, modifications will be made to a pre-existing product) or is to be designed with an individual type of disability in mind. In the latter case, specific ergonomic considerations must be devoted to each aspect of the worker’s disability. For example, given a worker suffering from limitations in brain function after a stroke, impairments such as aphasia (difficulty in communication), a paralysed right arm, and a spastic paresis of the leg preventing its being moved upwards might require the following adjustments:
- a personal computer or other device enabling the worker to communicate
- tools that can be operated with the remaining useful arm
- a prosthetic system that would serve to restore the function of the impaired foot as well as to compensate for the patient’s loss of ability to walk.
Is there any general answer to the question of how to design for the disabled worker? The system ergonomic design (SED) approach is an eminently suitable one for this task. Research related to the work situation or to the kind of product at issue requires a design team for the purpose of gathering special information relating either to a special group of disabled workers or to the unique case of an individual user disabled in a particular way. The design team will, by virtue of including a diversity of qualified people, be in possession of expertise beyond the technical sort expected of a designer alone; the medical and ergonomic knowledge shared among them will be as fully applicable as the strictly technical.
Design constraints determined by assembling data related to disabled users are treated with the same objectivity and in the same analytical spirit as are counterpart data relating to healthy users. Just as for the latter, one has to determine for disabled persons their personal patterns of behavioural response, their anthropometrical profiles, biomechanical data (as to reach, strength, range of motion, handling space used, physical load and so forth), ergonomic standards and safety regulations. But one is most regretfully obliged to concede that very little research indeed is done on behalf of disabled workers. There exist a few studies on anthropometry, somewhat more on biomechanics in the field of prostheses and orthoses, but hardly any studies have been carried on physical load capabilities. (The reader will find references to such material in the “Other relevant reading” list at the end of this chapter.) And while it is sometimes easy to gather and apply such data, frequently enough the task is difficult, and in fact, impossible. To be sure, one must obtain objective data, however strenuous the effort and unlikely the chances of doing so, given that the numbers of disabled persons available for research is small. But they are quite often more than willing to participate in whatever research they are offered the opportunity of sharing in, since there is great consciousness of the importance of such a contribution towards design and research in this field. It thus represents an investment not only for themselves but for the larger community of disabled people.
Designing for Specific Groups
In designing a product or an industrial process, one focuses on the “average” and “healthy” worker. Information regarding human abilities in terms of muscular strength, bodily flexibility, length of reach, and many other characteristics is for the most part derived from empirical studies carried out by military recruitment agencies, and reflects measured values valid for the typical young male in his twenties. But working populations, to be sure, consist of people of both sexes and a broad range of ages, to say nothing of a variety of physical types and abilities, levels of fitness and health, and functional capacities. A classification of the varieties of functional limitation among people as outlined by the World Health Organization is given in the accompanying article "Case Study: The International Classifcation of Functional Limitation in People." At present, industrial design for the most part takes insufficient account of the general abilities (or inabilities, for that matter) of workers at large, and should take as its point of departure a broader human average as a basis for design. Clearly, a suitable physical load for a 20-year-old may exceed the capacity to manage of a 15-year-old or a 60-year-old. It is the business of the designer to consider such differences not only from the point of view of efficiency, but with a eye to the prevention of job-related injury and illness.
The progress of technology has brought about the state of affairs that, of all the workplaces in Europe and North America, 60% involve the seated position. The physical load in work situations is now on average far less than before, but many worksites, nonetheless, call for physical loads that cannot be sufficiently reduced to fit human physical capabilities; in some developing countries, the resources of current technology are simply not available to relieve the human physical burden to any appreciable extent. And in technologically advanced countries, it is still a common problem that a designer will adapt his or her approach to constraints imposed by product specifications or production processes, either slighting or leaving out human factors related to disability and the prevention of harm due to the workload. With respect to these aims, designers have to be educated to devote attention to all such human factors, expressing the results of their study in a product requirements document (PRD). The PRD contains the system of demands which the designer has to meet in order to achieve both the expected product quality level and the satisfaction of human capability needs in the production process. While it is unrealistic to demand a product that matches a PRD in every respect, given the need of unavoidable compromises, the design method suited to the closest approach to this goal is the system ergonomic design (SED) method, to be discussed following a consideration of two alternative design approaches.
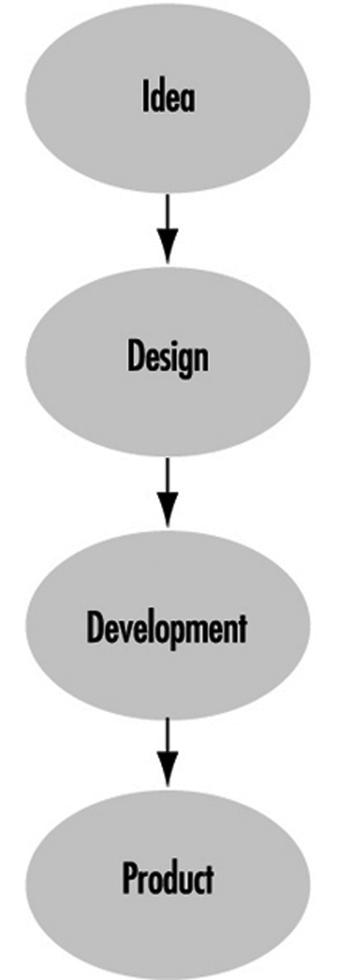
Creative Design
This design approach is characteristic of artists and others involved in the production of work of a high order of originality. The essence of this design process is that a concept is worked out intuitively and through “inspiration”, allowing problems to be dealt with as they arise, without conscious deliberation beforehand. Sometimes, the outcome will not resemble the initial concept, but nonetheless represents what the creator regards as his or her authentic product. Not seldom, too, the design is a failure. Figure 1 illustrates the route of creative design.
System design arose from the need to predetermine the steps in design in a logical order. As design becomes complex, it has to be subdivided into subtasks. Designers or subtask teams thus become interdependent, and design becomes the job of a design team rather than an individual designer. Complementary expertise is distributed through the team, and design assumes an interdisciplinary character.
System design is oriented to the optimal realization of complex and well-defined product functions through the selection of the most appropriate technology; it is costly, but the risks of failure are considerably reduced as compared with less organized approaches. The efficacy of the design is measured against the goals formulated in the PRD.
The way in which the specifications formulated in the PRD are of the first importance. Figure 2 illustrates the relationship between the PRD and other parts of the system design process.
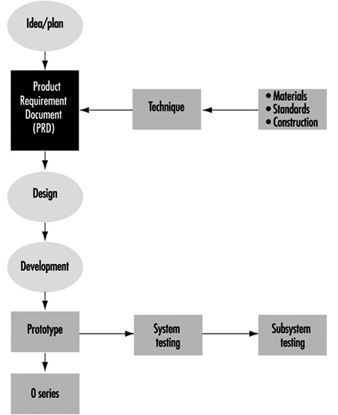
As this scheme shows, the input of the user is neglected. Only at the end of the design process can the user criticize the design. This is unhelpful to both producer and user, since one has to wait for the next design cycle (if there is one) before errors can be corrected and modifications made. Furthermore, user feedback is seldom systematized and imported into a new PRD as a design influence.
System ergonomic design (SED)
SED is a version of system design adapted to ensure that the human factor is accounted for in the design process. Figure 3 illustrates the flow of user input into the PRD.
Figure 3. System ergonomic design
 In system ergonomic design, the human being is considered part of the system: design specification changes are, in fact, made in consideration of the worker’s abilities with respect to cognitive, physical and mental aspects, and the method lends itself as an efficient design approach for any technical system where human operators are employed.
In system ergonomic design, the human being is considered part of the system: design specification changes are, in fact, made in consideration of the worker’s abilities with respect to cognitive, physical and mental aspects, and the method lends itself as an efficient design approach for any technical system where human operators are employed.
For example, to examine the implications of the worker’s physical abilities, task-allocation in the design of the process will call for a careful selection of tasks to be performed by the human operator or by the machine, each task being studied for its aptness to machine or human treatment. Clearly, the human worker will be more effective at interpreting incomplete information; machines however calculate much more rapidly with prepared data; a machine is the choice for lifting heavy loads; and so forth. Furthermore, since the user-machine interface can be tested at the prototype phase, one can eliminate design errors that would otherwise untimely manifest themselves at the phase of technical functioning.
Methods in User Research
No “best” method exists, nor any source of formulae and sure and certain guidelines, according to which design for disabled workers ought to be undertaken. It is a rather a common-sense business of making as exhaustive search of all obtainable knowledge relevant to the problem and of implementing it to its most evident best effect.
Information can be assembled from sources such as the following:
- The literature of research results.
- Direct observation of the disabled person at work and description of his or her particular work difficulties. Such observation should be made at a point in the worker’s schedule when he or she can be expected to be subject to fatigue—the end of a work shift, perhaps. The point is that any design solutions should be adapted to the most arduous phase of the work process, or else such phases may fail to be performed adequately (or at all) owing to the worker’s capacity having been physically exceeded.
- The interview. One has to be aware of the possibly subjective responses which the interview per se may have the effect of eliciting. It is a far better approach that the interview technique be combined with observation. Disabled persons sometimes hesitate to discuss their difficulties, but when workers are aware that the investigator is willing to exert special thoroughness on their behalf, their reticence will diminish. This technique is time-consuming, but quite worthwhile.
- Questionnaires. An advantage of the questionnaire is that it can be distributed to large groups of respondents and at the same time gather data of as specific a sort as one wishes to provide for. The questionnaire must, however, be constructed upon the basis of representative information pertaining to the group to which it will be administered. This means that the type of information to be sought must be obtained on the basis of interviews and observations carried out among a sample of workers and specialists that ought to be reasonably restricted as to size. In the case of disabled persons, it is sensible to include among such a sample the physicians and therapists who are involved with prescribing special aids for disabled persons and have examined them regarding their physical capabilities.
- Physical measurements. Measurements obtained from instruments in the field of bio-instrumentation (e.g., the activity level of muscles, or the amount of oxygen consumed in a given task) and by anthropometrical methods (e.g., the linear dimensions of body elements, the range of motion of limbs, muscular strength) are of indispensable value in human-oriented work designs.
The methods described above are some of the various ways of gathering data about people. Methods exist, too, to evaluate user-machine systems. One of these—simulation—is to construct a realistic physical copy. The development of a more or less abstract symbolic representation of a system is an example of modelling. Such expedients, of course, are both useful and necessary when the actual system or product is not in existence or not accessible to experimental manipulation. Simulation is more often used for training purposes and modelling for research. A mock-up is a full-size, three-dimensional copy of the designed workplace composed, where necessary, of improvised materials, and is of great use in testing design possibilities with the proposed disabled worker: in fact, the majority of design problems can be identified with the aid of such a device. Another advantage to this approach is that the motivation of the worker grows as he or she participates in the design of his or her own future workstation.
Analysis of Tasks
In the analysis of tasks, different aspects of a defined job are subject to analytical observation. These manifold aspects include posture, routing of work manipulations, interactions with other workers, handling tools and operating machines, the logical order of subtasks, the efficiency of operations, static conditions (a worker may have to perform tasks in the same posture over a long time or with high frequency), dynamic conditions (calling for numerous varying physical conditions), material environmental conditions (as in a cold slaughterhouse) or non-material conditions (as with stressful work surroundings or the organization of the work itself).
Work design for the disabled person has, then, to be founded on a thorough task analysis as well as a full examination of the functional abilities of the disabled person. The basic design approach is a crucial issue: it is more efficient to elaborate all possible solutions for the problem in hand without prejudice than to produce a single design concept or a limited number of concepts. In design terminology, this approach is called making a morphological overview. Given the multiplicity of original design concepts, one can proceed to an analysis of the pro and con features of each possibility with respect to material use, construction method, technical production features, ease of manipulation, and so on. It is not unprecedented that more than one solution reaches the prototype stage and that a final decision is made at a relatively late phase in the design process.
Although this may seem a time-consuming way to realize design projects, in fact the extra work it entails is compensated for in terms of fewer problems encountered in the developmental stage, to say nothing that the result—a new workstation or product—will have embodied a better balance between the needs of the disabled worker and the exigencies of the working environment. Unfortunately, the latter benefit rarely if ever reaches the designer in terms of feedback.
Product Requirements Document (PRD) and Disability
After all information relating to a product has been assembled, it should be transformed into a description not only of the product but of all those demands which may be made of it, regardless of source or nature. These demands may of course be divided along various lines. The PRD should include demands relating to user-operator data (physical measurements, range of motion, range of muscular strength, etc.), technical data (materials, construction, production technique, safety standards, etc.), and even conclusions arising out of market feasibility studies.
The PRD forms the designer’s framework, and some designers regard it as an unwelcome restriction of their creativity rather than as a salutary challenge. In view of the difficulties at times accompanying the execution of a PRD, it should always be borne steadily in mind that a design failure causes distress for the disabled person, who may relinquish his or her efforts to succeed in the employment arena (or else fall helpless victim to the progress of the disabling condition), and additional costs for redesign as well. To this end, technical designers should not operate alone in their design work for the disabled, but should cooperate with whatever disciplines are needed for securing the medical and functional information to set up an integrated PRD as a framework for the design.
Prototype Testing
When a prototype is built, it should be tested for errors. Error testing should be carried out not only from the point of view of the technical system and subsystems, but also with a view to its usability in combination with the user. When the user is a disabled person, extra precautions have to be taken. An error to which an unimpaired worker may successfully respond in safety may not afford the disabled worker the opportunity of avoiding harm.
Prototype testing should be carried out on a small number of disabled workers (except in the case of a unique design) according to a protocol matched to the PRD. Only by such empirical testing can the degree to which the design meets the demands of the PRD be adequately judged. Although results on small numbers of subjects may not be generalizable to all cases, they do supply valuable information for the designer’s use in either the final design or in future designs.
Evaluation
The evaluation of a technical system (a work situation, machine or tool) should be judged on its PRD, not by questioning the user or even by attempting comparisons of alternative designs with respect to physical performance. For instance, the designer of a specific knee brace, basing his or her design on research results that show unstable knee joints to exhibit a delayed hamstring reaction, will create a product that compensates for this delay. But another brace may have different design aims. Yet present evaluation methods show no insight as to when to prescribe what kind of knee brace to which patients under what conditions—precisely the sort of insight a health professional needs when prescribing technical aids in the treatment of disabilities.
Current research aims at making this sort of insight possible. A model used to obtain insight into those factors which actually determine whether or not a technical aid ought to be used, or whether or not a worksite is well designed and equipped for the disabled worker is the Rehabilitation Technology Useability Model (RTUM). The RTUM model offers a framework to use in evaluations of existing products, tools or machines, but can also be used in combination with the design process as shown in figure 4.
Figure 4. Rehabilitation Technology Useability Model (RTUM) in combination with the system ergonomic design approach

Evaluations of existing products reveal that as regards technical aids and worksites, the quality of PRDs is very poor. At some times, the product requirements are not recorded properly; at others they are not developed to a useful extent. Designers simply must learn to start documenting their product requirements, including those relevant to disabled users. Note that, as figure 4 shows, RTUM, in conjunction with SED, offers a framework that includes the requirements of disabled users. Agencies responsible for prescribing products for their users must request industry to evaluate those products before marketing them, a task in essence impossible in the absence of product requirement specifications; figure 4 also shows how provision can be made to ensure that the end result can be evaluated as it should (on a PRD) with the help of the disabled person or group for whom the product is intended. It is up to national health organizations to stimulate designers to abide by such design standards and to formulate appropriate regulations.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."