- You are here:
-
Home

-
Contents (2)
-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
-
Storage
- Yassi, Annalee

Yassi, Annalee
Address: Occupational & Environemtal Health Unit, University of Manitoba, 5112-750 Bannatyne Avenue, Winnipeg, MB Manitoba R3E 0W3
Country: Canada
Phone: 1 (204) 789-3289
Fax: 1 (204) 772-8748
E-mail: yassi@bldghsc.lan1.umanitoba.ca
Linkages Between Environmental and Occupational Health
Development, and industrialization in particular, have made immense positive contributions to health, including greater personal and social wealth, as well as vastly improved health and education services, transportation and communication. Unquestionably, on the global scale, people are living longer and are healthier than they were centuries and even decades ago. However, industrialization has also had adverse health consequences not only for workforces, but for the general population as well. These effects have been caused either directly by exposure to safety hazards and harmful agents, or indirectly through environmental degradation locally and globally (see “Industrial pollution in developing countries” in this chapter).
This article outlines the nature of environmental health hazards and the reasons for linking environmental health with occupational health.
Environmental health hazards, like occupational health hazards, may be biological, chemical, physical, biomechanical or psychosocial in nature. Environmental health hazards include traditional hazards of poor sanitation and shelter, as well as agricultural and industrial contamination of air, water, food and land. These hazards have resulted in a host of health impacts, ranging from catastrophic direct effects (e.g., the recent cholera epidemic in Latin America and the chemical poisoning outbreak in Bhopal, India), to chronic effects (e.g., in Minamata, Japan), to subtle, indirect, and even disputed effects (e.g., in Love Canal, USA). Table 1 summarizes some of the major notorious disasters in the last half century that have caused “environmental disease” outbreaks. There are undeniably countless other examples of environmental disease outbreaks, some of which are not easily detectable on the macrostatistical level. Meanwhile, over a billion people in the world lack access to safe drinking water (WHO 1992b) and over 600 million are exposed to ambient levels of sulphur dioxide that well exceed recommended levels. Moreover the pressure on agriculture and food production as both population and per capita demand increase, will likely lead to a greater burden on the environment (see “Food and agriculture” in this chapter). Environmental health impacts thus include the indirect effects of industrial disruption of adequate food and housing, as well as the degradation of the global systems on which the health of the planet depends.
Table 1. Selected major "environmental disease" outbreaks
|
Location and year |
Environmental hazard |
Type of disease |
Number affected |
|
London, UK 1952 |
Severe air-pollution with sulphur dioxide and suspended particulate matter (SPM) |
Increase in heart and lung disease manifestations |
3,000 deaths, many others ill |
|
Toyama, Japan 1950s |
Cadmium in rice |
Kidney and bone disease (“Itai-itai disease”) |
200 with severe disease, many more with slight effects |
|
South-east Turkey 1955-61 |
Hexachlorobenzene in seed grains |
Porphyria; neurological disease |
3,000 |
|
Minamata, Japan 1956 |
Methylmercury in fish |
Neurological disease (“Minimata disease”) |
200 with severe disease, 2,000 suspected |
|
USA cities 1960s-70s |
Lead in paint |
Anaemia, behavioural and mental effects |
Many thousands |
|
Fukuoka, Japan 1968 |
Polychlorinated biphenyls (PCBs) in food oil |
Skin disease, general weakness |
Several thousands |
|
Iraq 1972 |
Methylmercury in seed grains |
Neurological disease |
500 deaths, 6,500 hospitalized |
|
Madrid, Spain 1981 |
Aniline or other toxin in food oil |
Various symptoms |
340 deaths, 20,000 cases |
|
Bhopal, India 1985 |
Methylisocyanate |
Acute lung disease |
2,000 deaths, 200,000 poisoned |
|
California, USA 1985 |
Carbamate pesticide in watermelons |
Gastrointestinal, skeletal, muscle, autonomic and central nervous system effects (Carbamate illness) |
1,376 reported cases of illness resulting from consumption, 17 severely ill |
|
Chernobyl, USSR 1986 |
Iodine-134, Caesium-134 and -137 from a reactor explosion |
Radiation illness (including increases in cancer and thyroid diseases in children) |
300 injured, 28 died within 3 months, more than 600 cases of thyroid cancer |
|
Goiánia, Brazil 1987 |
Caesium-137 from an abandoned cancer therapy machine |
Radiation illness (follow-up of in utero exposures continuing) |
Some 240 people were contaminated and 2 died |
|
Peru 1991 |
Cholera epidemic |
Cholera |
139 deaths, many thousand ill |
In many countries large-scale agriculture and the concomitant active use of toxic pesticides is a major health hazard both for workers and for their households. Pollution by fertilizers or biological waste from the food industry, paper industry and so on can also have harmful effects on waterways, reducing fishing and food supplies. The fishermen and gatherers of other seafood may have to travel much further to get their daily catch, with increased risks of drowning accidents and other mishaps. The spread of tropical disease by the environmental changes associated with developments such as the building of dams, roads and so on constitutes another type of environmental health risk. The new dam may create breeding grounds for schistosomiasis, a debilitating disease affecting rice farmers who have to walk in water. The new road may create fast communication between an area with endemic malaria and another area hitherto spared from this disease.
It should be pointed out that the major basis for a harmful environment in the workplace or in the general environment is poverty. The traditional health threats in developing countries or in poor sections of any country include poor sanitation, water and food which spreads communicable diseases, poor housing with high exposures to cooking smoke and high fire risks, as well as high injury risks in small-scale agriculture or cottage industries. Reduction of poverty and improved living and working conditions is a fundamental priority for improved occupational and environmental health for billions of people. Despite efforts for energy conservation and sustainable development, failure to address the underlying inequities in wealth distribution threatens the global ecosystem.
Forests, for example, which represent the culmination of ecological successional processes, are being destroyed at an alarming rate, due to commercial logging and clearance by impoverished peoples for agriculture and firewood. The effects of forest depletion include soil erosion, which, if extreme, can lead to desertification. Loss of biodiversity is an important consequence (see “Species extinction, biodiversity loss and human health” in this chapter). It is estimated that one-third of all carbon dioxide emissions are from the burning of tropical forests (the importance of carbon dioxide in creating global warming is discussed in “Global climate change and ozone depletion” in this chapter). Thus, addressing poverty is imperative with respect to global environmental health as well as individual, community and regional well-being.
Reasons for Linking Environmental and Occupational Health
The main link between the workplace and the general environment is that the source of the hazard is usually the same, whether it is an agricultural activity or an industrial activity. In order to control the health hazard, a common approach may work effectively in both settings. This is particularly so when it comes to the choice of chemical technologies for production. If an acceptable result or product can be produced with a less toxic chemical, the choice of such a chemical can reduce or even eliminate the health risk. One example is the use of safer water-based paints instead of paints made with toxic organic solvents. Another example is the choice of non-chemical pest-control methods whenever this is possible. In fact, in many cases, particularly in the developing world, there is no separation between the home and the workplace; thus the setting is truly the same.
It is now well recognized that the scientific knowledge and training required to assess and control environmental health hazards are, for the most part, the same skills and knowledge required to address health hazards within the workplace. Toxicology, epidemiology, occupational hygiene, ergonomics, safety engineering - in fact, the very disciplines included in this Encyclopaedia - are the basic tools of environmental science. The process of risk assessment and risk management is also the same: identify the hazards, categorize the risks, assess the exposure and estimate risk. This is followed by evaluating control options, controlling the exposure, communicating the risk to the public and establishing an on-going exposure- and risk-monitoring programme. Thus occupational and environmental health are strongly linked by common methodologies, particularly in health assessment and exposure control.
The identification of environmental health hazards has often come from observations of adverse health outcomes among workers; and unquestionably it is in the workplace that the impact of industrial exposures is best understood. Documentation of health effects generally comes from one of three sources: animal or other laboratory experiments (both non-human and controlled human), accidental high-level exposures or the epidemiological studies that usually follow such exposures. To conduct an epidemiological study it is necessary to be able to define both the exposed population and the nature and level of the exposure, as well as to ascertain the negative health effect. It is generally easier to define the members of a workforce than to determine the membership of a community, particularly in a community that is transient; the nature and level of exposure to various members of the cohort are generally more clear-cut in a workplace population than in a community; and the outcomes of high levels of exposure are almost always easier to delineate than more subtle changes attributable to low-level exposure. While there are some examples of exposure outside factory gates approaching the worst occupational exposures (e.g., cadmium exposure from mining in China and Japan; lead and cadmium emissions from smelters in Upper Silesia, Poland), the levels of exposure are generally much higher to a workforce than to the surrounding community (WHO 1992b).
Since adverse health outcomes are more apparent in workers, information on occupational health effects of many toxic exposures (including heavy metals such as lead, mercury, arsenic and nickel, as well as such well-known carcinogens as asbestos) has been used to calculate the health risk to the wider community. With respect to cadmium, for example, as early as 1942 reports began to appear of cases of osteomalacia with multiple fractures among workers in a French factory producing alkaline batteries. During the 1950s and 1960s cadmium intoxication was considered to be strictly an occupational disease. However, the knowledge gained from the workplace helped achieve the recognition that osteomalacia and kidney disease that was occurring in Japan at this time, “Itai-itai” disease, was indeed due to contamination of rice from irrigation of soil with water contaminated with cadmium from industrial sources (Kjellström 1986). Thus occupational epidemiology has been able to make a substantive contribution to knowledge of the effects of environmental exposure, constituting another reason for linking the two fields.
On an individual level, occupational disease affects well-being in the home and the community; and, universally, an individual who is ill from inadequacies in the home and the community cannot be productive in the workplace.
Strictly from a scientific viewpoint, there is a need to consider total (environmental plus occupational) exposures in order to truly assess health impact and establish dose-response relationships. Pesticide exposure is a classic example wherein occupational exposure may be supplemented by considerable environmental exposure, through food and water-source contamination, and through non-occupational airborne exposure. From outbreaks in which over 100 poisonings occurred from contaminated food alone, over 15,000 cases and 1,500 deaths due to pesticide poisoning have been documented by the WHO (1990e). In one study of Central American cotton growers using pesticides, not only did very few of the workers have access to protective clothing, but virtually all of the workers lived within 100 metres of the cotton fields, many in temporary housing with no walls for protection from aerial pesticide spraying. The workers also often washed in irrigation channels containing pesticide residues, resulting in increased exposures (Michaels, Barrera and Gacharna 1985). To understand the relationship between pesticide exposure and any health effects reported, all sources of exposure should be taken into consideration. Thus ensuring that occupational and environmental exposures are evaluated together improves the accuracy of exposure assessment in both areas.
The health problems caused by occupational and environmental hazards are particularly acute in developing countries, where well established methods of hazard control are less likely to be applied because of limited awareness of the hazards, low political priority of health and environment matters, limited resources or lack of appropriate occupational and environmental health management systems. A major impediment to environmental health hazard control in many parts of the world is the lack of people with appropriate training. It has been documented that developing countries suffer from a severe shortage of expert staff in occupational health (Noweir 1986). In 1985 a WHO expert committee also concluded that there is an urgent need for staff trained in environmental health matters; indeed Agenda 21, the internationally agreed upon strategy taken by the United Nations Conference on Environment and Development (UN 1993), identifies training (national “capacity building”) as a key element of promoting human health through sustainable development. Where resources are limited, it is not feasible to train one group of people to look after health concerns within the workplace, and another group to attend to hazards outside the factory gate.
Even in developed countries, there is a strong trend to make most efficient use of resources by training and employing “occupational and environmental health” professionals. Today, businesses must find ways to manage their affairs logically and efficiently within the societal framework of duty, law and financial policy. Combining occupational and environment health under one roof is one way of achieving this goal.
Broad environmental concerns must be taken into consideration in designing workplaces and deciding on industrial hygiene control strategies. Substituting for one substance another one that is less acutely toxic may make good occupational health sense; however, if the new substance is not biodegradable, or damages the ozone layer, it would not be an appropriate exposure control solution—it would only move the problem elsewhere. The use of chlorofluorocarbons, now widely used as a refrigerant instead of the more acutely dangerous substance ammonia, is the classic example of what is now known to have been an environmentally inappropriate substitution. Thus linking occupational and environmental health minimizes unwise exposure control decisions.
While understanding of the health effects of various deleterious exposures has usually come from the workplace, the public health impact of environmental exposures to these same agents has often been a major force in stimulating clean-up efforts both inside the workplace and in the surrounding community. For example, discovery of high lead levels in workers’ blood by an industrial hygienist in a lead foundry in Bahia, Brazil, led to investigations of lead in the blood of children in nearby residential areas. The finding that the children had high lead levels was a major impetus in the company taking action to reduce occupational exposures as well as lead emissions from the factory (Nogueira 1987), although occupational exposures still remain substantially higher than would be tolerated by the general community.
In fact, environmental health standards are usually much stricter than occupational health standards. The WHO’s recommended guideline values for selected chemicals provide an example. The rationale for the difference is generally that the community consists of sensitive populations including the very old, the ill, young children and pregnant women, whereas the workforce is at least healthy enough to work. Also, it is often argued that risk is more “acceptable” to a workforce, as these people are benefiting by having a job, and are therefore more willing to accept the risk. Many political, ethical, as well as scientific, debates rage around the question of standards. Linking occupational and environmental health can be a positive contribution to sorting out these controversies. In this regard, tightening the connection between occupational and environmental health may facilitate greater consistency in approaches to standard setting.
Likely inspired at least in part by the active debate about the environment and sustainable development brought to the forefront by Agenda 21, many occupational health professional organizations have changed their names to “occupational and environmental” organizations in acknowledgement that their members are increasingly devoting their attention to environmental health hazards both inside and outside the workplace. Further, as noted in the chapter on ethics , the International Code of Ethics for Occupational Health Professionals states that the duty to protect the environment is part and parcel of the ethical obligations of occupational health professionals.
In summary, occupational and environmental health are strongly linked by:
- the very fact that the source of the health threat is usually the same
- common methodologies, particularly in health assessment and exposure control
- the contribution that occupational epidemiology makes to knowledge of the effects of environmental exposure
- the effects that occupational disease has on well-being in the home and the community, and conversely the effect of environmental pathology on worker productivity
- the scientific need to consider total exposures in order to determine dose-response relationships
- the efficiency in human resource development and utilization gained by such a linkage
- improvements in exposure control decisions stemming from the broader view
- greater consistency in standard setting facilitated by the link
- the fact that linking environmental and occupational health enhances the incentive for rectification of hazards to both the workforce and the community.
The desirability of bringing together occupational and environmental health notwithstanding, each has a unique and specific orientation that should not be lost. Occupational health must continue to focus on workers’ health, and environmental health must continue to concern itself with the health of the general public. None the less, even where it is desirable for professionals to operate strictly in only one of these fields, having a good appreciation of the other enhances the credibility, knowledge base and effectiveness of the overall endeavour. It is in this spirit that this chapter is presented.
Managing Chemical Hazards in Hospitals
The vast array of chemicals in hospitals, and the multitude of settings in which they occur, call for a systematic approach to their control. A chemical-by-chemical approach to prevention of exposures and their deleterious outcome is simply too inefficient to handle a problem of this scope. Moreover, as noted in the article “Overview of chemical hazards in health care”, many chemicals in the hospital environment have been inadequately studied; new chemicals are constantly being introduced and for others, even some that have become quite familiar (e.g., gloves made of latex), new hazardous effects are only now becoming manifest. Thus, while it is useful to follow chemical-specific control guidelines, a more comprehensive approach is needed whereby individual chemical control policies and practices are superimposed on a strong foundation of general chemical hazard control.
The control of chemical hazards in hospitals must be based on classic principles of good occupational health practice. Because health care facilities are accustomed to approaching health through the medical model, which focuses on the individual patient and treatment rather than on prevention, special effort is required to ensure that the orientation for handling chemicals is indeed preventive and that measures are principally focused on the workplace rather than on the worker.
Environmental (or engineering) control measures are the key to prevention of deleterious exposures. However, it is necessary to train each worker correctly in appropriate exposure prevention techniques. In fact, right-to-know legislation, as described below, requires that workers be informed of the hazards with which they work, as well as of the appropriate safety precautions. Secondary prevention at the level of the worker is the domain of medical services, which may include medical monitoring to ascertain whether health effects of exposure can be medically detected; it also consists of prompt and appropriate medical intervention in the event of accidental exposure. Chemicals that are less toxic must replace more toxic ones, processes should be enclosed wherever possible and good ventilation is essential.
While all means to prevent or minimize exposures should be implemented, if exposure does occur (e.g., a chemical is spilled), procedures must be in place to ensure prompt and appropriate response to prevent further exposure.
Applying the General Principles of Chemical Hazard Control in the Hospital Environment
The first step in hazard control is hazard identification. This, in turn, requires a knowledge of the physical properties, chemical constituents and toxicological properties of the chemicals in question. Material safety data sheets (MSDSs), which are becoming increasingly available by legal requirement in many countries, list such properties. The vigilant occupational health practitioner, however, should recognize that the MSDS may be incomplete, particularly with respect to long-term effects or effects of low-dose chronic exposure. Hence, a literature search may be contemplated to supplement the MSDS material, when appropriate.
The second step in controlling a hazard is characterizing the risk. Does the chemical pose a carcinogenic risk? Is it an allergen? A teratogen? Is it mainly short-term irritancy effects that are of concern? The answer to these questions will influence the way in which exposure is assessed.
The third step in chemical hazard control is to assess the actual exposure. Discussion with the health care workers who use the product in question is the most important element in this endeavour. Monitoring methods are necessary in some situations to ascertain that exposure controls are functioning properly. These may be area sampling, either grab sample or integrated, depending on the nature of the exposure; it may be personal sampling; in some cases, as discussed below, medical monitoring may be contemplated, but usually as a last resort and only as back-up to other means of exposure assessment.
Once the properties of the chemical product in question are known, and the nature and extent of exposure are assessed, a determination could be made as to the degree of risk. This generally requires that at least some dose-response information be available.
After evaluating the risk, the next series of steps is, of course, to control the exposure, so as to eliminate or at least minimize the risk. This, first and foremost, involves applying the general principles of exposure control.
Organizing a Chemical Control Programme in Hospitals
The traditional obstacles
The implementation of adequate occupational health programmes in health care facilities has lagged behind the recognition of the hazards. Labour relations are increasingly forcing hospital management to look at all aspects of their benefits and services to employees, as hospitals are no longer tacitly exempt by custom or privilege. Legislative changes are now compelling hospitals in many jurisdictions to implement control programmes.
However, obstacles remain. The preoccupation of the hospital with patient care, emphasizing treatment rather than prevention, and the staff’s ready access to informal “corridor consultation”, have hindered the rapid implementation of control programmes. The fact that laboratory chemists, pharmacists and a host of medical scientists with considerable toxicological expertise are heavily represented in management has, in general, not served to hasten the development of programmes. The question may be asked, “Why do we need an occupational hygienist when we have all these toxicology experts?” To the extent that changes in procedures threaten to have an impact on the tasks and services provided by these highly skilled personnel, the situation may be made worse: “We cannot eliminate the use of Substance X as it is the best bactericide around.” Or, “If we follow the procedure that you are recommending, patient care will suffer.” Moreover, the “we don’t need training” attitude is commonplace among the health care professions and hinders the implementation of the essential components of chemical hazard control. Internationally, the climate of cost constraint in health care is clearly also an obstacle.
Another problem of particular concern in hospitals is preserving the confidentiality of personal information about health care workers. While occupational health professionals should need only to indicate that Ms. X cannot work with chemical Z and needs to be transferred, curious clinicians are often more prone to push for the clinical explanation than their non-health care counterparts. Ms. X may have liver disease and the substance is a liver toxin; she may be allergic to the chemical; or she may be pregnant and the substance has potential teratogenic properties. While the need to alter the work assignment of particular individuals should not be routine, the confidentiality of the medical details should be protected if it is necessary.
Right-to-know legislation
Many jurisdictions around the world have implemented right-to-know legislation. In Canada, for example, WHMIS has revolutionized the handling of chemicals in industry. This country-wide system has three components: (1) the labelling of all hazardous substances with standardized labels indicating the nature of the hazard; (2) the provision of MSDSs with the constituents, hazards and control measures for each substance; and (3) the training of workers to understand the labels and the MSDSs and to use the product safely.
Under WHMIS in Canada and OSHA’s Hazard Communications requirements in the United States, hospitals have been required to construct inventories of all chemicals on the premises so that those that are “controlled substances” can be identified and addressed according to the legislation. In the process of complying with the training requirements of these regulations, hospitals have had to engage occupational health professionals with appropriate expertise and the spin-off benefits, particularly when bipartite train-the-trainer programmes were conducted, have included a new spirit to work cooperatively to address other health and safety concerns.
Corporate commitment and the role of joint health and safety committees
The most important element in the success of any occupational health and safety programme is corporate commitment to ensure its successful implementation. Policies and procedures regarding the safe handling of chemicals in hospitals must be written, discussed at all levels within the organization and adopted and enforced as corporate policy. Chemical hazard control in hospitals should be addressed by general as well as specific policies. For example, there should be a policy on responsibility for the implementation of right-to-know legislation that clearly outlines each party’s obligations and the procedures to be followed by individuals at each level of the organization (e.g., who chooses the trainers, how much work time is allowed for preparation and provision of training, to whom should communication regarding non-attendance be communicated and so on). There should be a generic spill clean-up policy indicating the responsibility of the worker and the department where the spill occurred, the indications and protocol for notifying the emergency response team, including the appropriate in-hospital and external authorities and experts, follow-up provisions for exposed workers and so on. Specific policies should also exist regarding the handling, storage and disposal of specific classes of toxic chemicals.
Not only is it essential that management be strongly committed to these programmes; the workforce, through its representatives, must also be actively involved in the development and implementation of policies and procedures. Some jurisdictions have legislatively mandated joint (labour-management) health and safety committees that meet at a minimum prescribed interval (bimonthly in the case of Manitoba hospitals), have written operating procedures and keep detailed minutes. Indeed in recognizing the importance of these committees, the Manitoba Workers’ Compensation Board (WCB) provides a rebate on WCB premiums paid by employers based on the successful functioning of these committees. To be effective, the members must be appropriately chosen—specifically, they must be elected by their peers, knowledgeable about the legislation, have appropriate education and training and be allotted sufficient time to conduct not only incident investigations but regular inspections. With respect to chemical control, the joint committee has both a pro-active and a re-active role: assisting in setting priorities and developing preventive policies, as well as serving as a sounding board for workers who are not satisfied that all appropriate controls are being implemented.
The multidisciplinary team
As noted above, the control of chemical hazards in hospitals requires a multidisciplinary endeavour. At a minimum, it requires occupational hygiene expertise. Generally hospitals have maintenance departments that have within them the engineering and physical plant expertise to assist a hygienist in determining whether workplace alterations are necessary. Occupational health nurses also play a prominent role in evaluating the nature of concerns and complaints, and in assisting an occupational physician in ascertaining whether clinical intervention is warranted. In hospitals, it is important to recognize that numerous health care professionals have expertise that is quite relevant to the control of chemical hazards. It would be unthinkable to develop policies and procedures for the control of laboratory chemicals without the involvement of lab chemists, for example, or procedures for handling anti-neoplastic drugs without the involvement of the oncology and pharmacology staff. While it is wise for occupational health professionals in all industries to consult with line staff prior to implementing control measures, it would be an unforgivable error to fail to do so in health care settings.
Data collection
As in all industries, and with all hazards, data need to be compiled both to help in priority setting and in evaluating the success of programmes. With respect to data collection on chemical hazards in hospitals, minimally, data need to be kept regarding accidental exposures and spills (so that these areas can receive special attention to prevent recurrences); the nature of concerns and complaints should be recorded (e.g., unusual odours); and clinical cases need to be tabulated, so that, for example, an increase in dermatitis from a given area or occupational group could be identified.
Cradle-to-grave approach
Increasingly, hospitals are becoming cognizant of their obligation to protect the environment. Not only the workplace hazardous properties, but the environmental properties of chemicals are being taken into consideration. Moreover, it is no longer acceptable to pour hazardous chemicals down the drain or release noxious fumes into the air. A chemical control programme in hospitals must, therefore, be capable of tracking chemicals from their purchase and acquisition (or, in some cases, synthesis on site), through the work handling, safe storage and finally to their ultimate disposal.
Conclusion
It is now recognized that there are thousands of potentially very toxic chemicals in the work environment of health care facilities; all occupational groups may be exposed; and the nature of the exposures are varied and complex. Nonetheless, with a systematic and comprehensive approach, with strong corporate commitment and a fully informed and involved workforce, chemical hazards can be managed and the risks associated with these chemicals controlled.
Health Care: Its Nature and its Occupational Health Problems
Health care is a labour intensive industry and, in most countries, health care workers (HCWs) constitute a major sector of the workforce. They comprise a wide range of professional, technical and support personnel working in a large variety of settings. In addition to health professionals, laboratory technicians, pharmacists, social workers and others involved in clinical services, they include administrative and clerical personnel, housekeeping and dietary staff, laundry workers, engineers, electricians, painters and maintenance workers who repair and refurbish the building and the equipment it contains. In contrast with those providing direct care, these support workers usually have only casual, incidental contact with patients.
HCWs represent diverse educational, social and ethnic levels and are usually predominantly female. Many, particularly in home care, are employed in entry-level positions and require considerable basic training. Table 1 lists samples of health care functions and associated occupations.
Table 1. Examples of health care functions and associated occupations
|
Functions |
Occupational category * |
Specific occupations |
|
Direct patient care |
Health-diagnosing occupations |
Physicians |
|
Technical support |
Health technicians |
Clinical laboratory technicians |
|
Services |
Health services |
Dental assistants |
|
Administrative support |
Clerical services |
Billing clerks |
|
Research |
Scientific occupations |
Scientists and research |
* Occupational categories are, in part, adapted from those used by the US Department of Labor, Bureau of Labor Statistics.
A segment of the health sector (unfortunately, often too small and under-resourced in most communities) is devoted to direct and indirect preventive services. The major focus of the health care industry, however, is the diagnosis, treatment and care of the sick. This creates a special set of dynamics, for the sick exhibit varying levels of physical and emotional dependencies that set them apart from the customers in such personal services industries as, for example, retail trade, restaurants and hotels. They require, and traditionally receive, special services and considerations, often on an emergency basis, provided frequently at the expense of the HCWs’ personal comfort and safety.
Reflecting their size and numbers of employees, acute and long-term care facilities constitute perhaps the most prominent elements in the health care industry. They are supplemented by outpatient clinics, “surgicenters” (facilities for outpatient surgery), clinical and pathological laboratories, pharmacies, x-ray and imaging centres, ambulance and emergency care services, individual and group offices, and home care services. These may be located within a hospital or operated elsewhere under its aegis, or they may be free-standing and operated independently. It should be noted that there are profound differences in the way health services are delivered, ranging from the well-organized, “high tech” care available in urban centres in developed countries to the underserved areas in rural communities, in developing countries and in inner-city enclaves in many large cities.
Superimposed on the health care system is a massive educational and research establishment in which students, faculty, researchers and support staffs often come in direct contact with patients and participate in their care. This comprises schools of medicine, dentistry, nursing, public health, social work and the variety of technical disciplines involved in health care.
The health care industry has been undergoing profound changes during the past few decades. Ageing of the population, especially in developed countries, has amplified the use of nursing homes, domiciliary facilities and home care services. Scientific and technological developments have not only led to the creation of new types of facilities staffed by new classes of specially-trained personnel, but they have also de-emphasized the role of the acute care hospital. Now, many services requiring inpatient care are being provided on an ambulatory basis. Finally, fiscal constraints dictated by the continuing escalation of health care costs have been reconfiguring the health care industry, at least in developing countries, resulting in pressure for cost-containment to be achieved through changes in the organization of health care services.
HCWs who are in direct contact with the sick, wherever they work, are exposed to a number of unique hazards. They face the risk of acquiring infections from the patients they serve, as well as the risk of musculoskeletal injuries when lifting, transferring or restraining them. Support staff not directly involved in patient care (e.g., laundry and housekeeping and materials handling workers) are not only routinely exposed to chemicals, such as cleaning agents and disinfectants of industrial strength, but are also exposed to biological hazards from contaminated linens and wastes (see figure 1). There is also the ethos of health care which, especially in emergency situations, requires HCWs to put the safety and comfort of their patients above their own. Coping with the stress of therapeutic failures, death and dying often takes its toll in worker burnout. All this is compounded by shift work, deliberate or inadvertent understaffing and the necessity of catering to the sometimes unreasonable demands from patients and their families. Finally, there is the threat of abuse and violence from patients, particularly when the job requires them to work alone or takes them into unsafe areas. All these are described in greater detail in other articles in this chapter and elsewhere in this Encyclopaedia.
Figure 1. Handling contaminated biological material

Health Sciences Centre, Winnipeg, Manitoba, Canada
The US National Institute for Occupational Safety and Health (NIOSH) reported that needle punctures, musculoskeletal sprains and back injuries probably were the most common injuries in the health care industry (Wugofski 1995). The World Health Organization (WHO) Conference on Occupational Hazards in 1981 identified as its five main areas of concern:
- cuts, lacerations and fractures
- back injuries
- lack of personal safety equipment
- poor maintenance of mechanical and electrical systems
- assault by patients.
Are they health care workers, too?
Often overlooked when considering the safety and well-being of health care workers are students attending medical, dental, nursing and other schools for health professionals and volunteers serving pro bono in healthcare facilities. Since they are not “employees” in the technical or legal sense of the term, they are ineligible for workers’ compensation and employment-based health insurance in many jurisdictions. Health care administrators have only a moral obligation to be concerned about their health and safety.
The clinical segments of their training bring medical, nursing and dental students into direct contact with patients who may have infectious diseases. They perform or assist in a variety of invasive procedures, including taking blood samples, and often do laboratory work involving body fluids and specimens of urine and faeces. They are usually free to wander about the facility, entering areas containing potential hazards often, since such hazards are rarely posted, without an awareness of their presence. They are usually supervised very loosely, if at all, while their instructors are often not very knowledgeable, or even interested, in matters of safety and health protection.
Volunteers are rarely permitted to participate in clinical care but they do have social contacts with patients and they usually have few restrictions with respect to areas of the facility they may visit.
Under normal circumstances, students and volunteers share with health care workers the risks of exposure to potentially harmful hazards. These risks are exacerbated at times of crisis and in emergencies when they step into or are ordered into the breech. Clearly, even though it may not be spelled out in laws and regulations or in organizational procedure manuals, they are more than entitled to the concern and protection extended to “regular” health care workers.
Leon Warshaw
Biological Hazards
Biological hazards, which pose a risk for infectious disease, are common throughout the world, but they are particularly problematic in developing countries. While the hepatitis B virus (HBV) is a nearly universal threat to HCWs, it is particularly important in African and Asian countries where this virus is endemic. As discussed later in this chapter, the risk of HBV transmission after percutaneous exposure to hepatitis B surface antigen (HBsAg) positive blood is approximately 100-fold higher than the risk of transmitting the human immunodeficiency virus (HIV) through percutaneous exposure to HIV-infected blood (i.e., 30% versus 0.3%). Nonetheless, there has indeed been an evolution of concern regarding parenteral exposure to blood and body fluids from the pre-HIV to the AIDS era. McCormick et al. (1991) found that the annual reported incidents of injuries from sharp instruments increased more than threefold during a 14-year period and among medical house officers the reported incidents increased ninefold. Overall, nurses incur approximately two-thirds of the needlestick injuries reported. Yassi and McGill (1991) also noted that nursing staff, particularly nursing students, are at highest risk for needlestick injuries, but they also found that approximately 7.5% of medical personnel reported exposures to blood and body fluids, a figure that is probably low because of underreporting. These data were consistent with other reports which indicated that, while there is increased reporting of needlesticks reflecting concerns about HIV and AIDS, certain groups continue to underreport. Sterling (1994) concludes that underreporting of needlestick injuries ranges from 40 to 60%.
Certain risk factors clearly enhance the likelihood of transmission of bloodborne diseases; these are discussed in the article “Prevention of occupational transmission of bloodborne pathogens”. Frequent exposure has indeed been associated with high seroprevalence rates of hepatitis B among laboratory workers, surgeons and pathologists. The risk of hepatitis C is also increased. The trend towards greater attention to prevention of needlestick injuries is, however, also noteworthy. The adoption of universal precautions is an important advance. Under universal precautions, it is assumed that all blood-containing fluid is potentially infectious and that appropriate safeguards should always be invoked. Safe disposal containers for needles and other sharp instruments are increasingly being placed in conveniently accessible locations in treatment areas, as illustrated in figure 2. The use of new devices, such as the needle-less access system for intravenous treatment and/or blood sampling has been shown to be a cost-effective method of reducing needlestick injuries (Yassi and McGill 1995).
Figure 2. Disposal container for sharp instruments and devices
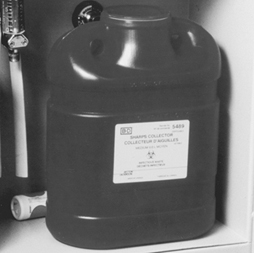
Health Sciences Centre, Winnipeg, Manitoba, Canada
Blood and body fluids are not the only source of infection for HCWs. Tuberculosis (TB) is also on the rise again in parts of the world where previously its spread had been curtailed and, as discussed later in this chapter, is a growing occupational health concern. In this, as in other nosocomial infections, such concern is heightened by the fact that so many of the organisms involved have become drug-resistant. There is also the problem of new outbreaks of deadly infectious agents, such as the Ebola virus. The article “Overview of infectious diseases” summarizes the major infectious disease risks for HCWs.
Chemical Hazards
HCWs are exposed to a wide variety of chemicals, including disinfectants, sterilants, laboratory reagents, drugs and anaesthetic agents, to name just a few of the categories. Figure 3 shows a storage cabinet in an area of a large hospital where prosthetics are fabricated and clearly illustrates the vast array of chemicals that are present in health care facilities. Some of these substances are highly irritating and may also be sensitizing. Some disinfectants and antiseptics also tend to be quite toxic, also with irritating and sensitizing propensities that may induce skin or respiratory tract disease. Some, like formaldehyde and ethylene oxide, are classified as mutagens, teratogens and human carcinogens as well. Prevention depends on the nature of the chemical, the maintenance of the apparatus in which it is used or applied, environmental controls, worker training and, in some instances, the availability of correct personal protective equipment. Often such control is straightforward and not very expensive. For example, Elias et al. (1993) showed how ethylene oxide exposure was controlled in one health care facility. Other articles in this chapter address chemical hazards and their management.
Figure 3. Storage cabinet for hazardous chemicals

Health Sciences Centre, Winnipeg, Manitoba, Canada
Physical Hazards and the Building Environment
In addition to the specific environmental contaminants faced by HCWs, many health care facilities also have documented indoor air quality problems. Tran et al. (1994), in studying symptoms experienced by operating room personnel, noted the presence of the “sick building syndrome” in one hospital. Building design and maintenance decisions are, therefore, extremely important in health care facilities. Particular attention must be paid to correct ventilation in specific areas such as laboratories, operating rooms and pharmacies, the availability of hoods and avoidance of the insertion of chemical-laden fumes into the general air-conditioning system. Controlling the recirculation of air and using special equipment (e.g., appropriate filters and ultraviolet lamps) is needed to prevent the transmission of air-borne infectious agents. Aspects of the construction and planning of health care facilities are discussed in the article “Buildings for health care facilities”.
Physical hazards are also ubiquitous in hospitals (see “Exposure to physical agents” in this chapter). The wide variety of electrical equipment used in hospitals can present an electrocution hazard to patients and staff if not properly maintained and grounded (see figure 4). Especially in hot and humid environments, heat exposure may present a problem to workers in such areas as laundries, kitchens and boiler rooms. Ionizing radiation is a special concern for staff in diagnostic radiology (i.e., x ray, angiography, dental radiography and computerized axial tomography (CAT) scans) as well as for those in therapeutic radiology. Controlling such radiation exposures is a routine matter in designated departments where there is careful supervision, well-trained technicians and properly shielded and maintained equipment, but it can be a problem when portable equipment is used in emergency rooms, intensive care units and operating rooms. It can also be a problem to housekeeping and other support staff whose duties take them into areas of potential exposure. In many jurisdictions these workers have not been properly trained to avoid this hazard. Exposure to ionizing radiation may also present a problem in diagnostic and therapeutic nuclear medicine units and in preparing and distributing doses of radioactive pharmaceuticals. In some cases, however, radiation exposure remains a serious problem (see the article “Occupational health and safety practice: The Russian experience” in this chapter).
Figure 4. Electrical equipment in hospital
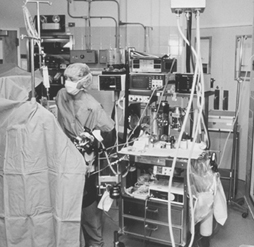
Health Sciences Centre, Winnipeg, Manitoba, Canada
Contradicting the prevailing impression of hospitals as quiet workplaces, Yassi et al. (1991) have documented the surprising extent of noise-induced hearing loss among hospital workers (see table 2). The article “Ergonomics of the physical work environment” in this chapter offers useful recommendations for controlling this hazard, as does table 3.
Table 2. 1995 integrated sound levels
|
Area monitored |
dBA (lex) Range |
|
Cast room |
76.32 to 81.9 |
|
Central energy |
82.4 to 110.4 |
|
Nutrition and food services (main kitchen) |
|
|
Housekeeping |
|
|
Laundry |
|
|
Linen service |
76.3 to 91.0 |
|
Mailroom |
|
|
Maintenance |
|
|
Materials handling |
|
|
Print shop |
|
|
Rehabilitation engineering |
|
Note: “Lex” means the equivalent sound level or the steady sound level in dBA which, if present in a workplace for 8 hours, would contain the same acoustic energy.
Table 3. Ergonomic noise reduction options
|
Work area |
Process |
Control options |
|
Central energy |
General area |
Enclose the source |
|
Dietetics |
Pot washer |
Automate process |
|
Housekeeping |
Burnishing |
Purchasing criteria |
|
Laundry |
Dryer/washer |
Isolate and reduce vibration |
|
Mailroom |
Tuberoom |
Purchasing criteria |
|
Maintenance |
Various equipment |
Purchasing criteria |
|
Materiel handling and |
Carts |
Maintenance |
|
Print shop |
Press operator |
Maintenance |
|
Rehabilitation |
Orthotics |
Purchasing criteria |
By far the most common and most costly type of injury faced by HCWs is back injury. Nurses and attendants are at greatest risk of musculoskeletal injuries due to the large amount of patient lifting and transferring that their jobs require. The epidemiology of back injury in nurses was summarized by Yassi et al. (1995a) with respect to one hospital. The pattern they observed mirrors those that have been universally reported. Hospitals are increasingly turning to preventive measures which may include staff training and the use of mechanical lifting devices. Many are also providing up-to-date diagnostic, therapeutic and rehabilitation health services that will minimize lost time and disability and are cost-effective (Yassi et al. 1995b). Hospital ergonomics has taken on increasing importance and, therefore, is the subject of a review article in this chapter. The specific problem of the prevention and management of back pain in nurses as one of the most important problems for this cohort of HCWs is also discussed in the article “Prevention and management of back pain in nurses” in this chapter. Table 4 lists the total number of injuries in a one-year period.
Table 4. Total number of injuries, mechanism of injury and nature of industry (one hospital, all departments), 1 April 1994 to 31 March 1995
|
Nature of injury sustained |
Total |
||||||||||||
|
Mechanism |
Blood/ |
Cut/ |
Bruise/ |
Sprain/ |
Fracture/ |
Burn/ |
Human |
Broken |
Head- |
Occupa- |
Other3 |
Un- |
|
|
Exertion |
|||||||||||||
|
Transferring |
105 |
105 |
|||||||||||
|
Lifting |
83 |
83 |
|||||||||||
|
Assisting |
4 |
4 |
|||||||||||
|
Turning |
27 |
27 |
|||||||||||
|
Breaking fall |
28 |
28 |
|||||||||||
|
Pushing |
1 |
25 |
26 |
||||||||||
|
Lifting |
1 |
52 |
1 |
54 |
|||||||||
|
Pulling |
14 |
14 |
|||||||||||
|
Combination- |
38 |
38 |
|||||||||||
|
Other |
74 |
74 |
|||||||||||
|
Fall |
3 |
45 |
67 |
3 |
1 |
119 |
|||||||
|
Struck/ |
66 |
76 |
5 |
2 |
2 |
1 |
152 |
||||||
|
Caught in/ |
13 |
68 |
8 |
1 |
1 |
91 |
|||||||
|
Exp. |
3 |
1 |
4 |
19 |
16 |
12 |
55 |
||||||
|
Staff abuse |
|||||||||||||
|
Patient |
16 |
11 |
51 |
28 |
8 |
3 |
1 |
2 |
120 |
||||
|
Spill/splashes |
80 |
1 |
81 |
||||||||||
|
Drug/ |
2 |
2 |
|||||||||||
|
Exp. |
5 |
5 |
10 |
||||||||||
|
Needlesticks |
159 |
22 |
181 |
||||||||||
|
Scalpel cuts |
34 |
14 |
48 |
||||||||||
|
Other5 |
3 |
1 |
29 |
1 |
6 |
40 |
|||||||
|
Unknown (no |
8 |
8 |
|||||||||||
|
Total |
289 |
136 |
243 |
558 |
5 |
33 |
8 |
7 |
19 |
25 |
29 |
8 |
1,360 |
1 No blood/body fluid. 2 This includes rashes/dermatitis/work-related illness/burning eyes, irritated eyes. 3 Exposure to chemical or physical agents but with no documented injuries affects. 4 Accident not reported. 5 Exposure to cold/heat, unknown.
In discussing musculoskeletal and ergonomic problems, it is important to note that while those engaged in direct patient care may be at greatest risk (see figure 5) many of the support personnel in hospital must contend with similar ergonomic burdens (see figure 6 and figure 7). The ergonomic problems facing hospital laundry workers have been well-documented (Wands and Yassi 1993) (see figure 8, figure 9 and figure 10) and they also are common among dentists, otologists, surgeons and especially microsurgeons, obstetricians, gynaecologists and other health personnel who often must work in awkward postures.
Figure 5. Patient lifting is an ergonomic hazard in most hospitals
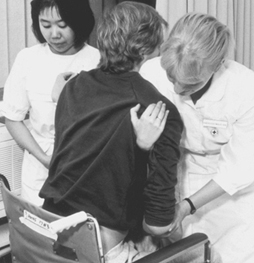
Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 6. Overhead painting: A typical ergonomic hazard for a tradesworker

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 7. Cast-making involves many ergonomic stresses

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 8. Laundry work such as this can cause repetitive stress injury to the upper limbs

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 9. This laundry task requires working in an awkward position

Health Sciences Centre, Winnipeg, Manitoba, Canada
Figure 10. A poorly designed laundry operation can cause back strain

Health Sciences Centre, Winnipeg, Manitoba, Canada
Organizational Problems
The article “Strain in health care work” contains a discussion of some of the organizational problems in hospitals and a summary of the principal findings of Leppanen and Olkinuora (1987), who reviewed Finnish and Swedish studies of stress among HCWs. With the rapid changes currently under way in this industry, the extent of alienation, frustration and burnout among HCWs is considerable. Added to that is the prevalence of staff abuse, an increasingly troublesome problem in many facilities (Yassi 1994). While it is often thought that the most difficult psychosocial problem faced by HCWs is dealing with death and dying, it is being recognized increasingly that the nature of the industry itself, with its hierarchical structure, its growing job insecurity and the high demands unsupported by adequate resources, is the cause of the variety of stress-related illness faced by HCWs.
The Nature of the Health Care Sector
In 1976, Stellman wrote, “If you ever wondered how people can manage to work with the sick and always stay healthy themselves, the answer is that they can’t” (Stellman 1976). The answer has not changed, but the potential hazards have clearly expanded from infectious diseases, back and other injuries, stress and burnout to include a large variety of potentially toxic environmental, physical and psychosocial exposures. The world of the HCW continues to be largely unmonitored and largely unregulated. None the less, progress is being made in addressing occupational health and safety hazards in hospitals. The International Commission on Occupational Health (ICOH) has a sub-committee addressing this problem, and several international conferences have been held with published proceedings that offer useful information (Hagberg et al. 1995). The US Centers for Disease Control and Prevention (CDC) and NIOSH have proposed guidelines to address many of the problems of the health care industry discussed in this article (e.g., see NIOSH 1988). The number of articles and books addressing health and safety issues for HCWs has been growing rapidly, and good overviews of health and safety in the US health care industry have been published (e.g., Charney 1994; Lewy 1990; Sterling 1994). The need for systematic data collection, study and analysis regarding hazards in the health care industry and the desirability of assembling interdisciplinary occupational health teams to address them have become increasingly evident.
When considering occupational health and safety in the health care industry, it is crucial to appreciate the enormous changes currently taking place in it. Health care “reform”, being instituted in most of the developed countries of the world, is creating extraordinary turbulence and uncertainty for HCWs, who are being asked to absorb rapid changes in their work tasks often with greater exposure to risks. The transformation of health care is spurred, in part, by advances in medical and scientific knowledge, the development of innovative technological procedures and the acquisition of new skills. It is also being driven, however, and perhaps to an even greater extent, by concepts of cost-effectiveness and organizational efficiency, in which “downsizing” and “cost control” have often seemed to become goals in themselves. New institutional incentives are being introduced at different organizational levels in different countries. The contracting out of jobs and services that had traditionally been carried out by a large stable workforce is now increasingly becoming the norm. Such contracting out of work is reported to have helped the health administrators and politicians achieve their long-term goal of making the process of health care more flexible and more accountable. These changes have also brought changes in roles that were previously rather well-defined, undermining the traditional hierarchical relationships among planners, administrators, physicians and other health professionals. The rise of investor-owned health care organizations in many countries has introduced a new dynamic in the financing and management of health services. In many situations, HCWs have been forced into new working relationships that involve such changes as downgrading services so that they can be performed by less-skilled workers at lower pay, reduced staffing levels, staff redeployments involving split shifts and part-time assignments. At the same time, there has been a slow but steady growth in the numbers of such physician surrogates as physician assistants, nurse practitioners, midwives and psychiatric social workers who command lower rates of pay than the physicians they are replacing. (The ultimate social and health costs both to HCWs and to the public, as patients and payers, is still to be determined.)
A growing trend in the US that is also emerging in the UK and northern European countries is “managed care”. This generally involves the creation of organizations paid on a per capita basis by insurance companies or government agencies to provide or contract for the provision of a comprehensive range of health services to a voluntarily-enrolled population of subscribers. Their aim is to reduce the costs of health care by “managing” the process: using administrative procedures and primary care physicians as “gatekeepers” to control the utilization of expensive in-patient hospital days, reducing referrals to high-priced specialists and use of costly diagnostic procedures, and denying coverage for expensive new forms of “experimental” treatment. The growing popularity of these managed care systems, fuelled by aggressive marketing to employer- and government-sponsored groups and individuals, has made it difficult for physicians and other health care providers to resist becoming involved. Once engaged, there is a variety of financial incentives and disincentives to influence their judgement and condition their behaviour. The loss of their traditional autonomy has been particularly painful for many medical practitioners and has had a profound influence on their patterns of practice and their relationships with other HCWs.
These rapid changes in the organization of the health care industry are having profound direct and indirect effects on the health and safety of HCWs. They affect the ways health services are organized, managed, delivered and paid for. They affect the ways HCWs are trained, assigned and supervised and the extent to which considerations of their health and safety are addressed. This should be kept in mind as the various occupational health hazards faced by HCWs are discussed in this chapter. Finally, although it may not appear to be directly relevant to the content of this chapter, thought should be given to the implications of the well-being and performance of HCWs to the quality and effectiveness of the services they provide to their patients.
Ethics in Health Protection and Health Promotion
While occupational health services are becoming more prevalent throughout the world, resources to develop and sustain these activities often do not keep pace with growing demands. Meanwhile, the boundaries of private and work life have been shifting, raising the issue of what can be, or should be, legitimately encompassed by occupational health. Workplace programmes that screen for drugs or HIV seropositivity, or provide counselling for personal problems, are obvious manifestations of the blurring of the boundary between private and work life.
From a public health viewpoint there are good arguments as to why health behaviours should not be compartmentalized into lifestyle factors, workplace factors and broader environmental factors. While the goals of eliminating drug abuse and other deleterious activities are laudable, there are ethical dangers in how these issues are addressed at the workplace. It will also be necessary to ensure that measures against such activities do not displace other health protection measures. The purpose of this article is specifically to examine the ethical issues in health protection and health promotion in the workplace.
Health Protection
Individual and collective protection of workers
While ethical behaviour is essential to all aspects of health care, the definition and promotion of ethical behaviour is often more complex in occupational health settings. The primary care clinician must prioritize the needs of the individual patient, and the community health professional must prioritize the health needs of the collective. The occupational health professional, on the other hand, has a duty to both the individual patient and the collective—the worker, the workforce and the public at large. Sometimes this multiple obligation presents conflicting responsibilities.
In most countries workers have an undeniable legal right to be protected from workplace hazards, and the focus of occupational health programmes should be precisely to address this right. Ethical issues associated with the protection of workers from unsafe conditions are generally those related to the fact that often the employer’s financial interests, or at least perceived financial interests, militate against undertaking the activities needed to protect workers’ health. The ethical stance that the occupational health professional must adopt, however, is clear-cut. As noted in the International Code of Ethics for Occupational Health Professionals (reprinted in this chapter): “Occupational health professionals must always act, as a matter of priority, in the interests of the health and safety of the workers.”
The occupational health professional, whether an employee or a consultant, often experiences pressures to compromise on ethical practice in worker health protection. The professional may even be asked by an employee to serve as an advocate against the organization when legal issues arise or when the employee, or the professional him- or herself, feels that health protection measures are not being provided.
To minimize such real-life conflicts it is necessary to establish societal expectations, market incentives and infrastructural mechanisms to counteract the employer’s real or perceived financial disadvantages in providing worker health protection measures. These may consist of clear regulations that require safe practices, with steep fines for violation of these standards; this, in turn, requires adequate compliance and enforcement infrastructure. It may also comprise a system of workers’ compensation premiums designed to promote prevention practices. Only when societal factors, norms, expectations and legislation reflect the importance of workplace health protection will ethical practice be truly allowed to flourish.
The right to be protected from unsafe conditions and acts of others
Occasionally, another ethical issue arises with respect to health protection: that is the situation in which an individual worker may him- or herself pose a workplace hazard. In keeping with the multiple responsibilities of the occupational health professional, the right of members of the collective (the workforce and the public) to be protected from the acts of others must always be considered. In many jurisdictions “fitness to work” is defined not only in terms of the worker’s ability to do the job, but also to do the job without posing an undue risk to co-workers or the public. It is unethical to deny someone a job (i.e., declare the worker unfit to work) on the basis of a health condition when no scientific evidence exists to substantiate the claim that this condition impairs the worker’s ability to work safely. However, sometimes clinical judgement suggests that a worker may pose a hazard to others, even when the scientific documentation to support a declaration of unfit is weak or even completely lacking. The repercussions, for example, of allowing a worker with undiagnosed dizzy spells to drive a crane, can be extremely serious. Indeed it may be unethical to allow an individual to assume special responsibilities in these cases.
The need to balance individual rights with collective rights is not unique to occupational health. In most jurisdictions it is legally required that a health practitioner report to the public health authorities conditions such as sexually transmitted diseases, tuberculosis or child abuse, even if this requires the breaching of confidentiality of the individuals involved. While there are often no concrete guidelines to assist the occupational health practitioner when formulating such opinions, ethical principles require that the practitioner utilize the scientific literature as thoroughly as possible in combination with his or her best professional judgement. Thus public health and safety considerations must be combined with concerns for the individual worker when performing medical and other exams for jobs with special responsibilities. Indeed screening for drugs and alcohol, if it is to be justified at all as a legitimate occupational health activity, could be justified only on this basis. The International Code of Ethics for Occupational Health Professionals states:
Where the health condition of the worker and the nature of the tasks performed are such as to be likely to endanger the safety of others, the worker must be clearly informed of the situation. In the case of a particularly hazardous situation, the management and, if so required by national regulations, the competent authority, must also be informed of the measures necessary to safeguard other persons.
The emphasis on the individual tends to overlook and indeed ignore the professional’s obligations to the overall good of society or even specific collective groups. For example, when the behaviour of the individual becomes a danger either to self or others, at what point should the professional act on behalf of the collective and override individual rights? Such decisions can have important ramifications for providers of employee assistance programmes (EAPs) who work with impaired workers. The duty to warn co-workers or clients who may use the impaired person’s services, as opposed to the obligation to protect the confidentiality of the person, has to be clearly understood. The professional cannot hide behind confidentiality or the protection of individual rights, as was discussed above.
Health Promotion Programmes
The assumptions and the debate
The assumptions generally underlying lifestyle change promotion activities in the workplace are that:
(l) employees’ daily lifestyle decisions regarding exercise, eating, smoking and stress management have a direct impact on their present and future health, the quality of their lives, and their job performance and (2) a company-sponsored positive lifestyle change programme, administered by full-time personnel but voluntary and open to all employees, will motivate employees to make positive lifestyle changes sufficient to affect both health and quality of life (Nathan 1985).
How far can the employer go in attempting to modify a behaviour such as off-hours drug use, or a condition such as overweight, which does not directly affect others or employee job performance. In health promotion activities, enterprises commit themselves to a role of reformer of those aspects of employees’ lifestyles that are, or are perceived to be, harmful to their health. In other words, the employer may wish to become an agent of social change. The employer may even strive to become the health inspector with regard to those conditions which are deemed to be favourable or unfavourable to health, and implement disciplinary action to keep employees in good health. Some have specific restrictions which prohibit employees from exceeding set body weights. Incentive measures are in place which reduce insurance or other benefits to employees who care for their bodies, especially through exercise. Policies may be used to encourage certain sub-groups, i.e., smokers, to give up practices that are harmful to their health.
Many organizations contend that they do not intend to direct the personal lives of employees, but rather are seeking to influence the workers to act sensibly. However, some question whether employers should intervene in an area that is recognized as private behaviour. Opponents argue that such activities are an abuse of employers’ power. What is rejected is less the legitimacy of the health proposals than the motivation behind them, which appears to be paternalistic and elitist. The health promotion programme may also be perceived to be hypocritical where the employer does not make changes to organizational factors that contribute to ill health, and where the principal motive appears to be cost containment.
Cost containment as the primary motivator
A central feature of the context of worksite-based health services is that the “main” business of the organization is not to provide health care, though services to employees may be seen as an important contribution to the achievement of the organization’s goals, such as efficient operation and cost containment. In most cases, health promotion EAPs and rehabilitation services are provided by employers seeking to meet organizational goals—i.e., a more productive work force, or the reduction of costs of insurance and workers’ compensation. While corporate rhetoric has emphasized the humanitarian motives underlying EAPs, the major rationale and impetus usually involves the organization’s concerns about the costs, absenteeism and loss of productivity associated with mental health problems and abuse of alcohol and drugs. These goals are substantially different from the traditional goals of health practitioners, since they take into consideration the goals of the organization as well as the needs of the patient.
When employers pay directly for the services, and services are provided at the worksite, professionals delivering services must, by necessity, take into account the organizational goals of the employer and the specific culture of the workplace involved. Programmes may be framed in terms of “bottom line impact”; and compromises on goals for health services may need to be made in the face of cost containment realities. The choice of action recommended by the professional may be influenced by these considerations, sometimes presenting an ethical dilemma as to how to balance what would be best for the individual worker with what would be most cost-effective for the organization. Where the professional’s primary responsibility is managed care with a stated goal of cost containment, conflicts may be exacerbated. Considerable caution must therefore be exercised in managed care approaches to ensure that health care objectives are not compromised by efforts to limit or reduce costs.
Which employees are entitled to EAP services, which types of problem should be considered and should the programme be extended to family members or retirees? It would appear that many decisions are based not on the stated intent of improved health but rather the limit of benefit coverage. Part-time staff who have no benefit coverage tend not to have access to EAP services so that the organization does not have to pay additional costs. However, part-time staff may also have problems which affect performance and productivity.
In the trade-off between quality care and lowered costs, who should decide how much quality is required and at what price—the patient, who uses the services but is not accountable for the payment or price, or the EAP gatekeeper, who does not pay the bill but whose job may depend upon the success of the treatment? Should the provider or the insurer, the ultimate payer, take the decision?
Similarly, who should decide when an employee is expendable? And, if insurance and treatment costs dictate such a decision, when is it more cost-efficient to fire an employee—for example, because of mental illness—and then recruit and train a new employee? More discussion of the role of occupational health professionals in addressing such decisions is certainly warranted.
Voluntarism or coercion?
The ethical problems created by unclear client allegiance are immediately evident in EAPs. Most EAP professionals would argue from their clinical training that their legitimate focus is the individual for whom they are the advocates. This concept depends on the notion of voluntarism. That is, the client seeks out assistance voluntarily and consents to the relationship, which is maintained only with his or her active participation. Even where the referral is made by a supervisor or management, the argument is made that participation is still fundamentally voluntary. Similar arguments are made for health promotion activities.
This contention of EAP practitioners that clients are operating on their own free will often falls apart in practice. The notion that participation is entirely voluntary is largely an illusion. Client perceptions of choice are sometimes much less than proclaimed, and supervisory referrals can well be based on confrontation and coercion. So are the majority of so-called self-referrals, which occur after a strong suggestion has been given by a powerful other. While the language is one of choice, it is clear that choices are indeed limited and there is only one right way to proceed.
When health care costs are paid by the employer or through the employer’s insurance, the boundaries between public and private life become less distinct, further increasing the potential for coercion. The current ideology of programmes is one of voluntarism; but can any activity be completely voluntary in the work setting?
Bureaucracies are not democracies and any so-called voluntary behaviour in organizational setting is likely to be open to challenge. Unlike the community setting, the employer has a fairly long term contractual relationship with most employees, which in many cases is dynamic with the possibility of raises, promotions, as well as overt and covert demotions. This may result in deliberate or inadvertent impressions that participation in a particular active preventive programme is normative and expected (Roman 1981).
Health education too must be cautious about claims of voluntarism as this fails to recognize the subtle forces which have great potency in the workplace on shaping behaviour. The fact that health promotion activities receive considerable positive publicity and are also provided free of cost, can lead to the perception that participation is not only supported but highly desired by management. There may be expectations of rewards for participation beyond those related to health. Participation may be seen as necessary to advancement or at least to maintaining one’s profile in the organization.
There may also be a subtle deception on the part of management, which promotes health activities as part of its sincere interest in the well-being of staff, while burying its real concerns related to cost containment expectations. Overt incentives such as higher insurance premiums for smokers or overweight employees may increase participation but at the same time be coercive.
Individual and collective risk factors
The overwhelming focus of work-based health promotion on individual lifestyle as the unit of intervention distorts the complexities underlying social behaviours. Social factors, such as racism, sexism and class bias, are generally overlooked by programmes which focus solely on changing personal habits. This approach takes behaviour out of context and assumes “that personal habits are discrete and independently modifiable, and that individuals can voluntarily choose to alter such behaviour” (Coriel, Levin and Jaco 1986).
Given the influence of social factors, what is the true extent to which people have control over modifying health risks? Certainly behavioural risk factors do exist, but the effects of social structure, the environment, heredity or simple chance must also be taken into account. The individual is not solely responsible for the development of disease, yet this is precisely what many work-site health promotion efforts assume.
A health promotion programme in which individual responsibility can be overstated, leads to moralizing.
Although personal responsibility is undeniably a factor in smoking for example, social influences such as class, stress, education and advertising are also involved. Deeming that only individual factors are causally responsible facilitates blaming the victim. Employees who smoke, are overweight, have high blood pressure, and so on, are blamed, albeit sometimes implicitly, for their condition. This absolves the organization and society from any responsibility for the problem. Employees may be blamed both for the condition and for not doing something about it.
The tendency to assign responsibility solely to the individual ignores a large body of scientific data. Evidence suggests that the physiological sequelae of work may have an impact on health which continues after the workday is done. It has been widely demonstrated that linkages between organizational factors (such as participation in decision making, social interaction and support, pace of work, work overload, etc.), and health outcomes, particularly cardiovascular disease, exist. Implications for organizational interventions, rather than or in addition to individual behaviour change, are quite clear. Nonetheless, most health promotion programmes aim to change individual behaviour but rarely consider such organizational factors.
The focus on individuals is less surprising when it is recognized that most professionals in health promotion, wellness and EAP programmes are clinicians who do not have a background in occupational health. Even when clinicians do identify workplace factors of concern, they are seldom equipped to recommend or carry out organizationally oriented interventions.
Diverting attention from health protection
Rarely have wellness programmes proposed interventions in the corporate culture or included alterations in work organization such as stressful management styles, the content of boring work or noise levels. By ignoring the contribution of the work environment to the health outcomes, popular programmes such as stress management may have a negative impact on health. For example, by focusing on individual stress reduction rather than altering stressful working conditions, workplace health promotion may be helping workers to adapt to unhealthy environments and in the long term increasing disease. Moreover, the research conducted has not provided much support for the clinical approaches. For example, in one study, individual stress management programmes had smaller effects on catecholamine production than did the manipulation of pay systems (Ganster et al. 1982).
In addition, Pearlin and Schooler (1978) found that while various problem-solving, coping responses were effective in one’s personal and family life, this type of coping is not effective in dealing with work-related stressors. Other studies further suggested that some personal coping behaviours actually increase distress if applied in the workplace (Parasuramen and Cleek 1984).
The advocates of wellness programmes are generally uninterested in the traditional concerns of occupational health and, consciously or otherwise, turn attention away from workplace hazards. As wellness programmes generally ignore the risk of occupational disease or hazardous working conditions, health protection advocates fear that individualizing the problem of employee health is an expedient way for some companies to deflect attention from costly but risk-reducing changes in the structure and content of workplace or jobs.
Confidentiality
Employers sometimes feel they have the right to have access to clinical information about workers who receive services from the professional. Yet the professional is bound by the ethics of the profession and by the practical need to maintain the trust of the worker. This problem becomes particularly troublesome if legal proceedings are at issue or if the problem at hand is surrounded by emotionally charged issues, such as disability from AIDS.
Professionals may also become involved in confidential issues related to the employer’s business practices and operations. If the industry in question is highly competitive, the employer may wish to keep secret such information as organizational plans, reorganizations and downsizing. Where business practices may have an impact on the health of employees, how does the professional prevent the occurrence of such adverse effects without jeopardizing the proprietary or competitive secrets of the organization?
Roman and Blum (1987) argue that confidentiality serves to protect the practitioner from extensive scrutiny. Citing client confidentiality, many oppose quality review or peer case review, which might reveal that the practitioner has exceeded the bounds of professional training or expertise. This is an important ethical consideration given the power of the counsellor to influence the health and well-being of clients. The issue is the need to clearly identify for the client the nature of the intervention in terms of what it can or cannot do.
The confidentiality of information collected by programmes which focus on individuals rather than systems of work may be prejudicial to the worker’s job security. Health promotion information can be misused to influence the employee’s status with health insurance or personnel issues. When aggregate data are available, it may be difficult to ensure that such data will not be used to identify individual employees, especially in small work groups.
Where the clinical utilization patterns of the EAP draw attention to a particular work unit or site, practitioners have been loath to bring this to management’s attention. Sometimes the citation of confidentiality issues in reality masks an inability to make reasonable recommendations for intervention due to fears that management will not be receptive to negative feedback about their behaviour or organizational practices. Unfortunately, clinicians sometimes lack the research and epidemiological skills which allow them to present solid data in support of their observations.
Other concerns relate to the misuse of information by a variety of different interest groups. Insurance companies, employers, trade unions, client groups and health professionals may misuse both collective and individual information gathered in the course of a health promotion activity.
Some may use data to deny services or coverage to employees or their survivors in legal or administrative proceedings dealing with compensation or insurance claims. Participants in programmes may believe that the “guarantee of confidentiality” provided by such programmes is inviolate. Programmes need to clearly advise employees that under certain circumstances (i.e., legal or administrative inquiries) personal information gathered by the programme may be made available to other parties.
Aggregate data may be misused so as to shift the burden from one party to another. Access to such information may not be equitable, in that collective information may be available only to organizational representatives and not those individuals seeking benefits. While releasing data on workers focusing on the individual lifestyle contributions to a condition, organizations may be able to restrict information about corporate practices which also created the problem.
Epidemiological data about patterns of conditions or work-related factors should not be gathered in such a manner as to facilitate exploitation by the employer, the insurer, the compensation system or by the clients.
Conflict with other professional or service standards
Professional standards and values may be in conflict with practices already in place in a given organization. Confrontational methods used by occupational alcoholism programmes may be unproductive or in conflict with professional values when dealing with other disorders or disabilities, yet the professional working in this context may be pressured to participate in the use of such methods.
Ethical relationships with outside providers must also be considered. While EAPs have clearly articulated the need for practitioners to avoid referrals to treatment services with which they are closely affiliated, health promotion providers have not been as resolute in defining their relationships with external providers of services that may be attractive to employees for personal lifestyle counselling. Arrangements between EAPs and particular providers which lead to referrals to treatment based on economic advantages to the providers rather than clinical needs of clients present an obvious conflict of interest.
There is also the temptation to engage unqualified individuals in health promotion. EAP practitioners do not normally have the training in health education techniques, physiology or fitness instruction to qualify them to provide such activities. When programmes are provided and administered by management and cost is of primary concern, there is less motivation to scrutinize skills and expertise and to invest in the best qualified professionals, as this will change the cost-benefit outcomes.
The use of peers to provide services raises other concerns. It has been shown that social support from one’s co-workers could buffer the health effects of certain job stressors. Many programmes have capitalized on the positive influence of social support by the use of peer counsellors or self-help support groups. However, while peers can be used as a supplement to some extent, they do not eliminate the need for qualified health professionals. Peers need to have a strong orientation programme, which includes content on ethical practices and not exceeding one’s personal limits or qualifications whether overtly or through misrepresentation.
Drug screening and testing
Drug testing has become a quagmire of regulations and legal interpretation and has not proven to be an effective avenue to either treatment or prevention. The recent report from the National Research Institute (O’Brien 1993) has concluded that drug testing is not a strong deterrent to alcohol and drug abuse. Further evidence suggests that it does not have a significant impact on work performance.
A positive drug test may reveal much about an employee’s lifestyle but nothing about his or her level of impairment or ability to perform work.
Drug testing has been seen as the thin edge of the wedge with which employers drive out all but the most invulnerable employee—the super-resilient person. The trouble is how far does the organization go? Can one test for compulsive behaviours such as gambling or for mental disorders, such as depression?
There is also a concern that organizations may use screening to identify undesirable traits (e.g., predisposition to heart disease or back injury) and to make personnel decisions based on this information. At present this practice appears to be limited to health insurance coverage, but how long can it be resisted by management attempting to reduce cost?
The government-stimulated practice of screening for drugs, and the future possibility of screening for defective genes and excluding whole classes of high-cost employees from health insurance coverage, advances the old presumption that characteristics of workers, not work, explain disabilities and dysfunctions; and this becomes a justification for making workers bear the social and economic costs. This leads again to a perspective in which factors based on the individual, not work, become the focus of health promotion activities.
Exploitation by the client
On occasion it may be clear to the professional that workers are attempting to take improper advantage of the system of services provided by an employer or by its insurance carrier or by workers’ compensation. Problems may include clearly unrealistic rehabilitation demands or outright malingering for financial gain. Appropriate methods of confronting such behaviour, and for taking action as needed, have to be balanced against other clinical realities, such as psychological reactions to disability.
Promotion of activities with questionable effectiveness
Despite the broad claims for worksite health promotion, the scientific data available to evaluate them are limited. The profession as a whole has not addressed the ethical issues of promoting activities which do not have a strong scientific support, or of choosing to engage in services which produce more revenue rather than focusing on ones which have a demonstrated impact.
Ironically, what is being sold is based upon little conclusive evidence of cost reduction, decreased absenteeism, reduced health care expenditures, reductions in employee turnover or increased productivity. Studies are poorly designed, seldom having comparison groups or long-term follow-up. The few that meet the standards of scientific rigour have provided little evidence of a positive return on investment.
There is also some evidence that the participants in worksite health promotion activities tend to be relatively healthy individuals:
Overall it appears participants are likely to be nonsmokers, more concerned with health matters, perceive themselves in better health, and be more interested in physical activities, especially aerobic exercise, than nonparticipants. There is also some evidence that participants may use less health services and be somewhat younger than nonparticipants (Conrad 1987).
Individuals at risk may not be using the health services.
Even where there is evidence to support particular activities and all of the professionals agree on the necessity for such services as follow-up, in practice services are not always provided. Generally EAPs concentrate on finding new cases while devoting little time to workplace prevention. Follow-up services are either non-existent or limited to one or two visits after return to work. With the chronic relapse potential of alcohol and drug cases, it would appear that EAPs are not devoting energies to continuing care, which is very costly to provide, but rather emphasize activities which generate new revenues.
Health examinations for insurance purposes and determination of benefits
Just as the boundary between private life and work factors affecting health has become increasingly blurred, so too has the distinction between fit and unfit or healthy and sick. Thus instead of examinations for insurance or benefits focusing on whether or not a worker is ill or disabled, and therefore “deserving” of benefits, there is an increasing realization that with workplace changes and health promotion activities, the worker, even with his or her illness or disability, can be accommodated. Indeed “adaptation of work to the capabilities of workers in the light of their state of physical and mental health” has been enshrined in the ILO Occupational Health Services Convention, 1985 (No. 161).
The linking of health protection measures and health promotion activities is nowhere as important as it is in addressing workers with special health needs. Just as an indexed patient may reflect pathology in a group, a worker with special health needs may reflect needs in the workforce as a whole. Alteration of the workplace to accommodate such workers very often results in improvements in the workplace that benefit all workers. Providing treatment and health promotion to workers with special health needs may decrease costs to the organization, by containing insurance or workers’ compensation benefits; more importantly, it is the ethical way to proceed.
In recognition that prompt rehabilitation and accommodation of injured workers is “good business,” many employers have introduced early intervention, rehabilitation and return to modified work programmes. Sometimes these programmes are offered through workers’ compensation boards, which have come to realize that both the employer and the individual worker suffer if the benefit system provides an incentive to maintain “the sick role,” rather than an incentive towards physical, mental and vocational rehabilitation.
Conclusion
The International Code of Ethics for Occupational Health Professionals (reprinted in this chapter) provides guidelines to ensure that health promotion activities do not divert attention from health protection measures, and to promote ethical practice in such activities. The Code states:
Occupational health professionals may contribute to public health in different ways, in particular by their activities in health education, health promotion and health screening. When engaging in these programmes, occupational health professionals must seek the participation ... of both employers and workers in their design and in their implementation. They must also protect the confidentiality of personal health data of the workers.
Finally, it is necessary to reiterate that the ethical practice of occupational health could best be promoted by addressing the workplace and societal infrastructure that must be designed to promote the interests of both the individual and the collective. Thus stress management, health promotion and EAPs, which until now have focused almost exclusively on individuals, must address institutional factors in the workplace. It will also be necessary to ensure that such activities do not displace health protection measures.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."