- You are here:
-
Home

-
Contents
-
Part V. Psychosocial and Organizational Factors
-
Psychosocial and Organizational Factors
- Stress Reactions

Stress Reactions
Selected Acute Physiological Outcomes
Andrew Steptoe and Tessa M. Pollard
The acute physiological adjustments recorded during the performance of problem-solving or psychomotor tasks in the laboratory include: raised heart rate and blood pressure; alterations in cardiac output and peripheral vascular resistance; increased muscle tension and electrodermal (sweat gland) activity; disturbances in breathing pattern; and modifications in gastrointestinal activity and immune function. The best studied neurohormonal responses are those of the catecholamines (adrenaline and noradrenaline) and cortisol. Noradrenaline is the primary transmitter released by the nerves of the sympathetic branch of the autonomic nervous system. Adrenaline is released from the adrenal medulla following stimulation of the sympathetic nervous system, while activation of the pituitary gland by higher centres in the brain results in the release of cortisol from the adrenal cortex. These hormones support autonomic activation during stress and are responsible for other acute changes, such as stimulation of the processes that govern blood clotting, and the release of stored energy supplies from adipose tissue. It is likely that these kinds of response will also be seen during job stress, but studies in which work conditions are simulated, or in which people are tested in their normal jobs, are required to demonstrate such effects.
A variety of methods is available to monitor these responses. Conventional psychophysiological techniques are used to assess autonomic responses to demanding tasks (Cacioppo and Tassinary 1990). Levels of stress hormones can be measured in the blood or urine, or in the case of cortisol, in the saliva. The sympathetic activity associated with challenge has also been documented by measures of noradrenaline spillover from nerve terminals, and by direct recording of sympathetic nervous activity with miniature electrodes. The parasympathetic or vagal branch of the autonomic nervous system typically responds to task performance with reduced activity, and this can, under certain circumstances, be indexed through recording heart rate variability or sinus arrhythmia. In recent years, power spectrum analysis of heart rate and blood pressure signals has revealed wave bands that are characteristically associated with sympathetic and parasympathetic activity. Measures of the power in these wavebands can be used to index autonomic balance, and have shown a shift towards the sympathetic branch at the expense of the parasympathetic branch during task performance.
Few laboratory assessments of acute physiological responses have simulated work conditions directly. However, dimensions of task demand and performance that are relevant to work have been investigated. For example, as the demands of externally paced work increase (through faster pace or more complex problem solving), there is a rise in adrenaline level, heart rate and blood pressure, a reduction in heart rate variability and an increase in muscle tension. In comparison with self-paced tasks performed at the same rate, external pacing results in greater blood pressure and heart rate increases (Steptoe et al. 1993). In general, personal control over potentially stressful stimuli reduces autonomic and neuroendocrine activation in comparison with uncontrollable situations, although the effort of maintaining control over the situation itself has its own physiological costs.
Frankenhaeuser (1991) has suggested that adrenaline levels are raised when a person is mentally aroused or performing a demanding task, and that cortisol levels are raised when an individual is distressed or unhappy. Applying these ideas to job stress, Frankenhaeuser has proposed that job demand is likely to lead to increased effort and thus to raise levels of adrenaline, while lack of job control is one of the main causes of distress at work and is therefore likely to stimulate raised cortisol levels. Studies comparing levels of these hormones in people doing their normal work with levels in the same people at leisure have shown that adrenaline is normally raised when people are at work. Effects for noradrenaline are inconsistent and may depend on the amount of physical activity that people carry out during work and leisure time. It has also been shown that adrenaline levels at work correlate positively with levels of job demand. In contrast, cortisol levels have not been shown typically to be raised in people at work, and it is yet to be demonstrated that cortisol levels vary according to the degree of job control. In the “Air Traffic Controller Health Change Study”, only a small proportion of workers produced consistent increases in cortisol as the objective workload became greater (Rose and Fogg 1993).
Thus only adrenaline among the stress hormones has been shown conclusively to rise in people at work, and to do so according to the level of demand they experience. There is evidence that levels of prolactin increase in response to stress while levels of testosterone decrease. However, studies of these hormones in people at work are very limited. Acute changes in the concentration of cholesterol in the blood have also been observed with increased workload, but the results are not consistent (Niaura, Stoney and Herbst 1992).
As far as cardiovascular variables are concerned, it has repeatedly been found that blood pressure is higher in men and women during work than either after work or during equivalent times of day spent at leisure. These effects have been observed both with self-monitored blood pressure and with automated portable (or ambulatory) monitoring instruments. Blood pressure is especially high during periods of increased work demand (Rose and Fogg 1993). It has also been found that blood pressure rises with emotional demands, for example, in studies of paramedics attending the scenes of accidents. However, it is often difficult to determine whether blood pressure fluctuations at work are due to psychological demands or to associated physical activity and changes in posture. The raised blood pressure recorded at work is especially pronounced among people reporting high job strain according to the Demand-Control model (Schnall et al. 1990).
Heart rate has not been shown to be consistently raised during work. Acute elevations of heart rate may nevertheless be elicited by disruption of work, for example with breakdown of equipment. Emergency workers such as fire-fighters exhibit extremely fast heart rates in response to alarm signals at work. On the other hand, high levels of social support at work are associated with reduced heart rates. Abnormalities of cardiac rhythm may also be elicited by stressful working conditions, but the pathological significance of such responses has not been established.
Gastrointestinal problems are commonly reported in studies of job stress (see “Gastrointestinal problems” below). Unfortunately, it is difficult to assess the physiological systems underlying gastrointestinal symptoms in the work setting. Acute mental stress has variable effects on gastric acid secretion, stimulating large increases in some individuals and reduced output in others. Shift workers have a particularly high prevalence of gastrointestinal problems, and it has been suggested that these may arise when diurnal rhythms in the central nervous system’s control of gastric acid secretion are disrupted. Anomalies of small bowel motility have been recorded using radiotelemetry in patients diagnosed with irritable bowel syndrome while they go about their everyday lives. Health complaints, including gastrointestinal symptoms, have been shown to co-vary with perceived workload, but it is not clear whether this reflects objective changes in physiological function or patterns of symptom perception and reporting.
Behavioural Outcomes
Researchers may disagree on the meaning of the term stress. However, there is a basic agreement that perceived work-related stress may be implicated in behavioural outcomes such as absenteeism, substance abuse, sleep disturbances, smoking and caffeine use (Kahn and Byosiere 1992). Recent evidence supporting these relationships is reviewed in this chapter. Emphasis is placed upon the aetiological role of work-related stress in each of these outcomes. There are qualitative differences, along several dimensions, among these outcomes. To illustrate, in contrast to the other behavioural outcomes, which are all considered problematic to the health of those engaging in them excessively, absenteeism, while detrimental to the organization, is not necessarily harmful to those employees who are absent from work. There are, however, common problems in the research on these outcomes, as discussed in this section.
The varying definitions of work-related stress have already been mentioned above. By way of illustration, consider the different conceptualizations of stress on the one hand as events and on the other as chronic demands at the workplace. These two approaches to stress measurement have seldom been combined in a single study designed to predict the sorts of behavioural outcome considered here. The same generalization is relevant to the combined use, in the same study, of family-related and work-related stress to predict any of these outcomes. Most of the studies referred to in this chapter were based on a cross-sectional design and employees’ self-reports on the behavioural outcome in question. In most of the research that concerned behavioural outcomes of work-related stress, the joint moderating or mediating roles of predisposing personality variables, like the Type A behaviour pattern or hardiness, and situational variables like social support and control, have hardly been investigated. Seldom have antecedent variables, like objectively measured job stress, been included in the research designs of the studies reviewed here. Finally, the research covered in this article employed divergent methodologies. Because of these limitations, a frequently encountered conclusion is that the evidence for work-related stress as a precursor of a behavioural outcome is inconclusive.
Beehr (1995) considered the question of why so few studies have systematically examined the associations between work- related stress and substance abuse. He argued that such neglect may be due in part to the failure of researchers to find these associations. To this failure, one should add the well-known bias of periodicals against publishing research that reports null results. To illustrate the inconclusiveness of the evidence linking stress and substance abuse, consider two large-scale national samples of employees in the United States. The first, by French, Caplan and Van Harrison (1982), failed to find significant correlations between types of work-related stress and either smoking, drug use or on-the-job caffeine ingestion. The second, an earlier research study by Mangione and Quinn (1975), did report such associations.
The study of the behavioural outcomes of stress is further complicated because they frequently appear in pairs or triads. Different combinations of outcomes are the rule rather than the exception. The very close association of stress, smoking and caffeine is alluded to below. Yet another example concerns the comorbidity of post-traumatic stress disorder (PTSD), alcoholism and drug abuse (Kofoed, Friedman and Peck 1993). This is a basic characteristic of several behavioural outcomes considered in this article. It has led to the construction of “dual diagnosis” and “triple diagnosis” schemes and to the development of comprehensive, multifaceted treatment approaches. An example of such an approach is that in which PTSD and substance abuse are treated simultaneously (Kofoed, Friedman and Peck 1993).
The pattern represented by the appearance of several outcomes in a single individual may vary, depending on background characteristics and genetic and environmental factors. The literature on stress outcomes is only beginning to address the complex questions involved in identifying the specific pathophysiological and neurobiological disease models leading to different combinations of outcome entities.
Smoking Behaviour
A large body of epidemiological, clinical and pathological studies relates cigarette smoking to the development of cardiovascular heart disease and other chronic diseases. Consequently, there is a growing interest in the pathway leading from stress, including stress at work, to smoking behaviour. Stress, and the emotional responses associated with it, anxiety and irritability, are known to be attenuated by smoking. However, these effects have been shown to be short-lived (Parrott 1995). Impairments of mood and affective states tend to occur in a repetitive cycle between each cigarette smoked. This cycle provides a clear pathway leading to the addictive use of cigarettes (Parrott 1995). Smokers, therefore, obtain only a short-lived relief from adverse states of anxiety and irritability that follow the experience of stress.
The aetiology of smoking is multifactorial (like most other behavioural outcomes considered here). To illustrate, consider a recent review of smoking among nurses. Nurses, the largest professional group in health care, smoke excessively compared with the adult population (Adriaanse et al. 1991). According to their study, this is true for both male and female nurses, and is explained by work stress, lack of social support and unmet expectations that characterize nurses’ professional socialization. Nurses’ smoking is considered a special public health problem since nurses often act as role models to patients and their families.
Smokers who express high motivation to smoke have reported, in several studies, above-average stress that they had experienced before smoking, rather than below-average stress after smoking (Parrott 1995). Consequently, stress management and anxiety reduction programmes in the workplace do have the potential of influencing motivation for smoking. However, workplace-based smoking-cessation programmes do bring to the fore the conflict between health and performance. Among aviators, as an example, smoking is a health hazard in the cockpit. However, pilots who are required to abstain from smoking during and before flights may suffer cockpit performance decrements (Sommese and Patterson 1995).
Drug and Alcohol Abuse
A recurrent problem is that often researchers do not distinguish between drinking and problem-drinking behaviour (Sadava 1987). Problem-drinking is associated with adverse health or performance consequences. Its aetiology has been shown to be associated with several factors. Among them, the literature refers to prior incidents of depression, lack of supportive family environment, impulsiveness, being female, other concurrent substance abuse and stress (Sadava 1987). The distinction between the simple act of drinking alcohol and problem drinking is important because of the current controversy on the reported beneficial effects of alcohol on low density lipoprotein (LDL) cholesterol and on the incidence of heart disease. Several studies have shown a J-shaped or U-shaped relationship between alcohol ingestion and the incidence of cardiovascular heart disease (Pohorecky 1991).
The hypothesis that people ingest alcohol even in an incipiently abusive pattern to reduce stress and anxiety is no longer accepted as adequate. Contemporary approaches to alcohol abuse view it as determined by processes set forth in a multifactorial model or models (Gorman 1994). Among risk factors for alcohol abuse, recent reviews refer to the following factors: sociocultural (i.e., whether alcohol is readily available and its use tolerated, condoned or even promoted), socio-economic (i.e., the price of alcohol), environmental (alcohol advertising and licensing laws affect the consumers’ motivation to drink), interpersonal influences (such as family drinking habits), and employment-related factors, including stress at work (Gorman 1994). It follows that stress is but one of several factors in a multidimensional model that explains alcohol abuse.
The practical consequence of the multifactorial model view of alcoholism is the decrease in the emphasis on the role of stress in the diagnosis, prevention and treatment of substance abuse in the workplace. As noted by a recent review of this literature (Peyser 1992), in specific job situations, such as those illustrated below, attention to work-related stress is important in formulating preventive policies directed at substance abuse.
Despite considerable research on stress and alcohol, the mechanisms that link them are not entirely understood. The most widely accepted hypothesis is that alcohol disrupts the subject’s initial appraisal of stressful information by constraining the spread of activation of associated information previously stored in long-term memory (Petraitis, Flay and Miller 1995).
Work organizations contribute to and may induce drinking behaviour, including problem drinking, by three basic processes documented in the research literature. First, drinking, abusive or not, may be affected by the development of organizational norms with respect to drinking on the job, including the local “official” definition of problem drinking and the mechanisms for its control established by management. Secondly, some stressful working conditions, like sustained overload or machine-paced jobs or the lack of control may produce alcohol abuse as a coping strategy alleviating the stress. Thirdly, work organizations may explicitly or implicitly encourage the development of occupationally based drinking subcultures, such as those that often emerge among professional drivers of heavy vehicles (James and Ames 1993).
In general, stress plays a different role in provoking drinking behaviour in different occupations, age groups, ethnic categories and other social groupings. Thus stress probably plays a predisposing role with respect to alcohol consumption among adolescents, but much less so among women, the elderly and college-age social drinkers (Pohorecky 1991).
The social stress model of substance abuse (Lindenberg, Reiskin and Gendrop 1994) suggests that the likelihood of employees’ drug abuse is influenced by the level of environmental stress, social support relevant to the experienced stress, and individual resources, particularly social competence. There are indications that drug abuse among certain minority groups (like Native American youth living on reservations: see Oetting, Edwards and Beauvais 1988) is influenced by the prevalence of acculturation stress among them. However, the same social groups are also exposed to adverse social conditions like poverty, prejudices and impoverished opportunities for economic, social and educational opportunities.
Caffeine Ingestion
Caffeine is the most widely consumed pharmacologically active substance in the world. The evidence bearing upon its possible implications for human health, that is whether it has chronic physiological effects on habitual consumers, is as yet inconclusive (Benowitz 1990). It has long been suspected that repeated exposure to caffeine may produce tolerance to its physiological effects (James 1994). The consumption of caffeine is known to improve physical performance and endurance during prolonged activity at submaximal intensity (Nehlig and Debry 1994). Caffeine’s physiological effects are linked to the antagonism of adenosine receptors and to the increased production of plasma catecholamines (Nehlig and Debry 1994).
The study of the relationship of work-related stress on caffeine ingestion is complicated because of the significant inter-dependance of coffee consumption and smoking (Conway et al. 1981). A meta-analysis of six epidemiological studies (Swanson, Lee and Hopp 1994) has shown that about 86% of smokers consumed coffee while only 77% of the non-smokers did so. Three major mechanisms have been suggested to account for this close association: (1) a conditioning effect; (2) reciprocal interaction, that is, caffeine intake increases arousal while nicotine intake decreases it and (3) the joint effect of a third variable on both. Stress, and particularly work-related stress, is a possible third variable influencing both caffeine and nicotine intake (Swanson, Lee and Hopp 1994).
Sleep Disturbances
The modern era of sleep research began in the 1950s, with the discovery that sleep is a highly active state rather than a passive condition of nonresponsiveness. The most prevalent type of sleep disturbance, insomnia, may occur in a transient short-term form or in a chronic form. Stress is probably the most frequent cause of transient insomnia (Gillin and Byerley 1990). Chronic insomnia usually results from an underlying medical or psychiatric disorder. Between one-third and two-thirds of patients with chronic insomnia have a recognizable psychiatric illness (Gillin and Byerley 1990).
One of the mechanisms suggested is that the effect of stress on sleep disturbances is mediated via certain changes in the cerebral system at different levels, and changes in the biochemical body functions that disturb the 24-hour rhythms (Gillin and Byerley 1990). There is some evidence that the above linkages are moderated by personality characteristics, such as the Type A behaviour pattern (Koulack and Nesca 1992). Stress and sleep disturbances may reciprocally influence each other: stress may promote transient insomnia, which in turn causes stress and increases the risk of episodes of depression and anxiety (Partinen 1994).
Chronic stress associated with monotonous, machine-paced jobs coupled with the need for vigilance—jobs frequently found in continuous-processing manufacturing industries—may lead to sleep disturbances, subsequently causing decrements in performance (Krueger 1989). There is some evidence that there are synergetic effects among work-related stress, circadian rhythms and reduced performance (Krueger 1989). The adverse effects of sleep loss, interacting with overload and a high level of arousal, on certain important aspects of job performance have been documented in several studies of sleep deprivation among hospital doctors at the junior level (Spurgeon and Harrington 1989).
The study by Mattiason et al. (1990) provides intriguing evidence linking chronic job stress, sleep disturbances and increases in plasma cholesterol. In this study, 715 male shipyard employees exposed to the stress of unemployment were systematically compared with 261 controls before and after the economic instability stress was made apparent. It was found that among the shipyard employees exposed to job insecurity, but not among the controls, sleep disturbances were positively correlated with increases in total cholesterol. This is a naturalistic field study in which the period of uncertainty preceding actual layoffs was allowed to elapse for about a year after some employees received notices concerning the impending layoffs. Thus the stress studied was real, severe, and could be considered chronic.
Absenteeism
Absence behaviour may be viewed as an employee coping behaviour that reflects the interaction of perceived job demands and control, on the one hand, and self-assessed health and family conditions on the other. Absenteeism has several major dimensions, including duration, spells and reasons for being absent. It was shown in a European sample that about 60% of the hours lost to absenteeism were due to illness (Ilgen 1990). To the extent that work-related stress was implicated in these illnesses, then there should be some relationship between stress on the job and that part of absenteeism classified as sick days. The literature on absenteeism covers primarily blue-collar employees, and few studies have included stress in a systematic way. (McKee, Markham and Scott 1992). Jackson and Schuler’s meta-analysis (1985) of the consequences of role stress reported an average correlation of 0.09 between role ambiguity and absence and -0.01 between role conflict and absence. As several meta-analytic studies of the literature on absenteeism show, stress is but one of many variables accounting for these phenomena, so we should not expect work-related stress and absenteeism to be strongly correlated (Beehr 1995).
The literature on absenteeism suggests that the relationship between work-related stress and absenteeism may be mediated by employee-specific characteristics. For example, the literature refers to the propensity to use avoidance coping in response to stress at work, and to being emotionally exhausted or physically fatigued (Saxton, Phillips and Blakeney 1991). To illustrate, Kristensen’s (1991) study of several thousand Danish slaughterhouse employees over a one-year period has shown that those who reported high job stress had significantly higher absence rates and that perceived health was closely associated with absenteeism due to illness.
Several studies of the relationships between stress and absenteeism provide evidence that supports the conclusion that they may be occupationally determined (Baba and Harris 1989). To illustrate, work-related stress among managers tends to be associated with the incidence of absenteeism but not with days lost attributed to illness, while this is not so with shop-floor employees (Cooper and Bramwell 1992). Occupational specificity of the stresses predisposing employees to be absent has been regarded as a major explanation of the meagre amount of absence variance explained by work-related stress across many studies (Baba and Harris 1989). Several studies have found that among blue-collar employees who work on jobs considered stressful—that is those that possess a combination of the characteristics of assembly-line type of jobs (namely, a very short cycle of operations and a piece-rate wage system)—job stress is a strong predictor of unexcused absence. (For a recent review of these studies, see McKee, Markham and Scott 1992; note that Baba and Harris 1989 do not support their conclusion that job stress is a strong predictor of unexcused absence).
The literature on stress and absenteeism provides a convincing example of a limitation noted in the introduction. The reference is to the failure of most research on stress-behavioural outcome relations to cover systematically, in the design of this research, both work and non-work stresses. It was noted that in research on absenteeism non-work stress contributed more than work-related stress to the prediction of absence, lending support to the view that absence may be non-work behaviour more than work-related behaviour (Baba and Harris 1989).
Well-being Outcomes
Jobs can have a substantial impact on the affective well-being of job holders. In turn, the quality of workers’ well-being on the job influences their behaviour, decision making and interactions with colleagues, and spills over into family and social life as well.
Research in many countries has pointed to the need to define the concept in terms of two separate dimensions that may be viewed as independent of each other (Watson, Clark and Tellegen 1988; Warr 1994). These dimensions may be referred to as “pleasure” and “arousal”. As illustrated in figure 1, a particular degree of pleasure or displeasure may be accompanied by high or low levels of mental arousal, and mental arousal may be either pleasurable or unpleasurable. This is indicated in terms of the three axes of well-being which are suggested for measurement: displeasure-to-pleasure, anxiety-to-comfort, and depression-to-enthusiasm.
Figure 1. Three principal axes for the measurement of affective well-being
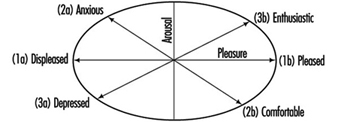
Job-related well-being has often been measured merely along the horizontal axis, extending from “feeling bad” to “feeling good”. The measurement is usually made with reference to a scale of job satisfaction, and data are obtained by workers’ indicating their agreement or disagreement with a series of statements describing their feelings about their jobs. However, job satisfaction scales do not take into account differences in mental arousal, and are to that extent relatively insensitive. Additional forms of measurement are also needed, in terms of the other two axes in the figure.
When low scores on the horizontal axis are accompanied by raised mental arousal (upper left quadrant), low well-being is typically evidenced in the forms of anxiety and tension; however, low pleasure in association with low mental arousal (lower left) is observable as depression and associated feelings. Conversely, high job-related pleasure may be accompanied by positive feelings that are characterized either by enthusiasm and energy (3b) or by psychological relaxation and comfort (2b). This latter distinction is sometimes described in terms of motivated job satisfaction (3b) versus resigned, apathetic job satisfaction (2b).
In studying the impact of organizational and psychosocial factors on employee well-being, it is desirable to examine all three of the axes. Questionnaires are widely used for this purpose. Job satisfaction (1a to 1b) may be examined in two forms, sometimes referred to as “facet-free” and “facet-specific” job satisfaction. Facet-free, or overall, job satisfaction is an overarching set of feelings about one’s job as a whole, whereas facet-specific satisfactions are feelings about particular aspects of a job. Principal facets include pay, working conditions, one’s supervisor and the nature of the work undertaken.
These several forms of job satisfaction are positively intercorrelated, and it is sometimes appropriate merely to measure overall, facet-free satisfaction, rather than to examine separate, facet-specific satisfactions. A widely used general question is “On the whole, how satisfied are you with the work you do?”. Commonly used responses are very dissatisfied, a little dissatisfied, moderately satisfied, very satisfied and extremely satisfied, and are designated by scores from 1 to 5 respectively. In national surveys it is usual to find that about 90% of employees report themselves as satisfied to some degree, and a more sensitive measuring instrument is often desirable to yield more differentiated scores.
A multi-item approach is usually adopted, perhaps covering a range of different facets. For instance, several job satisfaction questionnaires ask about a person’s satisfaction with facets of the following kinds: the physical work conditions; the freedom to choose your own method of working; your fellow workers; the recognition you get for good work; your immediate boss; the amount of responsibility you are given; your rate of pay; your opportunity to use your abilities; relations between managers and workers; your workload; your chance of promotion; the equipment you use; the way your firm is managed; your hours of work; the amount of variety in your job; and your job security. An average satisfaction score may be calculated across all the items, responses to each item being scored from 1 to 5, for instance (see the preceding paragraph). Alternatively, separate values can be computed for “intrinsic satisfaction” items (those dealing with the content of the work itself) and “extrinsic satisfaction” items (those referring to the context of the work, such as colleagues and working conditions).
Self-report scales which measure axes two and three have often covered only one end of the possible distribution. For example, some scales of job-related anxiety ask about a worker’s feelings of tension and worry when on the job (2a), but do not in addition test for more positive forms of affect on this axis (2b). Based on studies in several settings (Watson, Clark and Tellegen 1988; Warr 1990), a possible approach is as follows.
Axes 2 and 3 may be examined by putting this question to workers: “Thinking of the past few weeks, how much of the time has your job made you feel each of the following?”, with response options of never, occasionally, some of the time, much of the time, most of the time, and all the time (scored from 1 to 6 respectively). Anxiety-to-comfort ranges across these states: tense, anxious, worried, calm, comfortable and relaxed. Depression-to-enthusiasm covers these states: depressed, gloomy, miserable, motivated, enthusiastic and optimistic. In each case, the first three items should be reverse-scored, so that a high score always reflects high well-being, and the items should be mixed randomly in the questionnaire. A total or average score can be computed for each axis.
More generally, it should be noted that affective well-being is not determined solely by a person’s current environment. Although job characteristics can have a substantial effect, well-being is also a function of some aspects of personality; people differ in their baseline well-being as well as in their reactions to particular job characteristics.
Relevant personality differences are usually described in terms of individuals’ continuing affective dispositions. The personality trait of positive affectivity (corresponding to the upper right-quadrant) is characterized by generally optimistic views of the future, emotions which tend to be positive and behaviours which are relatively extroverted. On the other hand, negative affectivity (corresponding to the upper left-hand quadrant) is a disposition to experience negative emotional states. Individuals with high negative affectivity tend in many situations to feel nervous, anxious or upset; this trait is sometimes measured by means of personality scales of neuroticism. Positive and negative affectivities are regarded as traits, that is, they are relatively constant from one situation to another, whereas a person’s well-being is viewed as an emotional state which varies in response to current activities and environmental influences.
Measures of well-being necessarily identify both the trait (the affective disposition) and the state (current affect). This fact should be borne in mind in examining people’s well-being score on an individual basis, but it is not a substantial problem in studies of the average findings for a group of employees. In longitudinal investigations of group scores, observed changes in well-being can be attributed directly to changes in the environment, since every person’s baseline well-being is held constant across the occasions of measurement; and in cross-sectional group studies an average affective disposition is recorded as a background influence in all cases.
Note also that affective well-being may be viewed at two levels. The more focused perspective relates to a specific domain, such as an occupational setting: this may be a question of “job-related” well-being (as discussed here) and is measured through scales which directly concern feelings when a person is at work. However, more wide-ranging, “context-free” or “general,” well-being is sometimes of interest, and measurement of that wider construct requires a less specific focus. The same three axes should be examined in both cases, and more general scales are available for life satisfaction or general distress (axis 1), context-free anxiety (axis 2) and context-free depression (axis 3).
Immunological Reactions
When a human being or an animal is subjected to a psychological stress situation, there is a general response involving psychological as well as somatic (bodily) responses. This is a general alarm response, or general activation or wake-up call, which affects all physiological responses, including the musculoskeletal system, the vegetative system (the autonomic system), the hormones and also the immune system.
Since the 1960s, we have been learning how the brain, and through it, psychological factors, regulates and influences all physiological processes, whether directly or indirectly. Previously it was held that large and essential parts of our physiology were regulated “unconsciously,” or not by brain processes at all. The nerves that regulate the gut, glands and the cardiovascular system were “autonomic”, or independent of the central nervous system (CNS); similarly, the hormones and the immune system were beyond central nervous control. However, the autonomic nervous system is regulated by the limbic structures of the brain, and may be brought under direct instrumental control through classical and instrumental learning procedures. The fact that the central nervous system controls endocrinological processes is also well established.
The last development to undercut the view that the CNS was isolated from many physiological processes was the evolution of psychoimmunology. It has now been demonstrated that the interaction of the brain (and psychological processes), may influence immune processes, either via the endocrine system or by direct innervation of lymphoid tissue. The white blood cells themselves may also be influenced directly by signal molecules from nervous tissue. Depressed lymphocyte function has been demonstrated to follow bereavement (Bartrop et al. 1977), and conditioning of the immune-suppressive response in animals (Cohen et al. 1979) and psychological processes were shown to have effects bearing on animal survival (Riley 1981); these discoveries were milestones in the development of psychoimmunology.
It is now well established that psychological stress produces changes in the level of antibodies in the blood, and in the level of many of the white blood cells. A brief stress period of 30 minutes may produce significant increases in lymphocytes and natural killer (NK) cells. Following more long-lasting stress situations, changes are also found in the other components of the immune system. Changes have been reported in the counts of almost all types of white blood cell and in the levels of immunoglobulins and their complements; the changes also affect important elements of the total immune response and the “immune cascade” as well. These changes are complex and seem to be bidirectional. Both increases and decreases have been reported. The changes seem to depend not only on the stress-inducing situation, but on also what type of coping and defence mechanisms the individual is using to handle this situation. This is particularly clear when the effects of real long-lasting stress situations are studied, for instance those associated with the job or with difficult life situations (“life stressors”). Highly specific relationships between coping and defence styles and several subsets of immune cells (number of lympho-, leuko- and monocytes; total T cells and NK cells) have been described (Olff et al. 1993).
The search for immune parameters as markers for long-lasting, sustained stress has not been all that successful. Since the relationships between immunoglobulins and stress factors have been demonstrated to be so complex, there is, understandably, no simple marker available. Such relationships as have been found are sometimes positive, sometimes negative. As far as psycho-logical profiles are concerned, to some extent the correlation matrix with one and the same psychological battery shows different patterns, varying from one occupational group to another (Endresen et al. 1991). Within each group, the patterns seem stable over long periods of time, up to three years. It is not known whether there are genetic factors that influence the highly specific relationships between coping styles and immune responses; if so, the manifestions of these factors must be highly dependent on interaction with life stressors. Also, it is not known whether it is possible to follow an individual’s stress level over a long period, given that the individual’s coping, defence and immune response style is known. This type of research is being pursued with highly selected personnel, for instance astronauts.
There may be a major flaw in the basic argument that immunoglobulins can be used as valid health risk markers. The original hypothesis was that low levels of circulating immunoglobulins might signal a low resistance and low immune competence. However, low values may not signal low resistance: they may only signal that this particular individual has not been challenged by infectious agents for a while—in fact, they may signal an extraordinary degree of health. The low values sometimes reported from returning astronauts and Antarctic personnel may not be a signal of stress, but only of the low levels of bacterial and viral challenge in the environment they have left.
There are many anecdotes in the clinical literature suggesting that psychological stress or critical life events can have an impact on the course of serious and non-serious illness. In the opinion of some, placebos and “alternative medicine” may exert their effects through psychoimmunological mechanisms. There are claims that reduced (and sometimes increased) immune competence should lead to increased susceptibility to infections in animals and in humans, and to inflammatory states like rheumatoid arthritis as well. It has been demonstrated convincingly that psychological stress affects the immune response to various types of inoculations. Students under examination stress report more symptoms of infectious illness in this period, which coincides with poorer cellular immune control (Glaser et al. 1992). There are also some claims that psychotherapy, in particular cognitive stress-management training, together with physical training, may affect the antibody response to viral infection.
There are also some positive findings with regard to cancer development, but only a few. The controversy over the claimed relationship between personality and cancer susceptibility has not been solved. Replications should be extended to include measures of immune responses to other factors, including lifestyle factors, which may be related to psychology, but the cancer effect may be a direct consequence of the lifestyle.
There is ample evidence that acute stress alters immune functions in human subjects and that chronic stress may also affect these functions. But to what extent are these changes valid and useful indicators of job stress? To what extent are immune changes—if they occur—a real health risk factor? There is no consensus in the field as of the time of this writing (1995).
Sound clinical trials and sound epidemiological research are required to advance in this field. But this type of research requires more funds than are available to the researchers. This work also requires an understanding of the psychology of stress, which is not always available to immunologists, and a profound understanding of how the immune system operates, which is not always available to psychologists.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."