- You are here:
-
Home

-
Contents
-
Part I. The Body
- Cardiovascular System

3. Cardiovascular System
Chapter Editors: Lothar Heinemann and Gerd Heuchert
Table of Contents
Tables and Figures
Introduction
Lothar Heinemann and Gerd Heuchert
Cardiovascular Morbidity and Mortality in the Workforce
Gottfried Enderlein and Lothar Heinemann
The Risk Factor Concept in Cardiovascular Disease
Lothar Heinemann, Gottfried Enderlein and Heide Stark
Rehabilitation and Prevention Programmes
Lothar Heinemann and Gottfried Enderlein
Physical, Chemical and Biological Hazards
Physical Factors
Heide Stark and Gerd Heuchert
Chemical Hazardous Materials
Ulrike Tittelbach and Wolfram Dietmar Schneider
Biological Hazards
Regina Jäckel, Ulrike Tittelbach and Wolfram Dietmar Schneider
Tables
Click a link below to view table in article context
- Mortality from cardiovascular diseases
- Mortality rates, special cardiovascular diagnosis groups
- Rate of disease and reduced work ability
- Work associated with cardiovascular hazards
- Occupation-related infection and disease
Figures
Point to a thumbnail to see figure caption, click to see the figure in the article context.



Children categories

Physical, Chemical and Biological Hazards (3)
Physical, Chemical and Biological Hazards
Physical Factors
Noise
Hearing loss due to workplace noise has been recognized as an occupational disease for many years. Cardiovascular diseases are at the centre of the discussion on possible chronic extra-aural effects of noise. Epidemiological studies have been done within the workplace noise field (with high-level noise indicators) as well as in the surrounding noise field (with low-level noise indicators). The best studies to date were done on the relationship between exposure to noise and high blood pressure. In numerous new survey studies, noise researchers have assessed the available research results and summarized the current state of knowledge (Kristensen 1994; Schwarze and Thompson 1993; van Dijk 1990).
Studies show that the noise risk factor for diseases of the cardiovascular system is less significant than behavioural risk factors like smoking, poor nutrition or physical inactivity (Aro and Hasan 1987; Jegaden et al. 1986; Kornhuber and Lisson 1981).
The results of epidemiological studies do not permit any final answer on the adverse cardiovascular health effects of chronic workplace or environmental noise exposure. The experimental knowledge on hormonal stress effects and changes in peripheral vasoconstriction, on the one hand, and the observation, on the other, that a high workplace noise level >85 dBA) promotes the development of hypertension, allow us to include noise as an non-specific stress stimulus in a multi-factored risk model for cardiovascular diseases, warranting high biological plausibility.
The opinion is advanced in modern stress research that although increases in blood pressure during work are connected to noise exposure, the blood pressure level per se depends on a complex set of personality and environmental factors (Theorell et al. 1987). Personality and environmental factors play an intimate role in determining the total stress load at the workplace.
For this reason it appears all the more urgent to study the effect of multiple burdens at the workplace and to clarify the cross effects, mostly unknown up to now, between combined influencing exogenous factors and diverse endogenous risk characteristics.
Experimental studies
It is today generally accepted that noise exposure is a psychophysical stressor. Numerous experimental studies on animals and human subjects permit extending the hypothesis on the pathomechanism of noise to the development of cardiovascular diseases. There is a relatively uniform picture with respect to acute peripheral reactions to noise stimuli. Noise stimuli clearly cause peripheral vasoconstriction, measurable as a decrease in finger pulse amplitude and skin temperature and an increase in systolic and diastolic blood pressure. Almost all studies confirm an increase in heart rate (Carter 1988; Fisher and Tucker 1991; Michalak, Ising and Rebentisch 1990; Millar and Steels 1990; Schwarze and Thompson 1993; Thompson 1993). The degree of these reactions is modified by such factors as the type of noise occurrence, age, sex, state of health, nervous state and personal characteristics (Harrison and Kelly 1989; Parrot et al. 1992; Petiot et al. 1988).
A wealth of research deals with the effects of noise on metabolism and hormone levels. Exposure to loud noise almost always results fairly quickly in changes such as in blood cortisone, cyclical adenosinmonophosphate (CAMP), cholesterol and certain lipoprotein fractions, glucose, protein fractions, hormones (e.g., ACTH, prolactin), adrenalin and noradrenalin. Increased catecholamine levels can be found in the urine. All of this clearly shows that noise stimuli below the noise-deafness level can lead to hyperactivity of the hypophyseal adrenal cortex system (Ising and Kruppa 1993; Rebentisch, Lange-Asschenfeld and Ising 1994).
Chronic exposure to loud noise has been shown to result in a reduction of magnesium content in serum, erythrocytes and in other tissues, such as the myocardium (Altura et al. 1992), but study results are contradictory (Altura 1993; Schwarze and Thompson 1993).
The effect of workplace noise on blood pressure is equivocal. A series of epidemiological studies, which were mostly designed as cross-sectional studies, indicate that employees with long-term exposure to loud noise show higher systolic and/or diastolic blood pressure values than those who work under less noisy conditions. Counterpoised, however, are studies that found very little or no statistical association between long-term noise exposure and in- creased blood pressure or hypertension (Schwarze and Thompson 1993; Thompson 1993; van Dijk 1990). Studies that enlist hearing loss as a surrogate for noise show varied results. In any case, hearing loss is not a suitable biological indicator for noise ex- posure (Kristensen 1989; van Dijk 1990). The indications are mounting that noise and the risk factors—increased blood pres- sure, increased serum cholesterol level (Pillsburg 1986), and smoking (Baron et al. 1987)—have a synergistic effect on the de- velopment of noise-induced hearing loss. Differentiating between hearing loss from noise and hearing loss from other factors is difficult. In the studies (Talbott et al. 1990; van Dijk, Veerbeck and de Vries 1987), no connection was found between noise exposure and high blood pressure, whereas hearing loss and high blood pressure have a positive correlation after correction for the usual risk factors, especially age and body weight. The relative risks for high blood pressure range between 1 and 3.1 in com- parisons of exposure to loud and less loud noise. Studies with qualitatively superior methodology report a lower relationship. Differences among the blood pressure group means are relatively narrow, with values between 0 and 10 mm Hg.
A large epidemiological study of women textile workers in China (Zhao, Liu and Zhang 1991) plays a key role in noise effect research. Zhao ascertained a dose-effect relationship between noise levels and blood pressure among women industrial workers who were subject to various noise exposures over many years. Using an additive logistical model the factors “indicated cooking salt use”, “family history of high blood pressure” and “noise level” (0.05) significantly correlated with the probability of high blood pressure. The authors judged that no confounding was present due to overweight. The noise level factor nevertheless constituted half the risk of hypertension of the first two named factors. An increase in the noise level from 70 to 100 dBA raised the risk for high blood pressure by a factor of 2.5. The quantification of the risk of hypertension by using higher noise exposure levels was possible in this study only because the offered hearing protection was not worn. This study looked at non-smoking women aged 35 ±8 years, so according to v. Eiff’s results (1993), the noise-related risk of hypertension among men could be significantly higher.
Hearing protection is prescribed in western industrialized countries for noise levels over 85-90 dBA. Many studies carried out in these countries demonstrated no clear risk at such noise levels, so it can be concluded from Gierke and Harris (1990) that limiting the noise level to the set limits prevents most extra-aural effects.
Heavy Physical Work
The effects of “lack of movement” as a risk factor for cardiovascular disease and of physical activity as promoting health were elucidated in such classic publications as those by Morris, Paffenbarger and their co-workers in the 1950s and 1960s, and in numerous epidemiological studies (Berlin and Colditz 1990; Powell et al. 1987). In previous studies, no direct cause-and-effect relationship could be shown between lack of movement and the rate of cardiovascular disease or mortality. Epidemiological studies, however, point to the positive, protective effects of physical activity on reducing various chronic diseases, including coronary heart disease, high blood pressure, non insulin dependent diabetes mellitus, osteoporosis and colon cancer, as well as anxiety and depression. The connection between physical inactivity and the risk of coronary heart disease has been observed in numerous countries and population groups. The relative risk for coronary heart disease among inactive people compared to active people varies between 1.5 and 3.0; with the studies using qualitatively higher methodology showing higher relationship. This increased risk is comparable to that found for hypercholesterolemia, hypertension and smoking (Berlin and Colditz 1990; Centers for Disease Control and Prevention 1993; Kristensen 1994; Powell et al. 1987).
Regular, leisure-time physical activity appears to reduce the risk of coronary heart disease through various physiological and metabolic mechanisms. Experimental studies have shown that with regular motion training, the known risk factors and other health-related factors are positively influenced. It results, for example, in an increase in the HDL-cholesterol level, and a decrease in the serum-triglyceride level and blood pressure (Bouchard, Shepard and Stephens 1994; Pate et al. 1995).
A series of epidemiological studies, spurred on by the studies of Morris et al. on coronary risk among London bus drivers and conductors (Morris, Heady and Raffle 1956; Morris et al. 1966), and the study of Paffenbarger et al. (1970) among American harbour workers, looked at the relationship between the difficulty level of physical work and the incidence of cardiovascular diseases. Based on earlier studies from the 1950s and 1960s the prevailing idea was that physical activity at work could have a certain protective effect on the heart. The highest relative risk for cardiovascular diseases was found in people with physically inactive jobs (e.g., sitting jobs) as compared to people who do heavy physical work. But newer studies have found no difference in the frequency of coronary disease between active and inactive occupational groups or have even found a higher prevalence and incidence of cardiovascular risk factors and cardiovascular diseases among heavy labourers (Ilmarinen 1989; Kannel et al. 1986; Kristensen 1994; Suurnäkki et al. 1987). Several reasons can be given for the contradiction between the health-promoting effect of free-time physical activities on cardiovascular morbidity and the lack of this effect with heavy physical labour:
- Primary and secondary selection processes (healthy worker effect) can lead to serious distortions in occupational medical epidemiological studies.
- The relationship found between physical work and the onset of cardiovascular diseases can be influenced by a number of confounding variables (like social status, education, behavioural risk factors).
- Assessing the physical load, often solely on the basis of job descriptions, must be seen as an inadequate method.
Social and technological development since the 1970s has meant that only a few jobs with “dynamic physical activity” remain. Physical activity in the modern workplace often means heavy lifting or carrying and a high proportion of static muscle work. So it is not surprising that physical activity in occupations of this type lacks an essential criterion for coronary-protective effect: a sufficient intensity, duration and frequency to optimize the physical load on big muscle groups. The physical work is, in general, intensive, but has less of a workout effect on the cardiovascular system. The combination of heavy, physically demanding work and high free-time physical activity could establish the most favourable situation with respect to the cardiovascular risk-factor profile and the onset of CHD (Saltin 1992).
The results of studies to date are also not consistent on the question of whether heavy physical work is related to the onset of arterial hypertension.
Physically demanding work is related to changes in blood pressure. In dynamic work that utilizes big muscle masses, blood supply and demand are in balance. In dynamic work that requires the smaller and middle muscle masses, the heart may put out more blood than is needed for the total physical work and the result can be considerably increased systolic and diastolic blood pressure (Frauendorf et al. 1986).
Even with combined physical-mental strain or physical strain under the effects of noise, a substantial increase in blood pressure and heart rate are seen in a certain percentage (approximately 30%) of people (Frauendorf, Kobryn and Gelbrich 1992; Frauendorf et al. 1995).
No studies are presently available on the chronic effects of this increased circulatory activity in local muscle work, with or without noise or mental strain.
In two recently published independent studies, by American and German researchers (Mittleman et al. 1993; Willich et al. 1993), the question was pursued as to whether heavy physical work can be a trigger for an acute myocardial infarction. In the studies, of 1,228 and 1,194 people with acute myocardial infarction respectively, the physical strain one hour before the infarction was compared with the situation 25 hours before. The following relative risks were calculated for the onset of a myocardial infarction within one hour of heavy physical strain in comparison with light activity or rest: 5.9 (CI 95%: 4.6-7.7) in the American and 2.1 (CI 95%: 1.6-3.1) in the German study. The risk was highest for people not in shape. An important limiting observation is, however, that the heavy physical strain occurred one hour before the infarction in only 4.4 and 7.1% of the infarction patients respectively.
These studies involve questions of the significance of physical strain or a stress-induced increased output of catecholamines on the coronary blood supply, on triggering coronary spasms, or an immediately harmful effect of catecholamines on the beta adrenergic receptors of the heart muscle membrane as a cause of the infarction manifestation or acute cardiac death. It can be assumed that such results will not ensue with a healthy coronary vessel system and intact myocardium (Fritze and Müller 1995).
The observations make clear that statements on possible causal relationships between heavy physical labour and effects on cardiovascular morbidity are not easy to substantiate. The problem with this type of investigation clearly lies in the difficulty in measuring and assessing “hard work” and in excluding preselections (healthy worker effect). Prospective cohort studies are needed on the chronic effects of selected forms of physical work and also on the effects of combined physical-mental or noise stress on selected functional areas of the cardiovascular system.
It is paradoxical that the result of reducing heavy dynamic muscle work—until now greeted as a significant improvement in the level of strain in the modern workplace—possibly results in a new, significant health problem in modern industrial society. From the occupational medicine perspective, one might conclude that static physical strain on the muscle-skeleton system with lack of movement, presents a much greater health risk than previously assumed, according to the results of studies to date.
Where monotonous improper strains cannot be avoided, counterbalancing with free-time sports activities of comparable duration should be encouraged (e.g., swimming, bicycling, walking and tennis).
Heat and Cold
Exposure to extreme heat or cold is thought to influence cardiovascular morbidity (Kristensen 1989; Kristensen 1994). The acute effects of high outside temperatures or cold on the circulatory system are well documented. An increase in mortality as a result of cardiovascular diseases, mostly heart attacks and strokes, was observed at low temperatures (under +10°C) in the winter in countries at northern latitudes (Curwen 1991; Douglas, Allan and Rawles 1991; Kristensen 1994; Kunst, Looman and Mackenbach 1993). Pan, Li and Tsai (1995) found an impressive U-shaped relationship between outside temperature and mortality rates for coronary heart disease and strokes in Taiwan, a subtropical country, with a similarly falling gradient between +10°C and +29°C and a sharp increase thereafter at over +32°C. The temperature at which the lowest cardiovascular mortality was observed is higher in Taiwan than in countries with colder climates. Kunst, Looman and Mackenbach found in the Netherlands a V-shaped relationship between total mortality and outside temperature, with the lowest mortality at 17°C. Most cold-related deaths occurred in people with cardiovascular diseases, and most heat-related deaths were associated with respiratory tract illnesses. Studies from the United States (Rogot and Padgett 1976) and other countries (Wyndham and Fellingham 1978) show a similar U-shaped relationship, with the lowest heart attack and stroke mortality at outside temperatures around 25 to 27°C.
It is not yet clear how these results should be interpreted. Some authors have concluded that a causal relationship possibly exists between temperature stress and the pathogenesis of cardiovascular diseases (Curwen and Devis 1988; Curwen 1991; Douglas, Allan and Rawles 1991; Khaw 1995; Kunst, Looman and Mackenbach 1993; Rogot and Padgett 1976; Wyndham and Fellingham 1978). This hypothesis was supported by Khaw in the following observations:
- Temperature proved to be the strongest, acute (day to day) predictor for cardiovascular mortality under the parameters which were handled differently, such as seasonal environmental changes and factors like air pollution, sunlight exposure, incidence of flu and nutrition. This speaks against the assumption that temperature acts only as a substitute variable for other detrimental environmental conditions.
- The consistency of the connection in various countries and population groups, over time and in different age groups, is furthermore convincing.
- Data from clinical and laboratory research suggests various biologically plausible pathomechanisms, including effects of changing temperature on haemostasis, blood viscosity, lipid levels, the sympathetic nervous system and vasoconstriction (Clark and Edholm 1985; Gordon, Hyde and Trost 1988; Keatinge et al. 1986; Lloyd 1991; Neild et al. 1994; Stout and Grawford 1991; Woodhouse, Khaw and Plummer 1993b; Woodhouse et al. 1994).
Exposure to cold increases blood pressure, blood viscosity and heart rate (Kunst, Looman and Mackenbach 1993; Tanaka, Konno and Hashimoto 1989; Kawahara et al. 1989). Studies by Stout and Grawford (1991) and Woodhouse and co-workers (1993; 1994) show that fibrinogens, blood clotting factor VIIc and lipids were higher among older people in the winter.
An increase in blood viscosity and serum cholesterol was found with exposure to high temperatures (Clark and Edholm 1985; Gordon, Hyde and Trost 1988; Keatinge et al. 1986). According to Woodhouse, Khaw and Plummer (1993a), there is a strong inverse correlation between blood pressure and temperature.
Still unclear is the decisive question of whether long-term exposure to cold or heat results in lasting increased risk of cardiovascular disease, or whether exposure to heat or cold increases the risk for an acute manifestation of cardiovascular diseases (e.g., a heart attack, a stroke) in connection with the actual exposure (the “triggering effect”). Kristensen (1989) concludes that the hypothesis of an acute risk increase for complications from cardiovascular disease in people with underlying organic disease is confirmed, whereas the hypothesis of a chronic effect of heat or cold can neither be confirmed nor rejected.
There is little, if any, epidemiological evidence to support the hypothesis that the risk of cardiovascular disease is higher in populations with an occupational, long-term exposure to high temperature (Dukes-Dobos 1981). Two recent cross-section studies focused on metalworkers in Brazil (Kloetzel et al. 1973) and a glass factory in Canada (Wojtczak-Jaroszowa and Jarosz 1986). Both studies found a significantly increased prevalence of hypertension among those subject to high temperatures, which increased with the duration of the hot work. Presumed influences of age or nutrition could be excluded. Lebedeva, Alimova and Efendiev (1991) studied mortality among workers in a metallurgical company and found high mortality risk among people exposed to heat over the legal limits. The figures were statistically significant for blood diseases, high blood pressure, ischemic heart disease and respiratory tract diseases. Karnaukh et al. (1990) report an increased incidence of ischemic heart disease, high blood pressure and haemorrhoids among workers in hot casting jobs. The design of this study is not known. Wild et al. (1995) assessed the mortality rates between 1977 and 1987 in a cohort study of French potash miners. The mortality from ischemic heart disease was higher for underground miners than for above-ground workers (relative risk = 1.6). Among people who were separated from the company for health reasons, the ischemic heart disease mortality was five times higher in the exposed group as compared to the above-ground workers. A cohort mortality study in the United States showed a 10% lower cardiovascular mortality for heat-exposed workers as compared to the non-exposed control group. In any case, among those workers who were in heat-exposed jobs less than six months, the cardiovascular mortality was relatively high (Redmond, Gustin and Kamon 1975; Redmond et al. 1979). Comparable results were cited by Moulin et al. (1993) in a cohort study of French steel workers. These results were attributed to a possible healthy worker effect among the heat-exposed workers.
There are no known epidemiological studies of workers exposed to cold (e.g., cooler, slaughterhouse or fishery workers). It should be mentioned that cold stress is not only a function of temperature. The effects described in the literature appear to be influenced by a combination of factors like muscle activity, dress, dampness, drafts and possibly poor living conditions. Workplaces with exposure to cold should pay special attention to appropriate dress and avoiding drafts (Kristensen 1994).
Vibration
Hand-arm vibration stress
It is long known and well documented that vibrations transmitted to the hands by vibrating tools can cause peripheral vascular disorders in addition to damage to the muscle and skeletal system, and peripheral nerve-function disorders in the hand-arm area (Dupuis et al. 1993; Pelmear, Taylor and Wasserman 1992). The “white finger disease”, first described by Raynaud, appears with higher prevalency rates among exposed populations, and is recognized as an occupational disease in many countries.
Raynaud’s phenomenon is marked by an attack with vasospastic reduced fusion of all or some fingers, with the exception of the thumbs, accompanied by sensibility disorders in the affected fingers, feelings of cold, pallor and paraesthesia. After the exposure ends, circulation resumes, accompanied by a painful hyperaemia.
It is assumed that endogenous factors (e.g., in the sense of a primary Raynaud’s phenomenon) as well as exogenous exposures can be held responsible for the occurrence of a vibration-related vasospastic syndrome (VVS). The risk is clearly greater with vibrations from machines with higher frequencies (20 to over 800 Hz) than with machines that produce low-frequency vibrations. The amount of static strain (gripping and pressing strength) appears to be a contributing factor. The relative significance of cold, noise and other physical and psychological stressors, and heavy nicotine consumption is still unclear in the development of the Raynaud’s phenomenon.
The Raynaud’s phenomenon is pathogenetically based on a vasomotor disorder. Despite a large number of studies on functional, non-invasive (thermography, plethysmography, capillaroscopy, cold test) and invasive examinations (biopsy, arteriography), the pathophysiology of the vibration-related Raynaud’s phenomenon is not yet clear. Whether the vibration directly causes damage to the vascular musculature (a “local fault”), or whether it is a vasoconstriction as a result of sympathetic hyperactivity, or whether both these factors are necessary, is at present still unclear (Gemne 1994; Gemne 1992).
The work-related hypothenar hammer syndrome (HHS) should be distinguished in the differential diagnosis from vibration-caused Raynaud’s phenomenon. Pathogenetically this is a chronic-traumatic damage to the artery ulnaris (intima lesion with subsequent thrombosization) in the area of the superficial course above the unciform bone (os hamatum). HHS is caused by long-term mechanical effects in the form of external pressure or blows, or by sudden strain in the form of mechanical partial body vibrations (often combined with persistent pressure and the effects of impacts). For this reason, HHS can occur as a complication or in connection with a VVS (Kaji et al. 1993; Marshall and Bilderling 1984).
In addition to the early and, for exposure against hand-arm vibration, specific peripheral vascular effects, of particular scientific interest are the so-called non-specific chronic changes of autonomous regulations of the organ systems—for example, of the cardiovascular system, perhaps provoked by vibration (Gemne and Taylor 1983). The few experimental and epidemiological studies of possible chronic effects of hand-arm vibration give no clear results confirming the hypothesis of possible vibration-related endocrine and cardiovascular function disorders of the metabolic processes, cardiac functions or blood pressure (Färkkilä, Pyykkö and Heinonen 1990; Virokannas 1990) other than that the activity of the adrenergic system is increased from exposure to vibration (Bovenzi 1990; Olsen 1990). This applies to vibration alone or in combination with other strain factors like noise or cold.
Whole-body vibration stress
If whole-body mechanical vibrations have an effect on the cardio- vascular system, then a series of parameters such as heart rate, blood pressure, cardiac output, electrocardiogram, plethysmo- gram and certain metabolic parameters must show corresponding reactions. Conclusions on this are made difficult for the method- ological reason that these circulation quantifications do not react specifically to vibrations, but can also be influenced by other simultaneous factors. Increases in heart rate are apparent only under very heavy vibration loads; the influence on blood pressure values shows no systematic results and electrocardiographic (ECG) changes are not significantly differentiable.
Peripheral circulatory disorders resulting from vasoconstriction have been less researched and appear weaker and of shorter duration than those from hand-arm vibrations, which are marked by an effect on the grasping strength of the fingers (Dupuis and Zerlett 1986).
In most studies the acute effects of whole-body vibrations on the cardiovascular system of vehicle drivers were found to be relatively weak and temporary (Dupius and Christ 1966; Griffin 1990).
Wikström, Kjellberg and Landström (1994), in a comprehensive overview, cited eight epidemiological studies from 1976 to 1984 that examined the connection between whole-body vibrations and cardiovascular diseases and disorders. Only two of these studies found a higher prevalence of such illnesses in the group exposed to vibrations, but none where this was interpreted as the effect of whole-body vibrations.
The view is widely accepted that changes of physiological functions through whole-body vibrations have only a very limited effect on the cardiovascular system. Causes as well as mechanisms of the reaction of the cardiovascular system to whole-body vibrations are not yet sufficiently known. At present there is no basis to assume that whole-body vibrations per se contribute to the risk of diseases of the cardiovascular system. But attention should be paid to the fact that this factor very often is combined with exposure to noise, inactivity (sitting work) and shift work.
Ionizing Radiation, Electromagnetic Fields, Radioand Microwaves, Ultra- and Infrasound
Many case studies and a few epidemiological studies have drawn attention to the possibility that ionizing radiation, introduced to treat cancer or other diseases, may promote the development of arteriosclerosis and thereby increase the risk for coronary heart disease and also other cardiovascular diseases (Kristensen 1989; Kristensen 1994). Studies on the incidence of cardiovascular diseases in occupational groups exposed to ionizing radiation are not available.
Kristensen (1989) reports on three epidemiological studies from the early 1980s on the connection between cardiovascular diseases and exposure to electromagnetic fields. The results are contradic- tory. In the 1980s and 1990s the possible effects of electrical and magnetic fields on human health have attracted increasing atten- tion from people in occupational and environmental medicine. Partially contradictory epidemiological studies that looked for cor- relations between occupational and/or environmental exposure to weak, low-frequency electrical and magnetic fields, on the one hand, and the onset of health disorders on the other, aroused considerable attention. In the foreground of the numerous experi- mental and few epidemiological studies stand possible long-term effects such as carcinogenicity, teratogenicity, effects on the im- mune or hormone systems, on reproduction (with special atten- tion to miscarriages and defects), as well as to “hypersensitivity to electricity” and neuro-psychological behavioural reactions. Poss- ible cardiovascular risk is not being discussed at present (Gamber- ale 1990; Knave 1994).
Certain immediate effects of low-frequency magnetic fields on the organism that have been scientifically documented through in vitro and in vivo examinations of low to high field strengths should be mentioned in this connection (UNEP/WHO/IRPA 1984; UNEP/WHO/IRPA 1987). In the magnetic field, such as in the blood stream or during heart contraction, charged carriers lead to induction of electrical fields and currents. Thus the electrical voltage that is created in a strong static magnetic field over the aorta near the heart during coronary activity can amount to 30 mV at a flow thickness of 2 Tesla (T), and induction values over 0.1 T were detected in the ECG. But effects on the blood pressure, for example, were not found. Magnetic fields that change with time (intermittent magnetic fields) induce electrical eddy fields in biological objects that can for example arouse nerve and muscle cells in the body. No certain effect appears with electrical fields or induced currents under 1 mA/m2. Visual (induced with magnetophosphene) and nervous effects are reported at 10 to 100 mA/m2. Extrasystolic and heart chamber fibrillations appear at over 1 A/m2. According to currently available data, no direct health threat is to be expected for short-term whole-body exposure up to 2 T (UNEP/WHO/IRPA 1987). However, the danger threshold for indirect effects (e.g., from the magnetic field force action on ferromagnetic materials) lies lower than that for direct effects. Precautionary measures are thus required for persons with ferromagnetic implants (unipolar pacemakers, magnetizable aneurysm clips, haemoclips, artificial heart valve parts, other electrical implants, and also metal fragments). The danger threshold for ferromagnetic implants begins at 50 to 100 mT. The risk is that injuries or bleeding can result from migration or pivotal motions, and that functional capacities (e.g., of heart valves, pacemakers and so on) can be affected. In facilities in research and industry with strong magnetic fields, some authors advise medical surveillance examinations for people with cardiovascular diseases, including high blood pressure, in jobs where the magnetic field exceeds 2 T (Bernhardt 1986; Bernhardt 1988). Whole-body exposure of 5 T can lead to magnetoelectrodynamic and hydrodynamic effects on the circulatory system, and it should be assumed that short-term whole-body exposure of 5 T causes health hazards, especially for people with cardiovascular diseases, including high blood pressure (Bernhardt 1988; UNEP/WHO/ IRPA 1987).
Studies that examine the various effects of radio and microwaves have found no detrimental effects to health. The possibility of cardiovascular effects from ultrasound (frequency range between 16 kHz and 1 GHz) and infrasound (frequency range >>20 kHz) are discussed in the literature, but the empirical evidence is very slight (Kristensen 1994).
Chemical Hazardous Material
Despite numerous studies, the role of chemical factors in causing cardiovascular diseases is still disputed, but probably is small. The calculation of the aetiological role of chemical occupational factors for cardiovascular diseases for the Danish population resulted in a value under 1% (Kristensen 1994). For a few materials such as carbon disulphide and organic nitrogen compounds, the effect on the cardiovascular system is generally recognized (Kristensen 1994). Lead seems to affect blood pressure and cerebrovascular morbidity. Carbon monoxide (Weir and Fabiano 1982) undoubtedly has acute effects, especially in provoking angina pectoris in pre-existing ischaemia, but probably does not increase the risk of the underlying arteriosclerosis, as was long suspected. Other materials like cadmium, cobalt, arsenic, antimony, beryllium, organic phosphates and solvents are under discussion, but not sufficiently documented as yet. Kristensen (1989, 1994) gives a critical overview. A selection of relevant activities and industrial branches can be found in Table 1.
Table 1. Selection of activities and industrial branches that may be associated with cardiovascular hazards
|
Hazardous material |
Occupational branch affected/use |
|
Carbon disulphide (CS2 ) |
Rayon and synthetic fiber fabrication, rubber, |
|
Organic nitro-compounds |
Explosives and munitions manufacture, |
|
Carbon monoxide (CO) |
Employees in large industrial combustion |
|
Lead |
Smelting of lead ore and secondary raw |
|
Hydrocarbons, halogenated hydrocarbons |
Solvents (paints, lacquer) |
The exposure and effect data of important studies for carbon disulphide (CS2), carbon monoxide (CO) and nitroglycerine are given in the chemical section of the Encyclopaedia. This listing makes clear that problems of inclusion, combined exposures, varying consideration of compounding factors, changing target sizes and assessment strategies play a considerable role in the findings, so that uncertainties remain in the conclusions of these epidemiological studies.
In such situations clear pathogenetic conceptions and knowledge can support the suspected connections and thereby contribute to deriving and substantiating the consequences, including preventive measures. The effects of carbon disulphide are known on lipids and carbohydrate metabolism, on thyroid functioning (triggering hypothyroidism) and on coagulation metabolism (promoting thrombocyte aggregation, inhibiting plasminogen and plasmin activity). Changes in blood pressure such as hypertension are mostly traceable to vascular-based changes in the kidney, a direct causal link to high blood pressure due to carbon disulphide has not yet been excluded for certain, and a direct (reversible) toxic effect is suspected on the myocardium or an interference with the catecholamine metabolism. A successful 15-year intervention study (Nurminen and Hernberg 1985) documents the reversibility of the effect on the heart: a reduction in exposure was followed almost immediately by a decrease in cardiovascular mortality. In addition to the clearly direct cardiotoxic effects, arteriosclerotic changes in the brain, eye, kidney and coronary vasculature that can be considered the basis of encephalopathies, aneurysms in the retina area, nephropathies and chronic ischaemic heart disease have been proven among those who are exposed to CS2. Ethnic and nutritionally related components interfere in the pathomechanism; this was made clear in the comparative studies of Finnish and Japanese viscous rayon workers. In Japan, vascular changes in the area of the retina were found, whereas in Finland the cardiovascular effects dominated. Aneurysmatic changes in the retinal vasculature were observed at carbon disulphide concentrations under 3 ppm (Fajen, Albright and Leffingwell 1981). Reducing the exposure to 10 ppm clearly reduced cardiovascular mortality. This does not definitively clarify whether cardiotoxic effects are definitely excluded at doses under 10 ppm.
The acute toxic effects of organic nitrates involve widening of the vasa, accompanied by dropping blood pressure, increased heart rate, spotty erythema (flush), orthostatic dizziness and headaches. Since the half-life of the organic nitrate is short, the ailments soon subside. Normally, serious health considerations are not to be expected with acute intoxication. The so-called withdrawal syndrome appears when exposure is interrupted for employees with long-term exposure to organic nitrate, with a latency period of 36 to 72 hours. This includes ailments ranging from angina pectoris up to acute myocardial infarction and cases of sudden death. In the investigated deaths, often no coronary sclerotic changes were documented. The cause is therefore suspected to be “rebound vasospasm”. When the vasa-widening effect of the nitrate is removed, an autoregulative increase in resistance occurs in the vasa, including the coronary arteriae, which produces the above-mentioned results. In certain epidemiological studies, suspected associations between exposure duration and intensity of organic nitrate and ischaemic heart disease are considered uncertain, and pathogenetic plausibility for them is lacking.
Concerning lead, metallic lead in dust form, the salts of diva- lent lead and organic lead compounds are toxicologically impor- tant. Lead attacks the contractile mechanism of the vasa muscle cells and causes vascular spasms, which are considered causes for a series of symptoms of lead intoxication. Among these is tem- porary hypertension that appears with lead colic. Lasting high blood pressure from chronic lead intoxication can be explained by vasospasms as well as kidney changes. In epidemiological studies an association has been observed with longer exposure times between lead exposure and increased blood pressure, as well as an increased incidence of cerebrovascular diseases, whereas there was little evidence of increased cardiovascular diseases.
Epidemiological data and pathogenetic investigations to date have produced no clear results on the cardiovascular toxicity of other metals like cadmium, cobalt and arsenic. However, the hypothesis that halogenated hydrocarbon acts as a myocardial irritant is considered certain. The triggering mechanism of occasionally life-threatening arrhythmia from these materials presumably comes from myocardial sensitivity to epinephrine, which works as a natural carrier for the autonomic nervous system. Still being discussed is whether a direct cardiac effect exists such as reduced contractility, suppression of impulse formation centres, impulse transmission, or reflex impairment resulting from irrigation in the upper airway region. The sensitizing potential of hydrocarbons apparently depends on the degree of halogenation and on the type of the halogen contained, whereas chlorine-substituted hydrocarbons are supposed to have a stronger sensitizing effect than fluoride compounds. The maximum myocardial effect for hydrocarbons containing chlorine occurs at around four chlorine atoms per molecule. Short chain non-substituted hydrocarbons have a higher toxicity than ones with longer chains. Little is known about the arrhythmia-triggering dosage of the individual substances, as the reports on humans predominantly are case descriptions with exposure to high concentrations (accidental exposure and “sniffing”). According to Reinhardt et al. (1971), benzene, heptane, chloroform and trichlorethylene are especially sensitizing, whereas carbon tetrachloride and halothane have less arrhythmogenic effect.
The toxic effects of carbon monoxide result from tissue hypoxaemia, which results from the increased formation of CO-Hb (CO has 200-times greater affinity to haemoglobin than does oxygen) and the resulting reduced release of oxygen to the tissues. In addition to the nerves, the heart is one of the organs that react especially critically to such hypoxaemia. The resulting acute heart ailments have been repeatedly examined and described according to exposure time, breathing frequency, age and previous illnesses. Whereas among healthy subjects, cardiovascular effects first appear at CO-Hb concentrations of 35 to 40%, angina pectoris ailments could be experimentally produced in patients with ischaemic heart disease already at CO-Hb concentrations between 2 and 5% during physical exposure (Kleinman et al. 1989; Hinderliter et al. 1989). Deadly infarctions were observed among those with previous afflictions at 20% CO-Hb (Atkins and Baker 1985).
The effects of long-term exposure with low CO concentrations are still subject to controversy. Whereas experimental studies on animals possibly showed an atherogenic effect by way of hypoxia of the vasa walls or by direct CO effect on the vasa wall (increased vascular permeability), the flow characteristics of the blood (strengthened thrombocyte aggregation), or lipid metabolism, the corresponding proof for humans is lacking. The increased cardiovascular mortality among tunnel workers (SMR 1.35, 95% CI 1.09-1.68) can more likely be explained by acute exposure than from chronic CO effects (Stern et al. 1988). The role of CO in the cardiovascular effects of cigarette smoking is also not clear.
Biological Hazards
“A biological hazardous material can be defined as a biological material capable of self-replication that can cause harmful effects in other organisms, especially humans” (American Industrial Hygiene Association 1986).
Bacteria, viruses, fungi and protozoa are among the biological hazardous materials that can harm the cardiovascular system through contact that is intentional (introduction of technology-related biological materials) or unintentional (non-technology-related contamination of work materials). Endotoxins and mycotoxins may play a role in addition to the infectious potential of the micro-organism. They can themselves be a cause or contributing factor in a developing disease.
The cardiovascular system can either react as a complication of an infection with a localized organ participation—vasculitis (inflammation of the blood vessels), endocarditis (inflammation of the endocardium, primarily from bacteria, but also from fungus and protozoa; acute form can follow septic occurrence; subacute form with generalization of an infection), myocarditis (heart muscle inflammation, caused by bacteria, viruses and protozoa), pericarditis (pericardium inflammation, usually accompanies myocarditis), or pancarditis (simultaneous appearance of endocarditis, myocarditis and pericarditis)—or be drawn as a whole into a systemic general illness (sepsis, septic or toxic shock).
The participation of the heart can appear either during or after the actual infection. As pathomechanisms the direct germ colon- ization or toxic or allergic processes should be considered. In addition to type and virulence of the pathogen, the efficiency of the immune system plays a role in how the heart reacts to an infection. Germ-infected wounds can induce a myo- or endo- carditis with, for example, streptococci and staphylococci. This can affect virtually all occupational groups after a workplace accident.
Ninety per cent of all traced endocarditis cases can be attributed to strepto- or staphylococci, but only a small portion of these to accident-related infections.
Table 1 gives an overview of possible occupation-related infectious diseases that affect the cardiovascular system.
Table 1. Overview of possible occupation-related infectious diseases that affect the cardiovascular system
|
Disease |
Effect on heart |
Occurrence/frequency of effects on heart in case of disease |
Occupational risk groups |
|
AIDS/HIV |
Myocarditis, Endocarditis, Pericarditis |
42% (Blanc et al. 1990); opportunistic infections but also by the HIV virus itself as lymphocytic myocarditis (Beschorner et al. 1990) |
Personnel in health and welfare services |
|
Aspergillosis |
Endocarditis |
Rare; among those with suppressed immune system |
Farmers |
|
Brucellosis |
Endocarditis, Myocarditis |
Rare (Groß, Jahn and Schölmerich 1970; Schulz and Stobbe 1981) |
Workers in meatpacking and animal husbandry, farmers, veterinarians |
|
Chagas’ disease |
Myocarditis |
Varying data: 20% in Argentina (Acha and Szyfres 1980); 69% in Chile (Arribada et al. 1990); 67% (Higuchi et al. 1990); chronic Chagas’ disease always with myocarditis (Gross, Jahn and Schölmerich 1970) |
Business travelers to Central and South America |
|
Coxsackiessvirus |
Myocarditis, Pericarditis |
5% to 15% with Coxsackie-B virus (Reindell and Roskamm 1977) |
Personnel in health and welfare services, sewer workers |
|
Cytomegaly |
Myocarditis, Pericarditis |
Extremely rare, especially among those with suppressed immune system |
Personnel who work with children (especially small children), in dialysis and transplant departments |
|
Diphtheria |
Myocarditis, Endocarditis |
With localized diphtheria 10 to 20%, more common with progressive D. (Gross, Jahn and Schölmerich 1970), especially with toxic development |
Personnel who work with children and in health services |
|
Echinococcosis |
Myocarditis |
Rare (Riecker 1988) |
Forestry workers |
|
Epstein-Barr virus infections |
Myocarditis, Pericarditis |
Rare; especially among those with defective immune system |
Health and welfare personnel |
|
Erysipeloid |
Endocarditis |
Varying data from rare (Gross, Jahn and Schölmerich 1970; Riecker 1988) to 30% (Azofra et al. 1991) |
Workers in meatpacking, fish processing, fishers, veterinarians |
|
Filariasia |
Myocarditis |
Rare (Riecker 1988) |
Business travelers in endemic areas |
|
Typhus among other rickettsiosis (exclud- ing Q fever) |
Myocarditis, Vasculitis of small vasa |
Data varies, through direct pathogen, toxic or resistance-reduction during fever resolution |
Business travelers in endemic areas |
|
Early summer meningo-encephalitis |
Myocarditis |
Rare (Sundermann 1987) |
Forestry workers, gardeners |
|
Yellow fever |
Toxic damage to vasa (Gross, Jahn and Schölmerich 1970), Myocarditis |
Rare; with serious cases |
Business travelers in endemic areas |
|
Haemorrhagic fever (Ebola, Marburg, Lassa, Dengue, etc.) |
Myocarditis and endocardial bleedings through general hemorrhage, cardiovascular failure |
No information available |
Health service employees in affected areas and in special laboratories, and workers in animal husbandry |
|
Influenza |
Myocarditis, Hemorrhages |
Data varying from rare to often (Schulz and Stobbe 1981) |
Health service employees |
|
Hepatitis |
Myocarditis (Gross, Willensand Zeldis 1981; Schulzand Stobbe 1981) |
Rare (Schulz and Stobbe 1981) |
Health and welfare employees, sewage and waste-water workers |
|
Legionellosis |
Pericarditis, Myocarditis, Endocarditis |
If occurs, probably rare (Gross, Willens and Zeldis 1981) |
Maintenance personnel in air conditioning, humidifiers, whirlpools, nursing staff |
|
Leishmaniasis |
Myocarditis (Reindell and Roskamm 1977) |
With visceral leishmaniasis |
Business travelers to endemic areas |
|
Leptospirosis (icteric form) |
Myocarditis |
Toxic or direct pathogen infection (Schulz and Stobbe 1981) |
Sewage and waste-water workers, slaughterhouse workers |
|
Listerellosis |
Endocarditis |
Very rare (cutaneous listeriosis predominant as occupational disease) |
Farmers, veterinarians, meat-processing workers |
|
Lyme disease |
In stage 2: Myocarditis Pancarditis In stage 3: Chronic carditis |
8% (Mrowietz 1991) or 13% (Shadick et al. 1994) |
Forestry workers |
|
Malaria |
Myocarditis |
Relatively frequent with malaria tropica (Sundermann 1987); direct infection of capillaries |
Business travelers in endemic areas |
|
Measles |
Myocarditis, Pericarditis |
Rare |
Personnel in health service and who work with children |
|
Foot-and-mouth disease |
Myocarditis |
Very rare |
Farmers, animal husbandry workers, (especially with cloven- hoofed animals) |
|
Mumps |
Myocarditis |
Rare—under 0.2-0.4% (Hofmann 1993) |
Personnel in health service and who work with children |
|
Mycoplasma- pneumonia infections |
Myocarditis, Pericarditis |
Rare |
Health service and welfare employees |
|
Ornithosis/Psittacosis |
Myocarditis, Endocarditis |
Rare (Kaufmann and Potter 1986; Schulz and Stobbe 1981) |
Ornamental bird and poultry raisers, pet shop workers, veterinarians |
|
Paratyphus |
Interstitial myocarditis |
Especially among older and very sick as toxic damage |
Development aid workers in tropics and subtropics |
|
Poliomyelitis |
Myocarditis |
Common in serious cases in the first and second weeks |
Health service employees |
|
Q fever |
Myocarditis, Endocarditis, Pericarditis |
Possible to age 20 after acute disease (Behymer and Riemann 1989); data from rare (Schulz and Stobbe 1981; Sundermann 1987) to 7.2% (Conolly et al. 1990); more frequent (68%) among chronic Q-fever with weak immune system or pre-existing heart disease (Brouqui et al. 1993) |
Animal husbandry workers, veterinarians, farmers, possibly also slaughterhouse and dairy workers |
|
Rubella |
Myocarditis, Pericarditis |
Rare |
Health service and child care employees |
|
Relapsing fever |
Myocarditis |
No information available |
Business travelers and health service workers in tropics and subtropics |
|
Scarlet fever and other streptococcal infections |
Myocarditis, Endocarditis |
In 1 to 2.5% rheumatic fever as complication (Dökert 1981), then 30 to 80% carditis (Sundermann 1987); 43 to 91% (al-Eissa 1991) |
Personnel in health service and who work with children |
|
Sleeping sickness |
Myocarditis |
Rare |
Business travelers to Africa between 20° Southern and Northern parallels |
|
Toxoplasmosis |
Myocarditis |
Rare, especially among those with weak immune systems |
People with occupational contact with animals |
|
Tuberculosis |
Myocarditis, Pericarditis |
Myocarditis especially in conjunction with miliary tuberculosis, pericarditis with high tuberculosis prevalence to 25%, otherwise 7% (Sundermann 1987) |
Health service employees |
|
Typhus abdominalis |
Myocarditis |
Toxic; 8% (Bavdekar et al. 1991) |
Development aid workers, personnel in microbiological laboratories (especially stool labs) |
|
Chicken pox, Herpes zoster |
Myocarditis |
Rare |
Employees in health service and who work with children |
Introduction
Cardiovascular diseases (CVDs) are among the most common causes of illness and death in the working population, particularly in industrialized countries. They are also increasing in developing countries (Wielgosz 1993). In the industrialized countries, 15 to 20% of all working people will suffer from a cardiovascular dis- order sometime during their working lives and the frequency climbs sharply with age. Among those between 45 to 64 years of age, more than a third of the deaths among men and more than a quarter of deaths among women are caused by this group of diseases (see table 1). In recent years, CVDs have become the most frequent cause of death among post-menopausal women.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Because of their complex aetiology, only a very small pro- portion of the cases of cardiovascular disease are recognized as occupational. Many countries, however, recognize that occu- pational exposures contribute to CVDs (sometimes referred to as work-related diseases). Working conditions and job demands play an important role in the multifactorial process that leads to these diseases, but ascertaining the role of the individual causal com- ponents is very difficult. The components interact in close, shifting relationships and often the disease is triggered by a combination or accumulation of different causal factors, including those that are work related.
The reader is referred to the standard cardiology texts for details of the epidemiology, pathophysiology, diagnosis and treatment of cardiovascular diseases. This chapter will focus on those aspects of cardiovascular disease that are particularly relevant in the workplace and are likely to be influenced by factors in the job and work environment.
Cardiovascular Morbidity and Mortality in the Workforce
In the following article, the term cardiovascular diseases (CVDs) refers to organic and functional disorders of the heart and circu- latory system, including the resultant damage to other organ systems, which are classified under numbers 390 to 459 in the 9th revision of the International Classification of Diseases (ICD) (World Health Organization (WHO) 1975). Based essentially on international statistics assembled by the WHO and data collected in Germany, the article discusses the prevalence of CVDs, new disease rates, and frequency of deaths, morbidity and disability.
Definition and Prevalence in the Working-Age Population
Coronary artery disease (ICD 410-414) resulting in ischaemia of the myocardium is probably the most significant CVD in the working population, particularly in industrialized countries. This condition results from a constriction in the vascular system that supplies the heart muscle, a problem caused primarily by arteriosclerosis. It affects 0.9 to 1.5% of working-age men and 0.5 to 1.0% of women.
Inflammatory diseases (ICD 420-423) may involve the endo- cardium, the heart valves, the pericardium and/or the heart muscle (myocardium) itself. They are less common in industrialized countries, where their frequency is well below 0.01% of the adult population, but are seen more frequently in developing countries, perhaps reflecting the greater prevalence of nutritional disorders and infectious diseases.
Heart rhythm disorders (ICD 427) are relatively rare, although much media attention has been given to recent instances of disability and sudden death among prominent professional athletes. Although they can have a significant impact on the ability to work, they are often asymptomatic and transitory.
The myocardiopathies (ICD 424) are conditions which involve enlargement or thickening of the heart musculation, effectively narrowing the vessels and weakening the heart. They have attracted more attention in recent years, largely because of improved methods of diagnosis, although their pathogenesis is often obscure. They have been attributed to infections, metabolic diseases, immunologic disorders, inflammatory diseases involving the capillaries and, of particular importance in this volume, to toxic exposures in the workplace. They are divided into three types:
- dilative—the most common form (5 to 15 cases per 100,000 people), which is associated with the functional weakening of the heart
- hypertrophic—thickening and enlargement of the myocardium resulting in relative insufficiency of the coronary arteries
- restrictive—a rare type in which myocardial contractions are limited.
Hypertension (ICD 401-405) (increased systolic and/or diastolic blood pressure) is the most common circulatory disease, being found among 15 to 20% of working people in industrialized countries. It is discussed in greater detail below.
Atherosclerotic changes in the major blood vessels (ICD 440), often associated with hypertension, cause disease in the organs they serve. Foremost among these is cerebrovascular disease (ICD 430-438), which may result in a stroke due to infarction and/or haemorrhage. This occurs in 0.3 to 1.0% of working people, most commonly among those aged 40 and older.
Atherosclerotic diseases, including coronary artery disease, stroke and hypertension, by far the most common cardiovascular diseases in the working population, are multifactorial in origin and have their onset early in life. They are of importance in the workplace because:
- so large a proportion of the workforce has an asymptomatic or unrecognized form of cardiovascular disease
- the development of that disease may be aggravated or acute symptomatic events precipitated by working conditions and job demands
- the acute onset of a symptomatic phase of the cardiovascular disease is often attributed to the job and/or the workplace environment
- most individuals with an established cardiovascular disease are capable of working productively, albeit, sometimes, only after effective rehabilitation and job retraining
- the workplace is a uniquely propitious arena for primary and secondary preventive programmes.
Functional circulatory disorders in the extremities (ICD 443) include Raynaud’s disease, short-term pallor of the fingers, and are relatively rare. Some occupational conditions, such as frostbite, long-term exposure to vinyl chloride and hand-arm exposure to vibration can induce these disorders.
Varicosities in the leg veins (ICD 454), often improperly dismissed as a cosmetic problem, are frequent among women, especially during pregnancy. While a hereditary tendency to weakness of the vein walls may be a factor, they are usually associated with long periods of standing in one position without movement, during which the static pressure within the veins is increased. The result- ant discomfort and leg oedema often dictate change or modifi- cation of the job.
Annual incidence rates
Among the CVDs, hypertension has the highest annual new case rate among working people aged 35 to 64. New cases develop in approximately 1% of that population every year. Next in frequency are coronary heart disease (8 to 92 new cases of acute heart attack per 10,000 men per year, and 3 to 16 new cases per 10,000 women per year) and stroke (12 to 30 cases per 10,000 men per year, and 6 to 30 cases per 10,000 women per year). As demonstrated by global data collected by the WHO-Monica project (WHO-MONICA 1994; WHO-MONICA 1988), the lowest new incidence rates for heart attack were found among men in China and women in Spain, while the highest rates were found among both men and women in Scotland. The significance of these data is that in the population of working age, 40 to 60% of heart attack victims and 30 to 40% of stroke victims do not survive their initial episodes.
Mortality
Within the primary working ages of 15 to 64, only 8 to 18% of deaths from CVDs occur prior to age 45. Most occur after age 45, with the annual rate increasing with age. The rates, which have been changing, vary considerably from country to country (WHO 1994b).
Table 1 shows the death rates for men and for women aged 45 to 54 and 55 to 64 for some countries. Note that the death rates for men are consistently higher than those for women of corresponding ages. Table 2 compares the death rates for various CVDs among people aged 55 to 64 in five countries.
Table 1. Mortality from cardiovascular diseases in 1991 and 1990 in the age groups 45-54 and 55-64 for selected countries.
|
Country |
Men |
Women |
||||||
|
45-54 Years |
55-64 Years |
45-54 Years |
55-64 Years |
|||||
|
Rate |
% |
Rate |
% |
Rate |
% |
Rate |
% |
|
|
Russia** |
528 |
36 |
1,290 |
44 |
162 |
33 |
559 |
49 |
|
Poland** |
480 |
38 |
1,193 |
45 |
134 |
31 |
430 |
42 |
|
Argentina* |
317 |
40 |
847 |
44 |
131 |
33 |
339 |
39 |
|
Britain** |
198 |
42 |
665 |
47 |
59 |
20 |
267 |
32 |
|
USA* |
212 |
35 |
623 |
40 |
83 |
24 |
273 |
31 |
|
Germany** |
181 |
29 |
597 |
38 |
55 |
18 |
213 |
30 |
|
Italy* |
123 |
27 |
404 |
30 |
41 |
18 |
148 |
25 |
|
Mexico** |
128 |
17 |
346 |
23 |
82 |
19 |
230 |
24 |
|
France** |
102 |
17 |
311 |
22 |
30 |
12 |
94 |
18 |
|
Japan** |
111 |
27 |
281 |
26 |
48 |
22 |
119 |
26 |
*1990. **1991. Rate=Deaths per 100,000 inhabitants. % is from all causes of death in the age group.
Table 2. Mortality rates from special cardiovascular diagnosis groups in the years 1991 and 1990 in the age group 55-64 for selected countries
|
Diagnosis group |
Russia (1991) |
USA (1990) |
Germany (1991) |
France (1991) |
Japan (1991) |
|||||
|
|
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
|
393–398 |
16.8 |
21.9 |
3.3 |
4.6 |
3.6 |
4.4 |
2.2 |
2.3 |
1.2 |
1.9 |
|
401–405 |
22.2 |
18.5 |
23.0 |
14.6 |
16.9 |
9.7 |
9.4 |
4.4 |
4.0 |
1.6 |
|
410 |
160.2 |
48.9 |
216.4 |
79.9 |
245.2 |
61.3 |
100.7 |
20.5 |
45.9 |
13.7 |
|
411–414 |
586.3 |
189.9 |
159.0 |
59.5 |
99.2 |
31.8 |
35.8 |
6.8 |
15.2 |
4.2 |
|
415–429 |
60.9 |
24.0 |
140.4 |
64.7 |
112.8 |
49.2 |
73.2 |
27.0 |
98.7 |
40.9 |
|
430–438 |
385.0 |
228.5 |
54.4 |
42.2 |
84.1 |
43.8 |
59.1 |
26.7 |
107.3 |
53.6 |
|
440 |
|
|
4.4 |
2.1 |
11.8 |
3.8 |
1.5 |
0.3 |
0.3 |
0.1 |
|
Total 390–459 |
1,290 |
559 |
623 |
273 |
597 |
213 |
311 |
94 |
281 |
119 |
Deaths per 100,000 inhabitants; M=male; F=female.
Work Disability and Early Retirement
Diagnosis-related statistics on time lost from work represent an important perspective on the impact of morbidity on the working population, even though the diagnostic designations are usually less precise than in cases of early retirement because of disability. The case rates, usually expressed in cases per 10,000 employees, provide an index of the frequency of the disease categories, while the average number of days lost per case indicates the relative seriousness of particular diseases. Thus, according to statistics on 10 million workers in western Germany compiled by the Allgemeinen Ortskrankenkasse, CVDs accounted for 7.7% of the total disability in 1991-92, although the number of cases for that period was only 4.6% of the total (Table 3). In some countries, where early retirement is provided when work ability is reduced due to illness, the pattern of disability mirrors the rates for different categories of CVD.
Table 3. Rate of cardiovascular disease among early pensioners* due to reduced ability to work (N = 576,079) and diagnosis-related work disability in the western part of Germany, 1990-92
|
Diagnosis group |
Main cause of illness |
Access to early retirement; number per 100,000 early retirees |
Average annual work disability 1990–92 |
||||
|
Cases per 100,000 employed |
Duration (days) per case |
||||||
|
Men |
Women |
Men |
Women |
Men |
Women |
||
|
390–392 |
Acute rheumatic fever |
16 |
24 |
49 |
60 |
28.1 |
32.8 |
|
393–398 |
Chronic rheumatic heart disease |
604 |
605 |
24 |
20 |
67.5 |
64.5 |
|
401–405 |
Hypertension, high blood pressure diseases |
4,158 |
4,709 |
982 |
1,166 |
24.5 |
21.6 |
|
410–414 |
Ischaemic heart diseases |
9,635 |
2,981 |
1,176 |
529 |
51.2 |
35.4 |
|
410, 412 |
Acute and existing myocardial infarction |
2,293 |
621 |
276 |
73 |
85.8 |
68.4 |
|
414 |
Coronary heart disease |
6,932 |
2,183 |
337 |
135 |
50.8 |
37.4 |
|
415–417 |
Pulmonary circulatory diseases |
248 |
124 |
23 |
26 |
58.5 |
44.8 |
|
420–429 |
Other non-rheumatic heart diseases |
3,434 |
1,947 |
645 |
544 |
36.3 |
25.7 |
|
420–423 |
Inflammatory heart diseases |
141 |
118 |
20 |
12 |
49.4 |
48.5 |
|
424 |
Heart valve disorders |
108 |
119 |
22 |
18 |
45.6 |
38.5 |
|
425 |
Myocardiopathy |
1,257 |
402 |
38 |
14 |
66.8 |
49.2 |
|
426 |
Stimulus performance disorder |
86 |
55 |
12 |
7 |
39.6 |
45.0 |
|
427 |
Cardiac rhythm disorder |
734 |
470 |
291 |
274 |
29.3 |
21.8 |
|
428 |
Cardiac insufficiency |
981 |
722 |
82 |
61 |
62.4 |
42.5 |
|
430–438 |
Cerebrovascular diseases |
4,415 |
2,592 |
172 |
120 |
75.6 |
58.9 |
|
440–448 |
Diseases of the arteries, arterioles and capillaries |
3,785 |
1,540 |
238 |
90 |
59.9 |
44.5 |
|
440 |
Arteriosclerosis |
2,453 |
1,090 |
27 |
10 |
71.7 |
47.6 |
|
443 |
Raynaud’s disease and other vascular diseases |
107 |
53 |
63 |
25 |
50.6 |
33.5 |
|
444 |
Arterial embolism and thrombosis |
219 |
72 |
113 |
34 |
63.3 |
49.5 |
|
451–456 |
Diseases of the veins |
464 |
679 |
1,020 |
1,427 |
22.9 |
20.3 |
|
457 |
Noninfectious diseases of the lymph nodes |
16 |
122 |
142 |
132 |
10.4 |
14.2 |
|
458 |
Hypotension |
29 |
62 |
616 |
1,501 |
9.4 |
9.5 |
|
459 |
Other circulatory diseases |
37 |
41 |
1,056 |
2,094 |
11.5 |
10.2 |
|
390–459 |
Total cardiovascular diseases |
26,843 |
15,426 |
6,143 |
7,761 |
29.6 |
18.9 |
*Early pensioned: Statutory pensions insurance for former Federal Republic of Germany, work disability AOK-West.
The Risk Factor Concept in Cardiovascular Disease
Risk factors are genetic, physiological, behavioural and socioeconomic characteristics of individuals that place them in a cohort of the population that is more likely to develop a particular health problem or disease than the rest of the population. Usually applied to multifactorial diseases for which there is no single precise cause, they have been particularly useful in identifying candidates for primary preventive measures and in assessing the effectiveness of the prevention programme in controlling the risk factors being targeted. They owe their development to large-scale prospective population studies, such as the Framingham study of coronary artery disease and stroke conducted in Framingham, Massachusetts, in the United States, other epidemiological studies, intervention studies and experimental research.
It should be emphasized that risk factors are merely expressions of probability—that is, they are not absolute nor are they diagnostic. Having one or more risk factors for a particular disease does not necessarily mean that an individual will develop the disease, nor does it mean that an individual without any risk factors will escape the disease. Risk factors are individual characteristics which affect that person’s chances of developing a particular disease or group of diseases within a defined future time period. Categories of risk factors include:
- somatic factors, such as high blood pressure, lipid metabolism disorders, overweight and diabetes mellitus
- behavioural factors, such as smoking, poor nutrition, lack of physical movement, type-A personality, high alcohol consumption and drug abuse
- strains, including exposures in the occupational, social and private spheres.
Naturally, genetic and dispositional factors also play a role in high blood pressure, diabetes mellitus and lipid metabolism disorders. Many of the risk factors promote the development of arteriosclerosis, which is a significant precondition for the onset of coronary heart disease.
Some risk factors may put the individual at risk for the development of more than one disease; for example, cigarette smoking is associated with coronary artery disease, stroke and lung cancer. At the same time, an individual may have multiple risk factors for a particular disease; these may be additive but, more often, the combinations of risk factors may be multiplicative. Somatic and lifestyle factors have been identified as the main risk factors for coronary heart disease and stroke.
Hypertension
Hypertension (increased blood pressure), a disease in its own right, is one of the major risk factors for coronary heart disease (CHD) and stroke. As defined by the WHO, blood pressure is normal when the diastolic is below 90 mm Hg and the systolic is below 140 mm Hg. In threshold or borderline hypertension, the diastolic ranges from 90 to 94 mm Hg and the systolic from 140 to 159 mm Hg. Individuals with diastolic pressures equal to or greater than 95 mm Hg and systolic pressures equal to or greater than 160 mm Hg are designated as being hypertensive. Studies have shown, however, that such sharp criteria are not entirely correct. Some individuals have a “labile” blood pressure—the pressure fluctuates between normal and hypertensive levels depending on the circumstances of the moment. Further, without regard to the specific categories, there is a linear progression of relative risk as the pressure rises above the normal level.
In the United States, for example, the incidence rate of CHD and stroke among men aged 55 to 61 was 1.61% per year for those whose blood pressure was normal compared to 4.6% per year for those with hypertension (National Heart, Lung and Blood Institute 1981).
Diastolic pressures over 94 mm Hg were found in 2 to 36% of the population aged 35 to 64 years, according to the WHO-MONICA study. In many countries of Central, Northern and Eastern Europe (e.g., Russia, the Czech Republic, Finland, Scotland, Romania, France and parts of Germany, as well as Malta), hypertension was found in over 30% of the population aged 35 to 54, while in countries including Spain, Denmark, Belgium, Luxembourg, Canada and the United States, the corresponding figure was less than 20% (WHO-MONICA 1988). The rates tend to increase with age, and there are racial differences. (In the United States, at least, hypertension is more frequent among African-Americans than in the White population.)
Risks for developing hypertension
The important risk factors for developing hypertension are excess body weight, high salt intake, a series of other nutritional factors, high alcohol consumption, physical inactivity, and psychosocial factors, including stress (Levi 1983). Furthermore, there is a certain genetic component whose relative significance is not yet fully understood (WHO 1985). Frequent familial high blood pressure should be considered a danger and special attention paid to controlling lifestyle factors.
There is evidence that psychosocial and psychophysical factors, in conjunction with the job, can have an influence on developing hypertension, especially for short-term blood pressure increases. Increases have been found in the concentration of certain hormones (adrenalin and noradrenalin) as well as cortisol (Levi 1972), which, alone and in combination with high salt consumption, can lead to increased blood pressure. Work stress also appears to be related to hypertension. A dose-effect relationship with intensity of air traffic was shown (Levi 1972; WHO 1985) in comparing groups of air traffic controllers with different high psychic strain.
Treatment of hypertension
Hypertension can and should be treated, even in the absence of any symptoms. Lifestyle changes such as weight control, reduction of sodium intake and regular physical exercise, coupled when necessary with anti-hypertensive medications, regularly evoke re- ductions in blood pressure, often to normal levels. Unfortunately, many individuals found to be hypertensive are not receiving adequate treatment. According to the WHO-MONICA study (1988), less than 20% of hypertensive women in Russia, Malta, eastern Germany, Scotland, Finland and Italy were receiving adequate treatment during the mid-1980s, while the comparable figure for men in Ireland, Germany, China, Russia, Malta, Finland, Poland, France and Italy was under 15%.
Prevention of hypertension
The essence of preventing hypertension is identifying individuals with blood pressure elevation through periodic screening or medical examination programmes, repeated checks to verify the extent and duration of the elevation, and the institution of an appropriate treatment regimen that will be maintained indefinitely. Those with a family history of hypertension should have their pressures checked more frequently and should be guided to elimination or control of any risk factors they may present. Control of alcohol abuse, physical training and physical fitness, normal weight maintenance and efforts to reduce psychological stress are all important elements of prevention programmes. Improvement in workplace conditions, such as reducing noise and excess heat, are other preventive measures.
The workplace is a uniquely advantageous arena for programmes aimed at the detection, monitoring and control of hypertension in the workforce. Convenience and low or no cost make them attractive to the participants and the positive effects of peer pressure from co-workers tend to enhance their compliance and the success of the programme.
Hyperlipidemia
Many long-term international studies have demonstrated a convincing relationship between abnormalities in lipid metabolism and an increased risk of CHD and stroke. This is particularly true for elevated total cholesterol and LDL (low density lipoproteins) and/or low levels of HDL (high density lipoproteins). Recent research provides further evidence linking the excess risk with different lipoprotein fractions (WHO 1994a).
The frequency of elevated total cholesterol levels >>6.5 mmol/l) was shown to vary considerably in population groups by the worldwide WHO-MONICA studies in the mid-1980s (WHO- MONICA 1988). The rate of hypercholesterolemia for popu- lations of working age (35 to 64 years of age) ranged from 1.3 to 46.5% for men and 1.7 to 48.7% for women. Although the ranges were generally similar, the mean cholesterol levels for the study groups in different countries varied significantly: in Finland, Scot- land, East Germany, the Benelux countries and Malta, a mean of over 6 mmol/l was found, while the means were lower in east Asian countries like China (4.1 mmol/l) and Japan (5.0 mmol/l). In both regions, the means were below 6.5 mmol/l (250 mg/dl), the level designated as the threshold of normal; however, as noted above for blood pressure, there is a progressive increase of risk as the level rises, rather than a sharp demarcation between normal and abnormal. Indeed, some authorities have pegged a total chol- esterol level of 180 mg/dl as the optimal level that should not be exceeded.
It should be noted that gender is a factor, with women averaging lower levels of HDL. This may be one reason why women of working age have a lower mortality rate from CHD.
Except for the relatively few individuals with hereditary hyper- cholesterolemia, cholesterol levels generally reflect the dietary intake of foods rich in cholesterol and saturated fats. Diets based on fruit, plant products and fish, with reduced total fat intake and substitution of poly-unsaturated fats, are generally associated with low cholesterol levels. Although their role is not yet entirely clear, intake of anti-oxidants (vitamin E, carotene, selenium and so on) is also thought to influence cholesterol levels.
Factors associated with higher levels of HDL cholesterol, the “protective” form of lipoprotein, include race (Black), gender (female), normal weight, physical exercise and moderate alcohol intake.
Socio-economic level also appears to play a role, at least in industrialized countries, as in West Germany, where higher cholesterol levels were found in population groups of both men and women with lower education levels (under ten years of schooling) compared to those completing 12 years of education (Heinemann 1993).
Cigarette Smoking
Cigarette smoking is among the most important risk factors for CVD. The risk from cigarette smoking is directly related to the number of cigarettes one smokes, the length of time one has been smoking, the age at which one began to smoke, the amount one inhales and the tar, nicotine and carbon monoxide content of the inspired smoke. Figure 1 illustrates the striking increase in CHD mortality among cigarette smokers compared to non-smokers. This increased risk is demonstrated among both men and women and in all socio-economic classes.
The relative risk of cigarette smoking declines after tobacco use is discontinued. This is progressive; after about ten years of non-smoking, the risk is down almost to the level of those who never smoked.
Recent evidence has demonstrated that those inhaling “second-hand smoke” (i.e., passive inhalation of smoke from cigarettes smoked by others) are also at significant risk (Wells 1994; Glantz and Parmley 1995).
Rates of cigarette smoking vary among countries, as demonstrated by the international WHO-MONICA study (1988). The highest rates for men aged 35 to 64 were found in Russia, Poland, Scotland, Hungary, Italy, Malta, Japan and China. More women smokers were found in Scotland, Denmark, Ireland, the United States, Hungary and Poland (the recent Polish data are limited to large cities).
Social status and occupational level are factors in the level of smoking among workers. Figure 1, for example, demonstrates that the proportions of smokers among men in East Germany increased in the lower social classes. The reverse is found in countries with relatively low numbers of smokers, where there is more smoking among those at higher social levels. In East Germany, smoking is also more frequent among shift-workers when compared with those on a “normal” work schedule.
Figure 1. Relative mortality risk from cardiovascular diseases for smokers (including ex-smokers) and social classes compared to non-smoking, normal weight, skilled workers (male) based on occupational medical care examinations in East Germany, mortality 1985-89, N= 2.7 million person years.
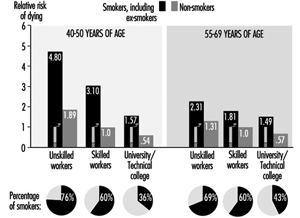
Unbalanced Nutrition, Salt Consumption
In most industrialized countries traditional low-fat nutrition has been replaced by high-calorie, high-fat, low carbohydrate, too sweet or too salty eating habits. This contributes to the development of overweight, high blood pressure, and high cholesterol level as elements of high cardiovascular risk. The heavy consumption of animal fats, with their high proportion of saturated fatty acids, leads to an increase in LDL cholesterol and increased risk. Fats derived from vegetables are much lower in these substances (WHO 1994a). Eating habits are also strongly associated with both socio-economic level and occupation.
Overweight
Overweight (excess fat or obesity rather than increased muscle mass) is a cardiovascular risk factor of lesser direct significance. There is evidence that the male pattern of excess fat distribution (abdominal obesity) is associated with a greater risk of cardiovascular and metabolic problems than the female (pelvic) type of fat distribution.
Overweight is associated with hypertension, hypercholesterolemia and diabetes mellitus, and, to a much greater extent in women than men, tends to increase with age (Heuchert and Enderlein 1994) (Figure 2). It is also a risk factor for musculoskeletal problems and osteoarthritis, and makes physical exercise more difficult. The frequency of significant overweight varies considerably among countries. Random population surveys conducted by the WHO-MONICA project found it in more than 20% of females aged 35 to 64 in the Czech Republic, East Germany, Finland, France, Hungary, Poland, Russia, Spain and Yugoslavia, and in both sexes in Lithuania, Malta and Romania. In China, Japan, New Zealand and Sweden, fewer than 10% of both men and women in this age group were significantly overweight.
Common causes of overweight include familial factors (these may in part be genetic but more often reflect common dietary habits), overeating, high-fat and high-carbohydrate diets and lack of physical exercise. Overweight tends to be more common among the lower socio-economic strata, particularly among women, where, among other factors, financial constraints limit the availability of a more balanced diet. Population studies in Germany demonstrated that the proportion of significant overweight among those with lower education levels is 3 to 5 times greater than that among people with more education, and that some occupations, notably food preparation, agriculture and to some extent shift work, have a high percentage of overweight people (Figure 3) (Heinemann 1993).
Figure 2. Prevalence of hypertension by age, sex and six levels of relative body weight according tot he body-mass index (BMI) in occupational medical care examinations in East Germany (normal BMI values are underlined).
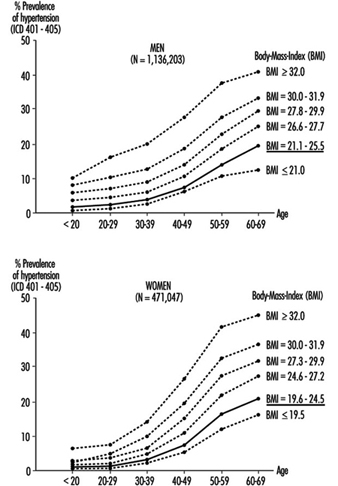
Figure 3. Relative risk from overweight by length of education(years of schooling) in Germay (population 25-64 years).
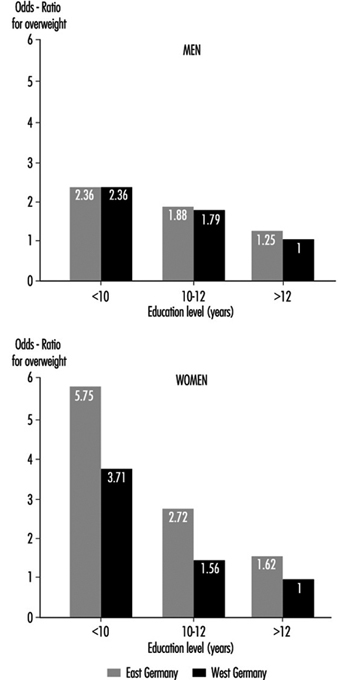
Physical Inactivity
The close association of hypertension, overweight and diabetes mellitus with lack of exercise at work and/or off the job has made physical inactivity a significant risk factor for CHD and stroke (Briazgounov 1988; WHO 1994a). A number of studies have demonstrated that, holding all other risk factors constant, there was a lower mortality rate among persons engaging regularly in high-intensity exercises than among those with a sedentary lifestyle.
The amount of exercise is readily measured by noting its duration and either the amount of physical work accomplished or the extent of the exercise-induced increase in heart rate and the time required for that rate to return to its resting level. The latter is also useful as an indicator of the level of cardiovascular fitness: with regular physical training, there will be less of an increase in heart rate and a more rapid return to the resting rate for a given intensity of exercise.
Workplace physical fitness programmes have been shown to be effective in enhancing cardiovascular fitness. Participants in these tend also to give up cigarette smoking and to pay greater attention to proper diets, thus significantly reducing their risk of CHD and stroke.
Alcohol
High alcohol consumption, especially the drinking of high-proof spirits, has been associated with a greater risk of hypertension, stroke and myocardiopathy, while moderate alcohol use, particularly of wine, has been found to reduce the risk of CHD (WHO 1994a). This has been associated with the lower CHD mortality among the upper social strata in industrialized countries, who generally prefer wine to “hard” liquors. It should also be noted that while their alcohol intake may be similar to that of wine drinkers, beer drinkers tend to accumulate excess weight, which, as noted above, may increase their risk.
Socio-economic Factors
A strong correlation between socio-economic status and the risk of CVD has been demonstrated by analyses of the death register mortality studies in Britain, Scandinavia, Western Europe, the United States and Japan. For example, in eastern Germany, the cardiovascular death rate is considerably lower for the upper social classes than for the lower classes (see Figure 1) (Marmot and Theorell 1991). In England and Wales, where general mortality rates are declining, the relative gap between the upper and lower classes is widening.
Socio-economic status is typically defined by such indicators as occupation, occupational qualifications and position, level of education and, in some instances, income level. These are readily translated into standard of living, nutritional patterns, free-time activities, family size and access to medical care. As noted above, behavioural risk factors (such as smoking and diet) and the somatic risk factors (such as overweight, hypertension and hyperlipidemia) vary considerably among social classes and occupational groups (Mielck 1994; Helmert, Shea and Maschewsky Schneider 1995).
Occupational Psychosocial Factors and Stress
Occupational stress
Psychosocial factors at the workplace primarily refer to the combined effect of working environment, work content, work demands and technological-organizational conditions, and also to personal factors like capability, psychological sensitivity, and finally also to health indicators (Karasek and Theorell 1990; Siegrist 1995).
The role of acute stress on people who already suffer from cardiovascular disease is uncontested. Stress leads to episodes of angina pectoris, rhythm disorders and heart failure; it can also precipitate a stroke and/or a heart attack. In this context stress is generally understood to mean acute physical stress. But evidence has been mounting that acute psychosocial stress can also have these effects. Studies from the 1950s showed that people who work two jobs at a time, or who work overtime for long periods, have a relatively higher risk of heart attack, even at a young age. Other studies showed that in the same job, the person with the greater work and time pressure and frequent problems on the job is at significantly greater risk (Mielck 1994).
In the last 15 years, job stress research suggests a causal relationship between work stress and the incidence of cardiovascular disease. This is true for cardiovascular mortality as well as frequency of coronary disease and hypertension (Schnall, Landsbergis and Baker 1994). Karasek’s job strain model defined two factors that could lead to an increased incidence of cardiovascular disease:
- extent of job demands
- extent of decision-making latitude.
Later Johnson added as a third factor the extent of social support (Kristensen 1995) which is discussed more fully elsewhere in this Encyclopaedia. The chapter Psychosocial and Organizational Factors includes discussions on individual factors, such as Type A personality, as well as social support and other mechan- isms for overcoming the effects of stress.
The effects of factors, whether individual or situational, that lead to increased risk of cardiovascular disease can be reduced by “coping mechanisms”, that is, by recognizing the problem and overcoming it by attempting to make the best of the situation.
Until now, measures aimed at the individual have predominated in the prevention of the negative health effects of work stress. Increasingly, improvements in organizing the work and expanding employee decision-making latitude have been used (e.g., action research and collective bargaining; in Germany, occupational quality and health circles) to achieve an improvement in productivity as well as to humanize the work by decreasing the stress load (Landsbergis et al. 1993).
Night and Shift Work
Numerous publications in the international literature cover the health risks posed by night and shift work. It is generally accepted that shift work is one risk factor which, together with other relev- ant (including indirect) work-related demands and expectation factors, leads to adverse effects.
In the last decade research on shift work has increasingly dealt with the long-term effects of night and shift work on the frequency of cardiovascular disease, especially ischaemic heart disease and myocardial infarction, as well as cardiovascular risk factors. The results of epidemiological studies, especially from Scandinavia, permit a higher risk of ischemic heart disease and myocardial infarction to be presumed for shift workers (Alfredsson, Karasek and Theorell 1982; Alfredsson, Spetz and Theorell 1985; Knutsson et al. 1986; Tüchsen 1993). In Denmark it was even estimated that 7% of cardiovascular disease in men as well as women can be traced to shift work (Olsen and Kristensen 1991).
The hypothesis that night and shift workers have a higher risk (estimated relative risk approximately 1.4) for cardiovascular disease is supported by other studies that consider cardiovascular risk factors like hypertension or fatty acid levels for shift workers as compared to day workers. Various studies have shown that night and shift work may induce increased blood pressure and hypertension as well as increased triglyceride and/or serum cholesterol (as well as normal range fluctuations for HDL-cholesterol in increased total cholesterol). These changes, together with other risk factors (like heavy cigarette smoking and overweight among shift workers), can cause increased morbidity and mortality due to atherosclerotic disease (DeBacker et al. 1984; DeBacker et al. 1987; Härenstam et al. 1987; Knutsson 1989; Lavie et al. 1989; Lennernäs, Åkerstedt and Hambraeus 1994; Orth-Gomer 1983; Romon et al. 1992).
In all, the question of possible causal links between shift work and atherosclerosis cannot be definitively answered at present, as the pathomechanism is not sufficiently clear. Possible mechanisms discussed in the literature include changes in nutrition and smoking habits, poor sleep quality, increases in lipid level, chronic stress from social and psychological demands and disrupted circadian rhythms. Knutsson (1989) has proposed an interesting pathogenesis for the long-term effects of shift work on chronic morbidity.
The effects of various associated attributes on risk estimation have hardly been studied, since in the occupational field other stress-inducing working conditions (noise, chemical hazardous materials, psychosocial stress, monotony and so on) are connected with shift work. From the observation that unhealthy nutritional and smoking habits are often connected with shift work, it is often concluded that an increased risk of cardiovascular disease among shift workers is more the indirect result of unhealthy behaviour (smoking, poor nutrition and so on) than directly the result of night or shift work (Rutenfranz, Knauth and Angersbach 1981). Furthermore, the obvious hypothesis of whether shift work promotes this conduct or whether the difference comes primarily from the choice of workplace and occupation must be tested. But regardless of the unanswered questions, special attention must be paid in cardiovascular prevention programmes to night and shift workers as a risk group.
Summary
In summary, risk factors represent a broad variety of genetic, somatic, physiological, behavioural and psychosocial characteristics which can be assessed individually for individuals and for groups of individuals. In the aggregate, they reflect the probability that CVD, or more precisely in the context of this article, CHD or stroke will develop. In addition to elucidating the causes and pathogenesis of multifactorial diseases, their chief importance is that they delineate individuals who should be targets for risk factor elimination or control, an exercise admirably suited to the workplace, while repeated risk assessments over time demonstrate the success of that preventive effort.
Rehabilitation and Prevention Programmes
Most individuals with recognized CVD are able to work effectively and productively in most of the jobs found in the modern workplace. Just a few decades ago, individuals surviving an acute myocardial infarction were cosseted and pampered for weeks and months with close supervision and enforced inactivity. Laboratory confirmation of the diagnosis was enough to justify labelling the individual as “permanently and totally disabled”. New diagnostic technology that provides more accurate evaluation of cardiac status and the favourable experiences of those who could not or would not accept such a label, soon demonstrated that an early return to work and an optimal level of activity was not only possible but desirable (Edwards, McCallum and Taylor 1988; Theorell et al. 1991; Theorell 1993). Today, patients commence supervised physical activity as soon as the acute effects of the infarction subside, are often out of the hospital in a few days instead of the mandatory 6 to 8 weeks of yore, and are often back on the job within a few weeks. When desirable and feasible, surgical procedures such as angioplasty, by-pass operations and even cardiac transplantation can improve the coronary blood flow, while a regimen featuring diet, exercise and control of the risk factors for CHD can minimize (or even reverse) the progression of coronary atherosclerosis.
Once the acute, often life-threatening phases of the CVD have been overcome, passive movement followed by active exercise should be initiated early during the stay in the hospital or clinic. With heart attacks, this phase is completed when the individual can climb stairs without great difficulty. At the same time, the individual is schooled in a risk-prevention regimen that includes proper diet, cardiovascular conditioning exercises, adequate rest and relaxation, and stress management. During these phases of rehabilitation, support from family members, friends and co-workers can be particularly helpful (Brusis and Weber-Falkensammer 1986). The programme can be carried out in rehabilitation facilities or in ambulatory “heart groups” under the supervision of a trained physician (Halhubar and Traencker 1986). The focus on controlling lifestyle and behavioural risk factors and controlling stress has been shown to result in a measurable reduction in the risk of re-infarction and other cardiovascular problems.
Throughout the programme the attending physician should maintain contact with the employer (and particularly with the company doctor, if there is one) to discuss the prospects for recovery and the probable duration of the period of disability, and to explore the feasibility of any special arrangements that may be needed to permit an early return to the job. The worker’s knowledge that the job is waiting and that he or she is expected to be able to return to it is a potent motivating factor for the enhancement of recovery. Experience has amply demonstrated that the success of the rehabilitation effort diminishes as the absence from work lengthens.
In instances where desirable adjustments in the job and/or the workplace are not possible or feasible, retraining and appropriate job placement can obviate unnecessary invalidism. Specially protected workshops are often helpful in reintegrating into the workplace people who have been absent from the job for long periods while receiving treatment for the serious effects of stroke, congestive heart failure or disabling angina pectoris.
Following the return to work, continued surveillance by both the attending physician and the occupational physician is eminently desirable. Periodic medical evaluations, at intervals that are frequent initially but lengthen as recovery is assured, are helpful in assessing the worker’s cardiovascular status, adjusting medications and other elements in the maintenance regimen and monitoring the adherence to the lifestyle and behavioural recommendations. Satisfactory findings in these examinations may allow the gradual easing of any work limitations or restrictions until the worker is fully integrated into the workplace.
Workplace Health Promotion and Prevention Programmes
The prevention of occupational diseases and injuries is a prime responsibility of the organization’s occupational health and safety programme. This includes primary prevention (i.e., the identifica- tion and elimination or control of potential hazards and strains by changing the work environment or the job). It is supplemented by secondary prevention measures which protect the workers from the effects of existing hazards and strains that cannot be elim- inated (i.e., personal protective equipment and periodic medical surveillance examinations). Workplace health promotion and pre- vention (HPP) programmes go beyond these goals. They place their emphasis on health-conscious behaviour as it relates to life- style, behavioural risk factors, eliminating or coping with stress and so on. They are of great significance, particularly in pre- venting CVD. The goals of HPP, as formulated by the WHO Committee on Environmental and Health Monitoring in Occupational Health, extend beyond the mere absence of disease and injury to include well-being and functional capacity (WHO 1973).
The design and operation of HPP programmes are discussed in more detail elsewhere in the chapter. In most countries, they have a particular focus on the prevention of CVDs. For example, in Germany, the “Have a heart for your heart” programme supplements the heart health circles organized by the health insurance companies (Murza and Laaser 1990, 1992), while the “Take Heart” movement in Britain and Australia has similar goals (Glasgow et al. 1995).
That such programmes are effective was verified in the 1980s by the WHO Collaborative Trial in Prevention of Heart Disease, which was carried out in 40 pairs of factories in four European countries and involved approximately 61,000 men aged 40 to 59. The preventive measures largely comprised health education activities, carried out primarily by the organization’s employee health service, focused on cholesterol-lowering diets, giving up cigarette smoking, weight control, increased physical activity and controlling hypertension. A randomized screening of 10% of the eligible workers in the factories designated as controls demonstrated that during the 4 to 7 years of the study, overall risk of CVDs could be reduced by 11.1% (19.4% among those initially at high risk). In the study factories, mortality from CHDs fell by 7.4%, while overall mortality fell by 2.7%. The best results were achieved in Belgium, where the intervention was carried out continuously during the entire study period, while the poorest results were seen in Britain, where the prevention activities were sharply curtailed prior to the last follow-up examination. This disparity emphasizes the relationship of success to the duration of the health education effort; it takes time to inculcate the desired lifestyle changes. The intensity of the educational effort was also a factor: in Italy, where six full-time health educators were involved, a 28% reduction in overall risk-factor profile was achieved, whereas in Britain, where only two full-time educators served three times the number of workers, a risk factor reduction of only 4% was achieved.
While the time required to detect reductions in CHD mortality and morbidity is a formidable limiting factor in epidemiological studies aimed at evaluating the results of company health programmes (Mannebach 1989), reductions in risk factors have been demonstrated (Janssen 1991; Gomel et al. 1993; Glasgow et al. 1995). Temporary decreases in the number of lost workdays and a decline in hospitalization rates have been reported (Harris 1994). There seems to be general agreement that HPP activities in the community and particularly in the workplace have significantly contributed to the reduction in cardiovascular mortality in the United States and other western industrialized countries.
Conclusion
CVDs loom large in the workplace, not so much because the cardiovascular system is particularly vulnerable to environmental and job hazards, but because they are so common in the popu- lation of working age. The workplace offers a singularly advant- ageous arena for the detection of unrecognized, asymptomatic CVDs, for the circumvention of workplace factors that might accelerate or aggravate them and for the identification of factors that increase the risk of CVDs and the mounting of programmes to eliminate or control them. When CVDs do occur, prompt attention to control of job-related circumstances that may prolong or increase their severity can minimize the extent and duration of disability, while early, professionally supervised rehabilitation efforts will facilitate the restoration of working capacity and reduce the risk of recurrences.
Physical, Chemcial and Biological Hazards
The intact cardiovascular system is remarkably resistant to the harmful effects of physical, chemical and biological hazards encountered on the job or in the workplace. With a very few exceptions, such hazards are rarely a direct cause of CVDs. On the other hand, once the integrity of the cardiovascular system is compromised—and this may be entirely silent and unrecognized—exposure to these hazards may contribute to the ongoing development of a disease process or precipitate symptoms reflecting functional impairment. This dictates early identification of workers with incipient CVD and modification of their jobs and/or the work environment to reduce the risk of harmful effects. The following segments will include brief discussions of some of the more commonly encountered occupational hazards that may affect the cardiovascular system. Each of the hazards presented below is discussed more fully elsewhere in the Encyclopaedia.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."