- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Waste Disposal Operations
Workers involved in municipal waste disposal and handling face occupational health and safety hazards which are as diverse as the materials they are handling. Workers’ primary complaints relate to odour and upper respiratory tract irritation usually related to dust. However, actual occupational health and safety concerns vary with the work process and the waste stream characteristics (mixed municipal solid waste (MSW), sanitary and biological waste, recycled wastes, agricultural and food wastes, ash, construction debris and industrial wastes). Biological agents such as bacteria, endotoxins and fungi may present hazards, particularly for immune system-compromised and hypersensitive workers. In addition to safety concerns, health impacts have involved predominantly respiratory health problems among workers, including symptoms of organic dust toxic syndrome (ODTS), irritation of the skin, eyes and upper airways and cases of more severe pulmonary diseases such as asthma, alveolitis and bronchitis.
The World Bank (Beede and Bloom 1995) estimates that 1.3 billion tonnes of MSW were generated in 1990 which represents an average of two-thirds of a kilogram per person per day. In the US alone, an estimated 343,000 workers were involved in MSW collection, transport and disposal according to 1991 US Census Bureau statistics. In industrialized countries waste streams are increasingly distinct and work processes are increasingly complex. Efforts to segregate and better define the compositions of waste streams are often critical for identifying occupational hazards and appropriate controls and for controlling environmental impacts. Most waste disposal workers continue to face unpredictable exposures and risks from mixed wastes in dispersed open dumps, often with open burning.
The economics of waste disposal, reuse and recycling, as well as public health concerns, are driving rapid changes in waste handling globally to maximize recovery of resources and reduce dispersion of refuse into the environment. Depending on local economic factors this results in the adoption of either increasingly labour-intensive or capital-intensive work processes. Labour-intensive practices draw an increasing number of workers into hazardous work environments and commonly involve informal sector scavengers who sort mixed refuse by hand and sell recyclable and reusable materials. Increased capitalization has not automatically led to improvements in working conditions as increased work within confined spaces (e.g., in drum composting operations or incinerators), and increased mechanical processing of wastes can result in increased exposure to both airborne contaminants and mechanical hazards, unless proper controls are implemented.
Waste Disposal Processes
A variety of waste disposal processes are used, and as waste collection, transportation and disposal costs increase to meet increasingly stringent environmental and community standards, an increasing diversity of processes can be cost-justified. These processes break down into four basic approaches which may be used in combination or in parallel for various waste streams. The four basic processes are dispersal (land or water dumping, evaporation), storage/isolation (sanitary and hazardous waste landfills), oxidation (incineration, composting) and reduction (hydrogenation, anaerobic digestion). These processes share some general occupational hazards associated with waste handling, but also involve work-process-specific occupational hazards.
General Occupational Hazards in Waste Handling
Regardless of the specific disposal process being utilized, simply processing MSW and other wastes involves common defined hazards (Colombi 1991; Desbaumes 1968; Malmros and Jonsson 1994; Malmros, Sigsgaard and Bach 1992; Maxey 1978; Mozzon, Brown and Smith 1987; Rahkonen, Ettala and Loikkanen 1987; Robazzi et al. 1994).
Unidentified, highly hazardous materials are often intermixed with normal waste. Pesticides, flammable solvents, paints, industrial chemicals, and biohazardous waste, may all be intermixed with household waste. This hazard can be handled primarily through segregation of the waste stream and in particular separation of industrial and household waste.
Odours and exposure to mixed volatile organic compounds (VOCs) can induce nausea but are typically well below American Conference of Governmental Industrial Hygenists (ACGIH) threshold limit values (TLVs), even within enclosed spaces (ACGIH 1989; Wilkins 1994). Control typically involves isolation of the process, as in sealed anaerobic digesters or drum composters, minimizing worker contact through daily soil cover or transfer station cleanup and controlling biological degradation processes, particularly minimizing anaerobic degradation by controlling moisture content and aeration.
Insect- and rodent-borne pathogens can be controlled through daily cover of waste with soil. Botros et al. (1989) reported that 19% of garbage workers in Cairo had antibodies to Rickettsia Typhi (from fleas) which causes human rickettsial disease.
Injection or blood contact with infectious waste, such as needles and blood soiled waste, is best controlled at the generator by segregation and sterilization of such waste prior to disposal and disposal in puncture resistant containers. Tetanus is also a real concern should skin damage occur. Up-to-date immunization is required.
Ingestion of Giardia sp. and other gastrointestinal pathogens can be controlled by minimizing handling, reducing hand-to-mouth contact (including tobacco use), supplying safe drinking water, providing toilet and clean up facilities for workers and maintaining appropriate temperature in composting operations in order to destroy pathogens prior to dry handling and bagging. Precautions are particularly appropriate for Giardia found in sewage sludge and disposable baby diapers in MSW, as well as for tape and round worms from poultry and slaughterhouse wastes.
Inhalation of airborne bacteria and fungi is of particular concern when mechanical processing increases (Lundholm and Rylander 1980) with compactors (Emery et al. 1992), macerators or shredders, aeration, bagging operations and when moisture content is allowed to drop. This results in increased respiratory disorders (Nersting et al. 1990), bronchial obstruction (Spinaci et al. 1981) and chronic bronchitis (Ducel et al. 1976). Although there are no formal guidelines, the Dutch Occupational Health Association (1989) recommended that total bacteria and fungal counts should be kept below 10,000 colony forming units per cubic metre (cfu/m3) and below 500 cfu/m3 for any single pathogenic organism (outdoor air levels are about 500 cfu/m3 for total bacteria, indoor air is typically less). These levels may be regularly exceeded in composting operations.
Biotoxins are formed by fungi and bacteria including endotoxins formed by gram-negative bacteria. Inhaling or ingesting an endotoxin, even after killing the bacteria which produced it, can cause fever and flu-like symptoms without infection. The Dutch Working Group on Research Methods in Biological Indoor Air Pollution recommends that airborne gram-negative bacteria be kept below 1000 cfu/m3 to avoid endotoxin effects. Bacteria and fungi can produce a variety of other potent toxins which may also present occupational hazards.
Heat exhaustion and heat stroke can be serious concerns particularly where safe drinking water is limited and where PPE is utilized in sites known to contain hazardous wastes. Simple PVC-Tyvek suits show a heat stress equivalent of adding 6 to 11°C (11 to 20°F) to the ambient wet bulb globe temperature (WBGT) index (Paull and Rosenthal 1987). When the WBGT exceeds 27.7°C (82°F) conditions are considered hazardous.
Skin damage or disease are common complaints in waste handling operations (Gellin and Zavon 1970). Direct skin damage from caustic ash and other irritating waste contaminants, combined with high exposures to pathogenic organisms, frequent skin lacerations and punctures and, typically, poor availability of washing facilities result in a high incidence of skin problems.
Wastes contain a variety of materials that can cause lacerations or punctures. These are of particular concern in labour intensive operations such as waste sorting for recycling or manual turning of MSW compost and where mechanical processes such as compacting, crushing or shredding can create projectiles. The most critical control measures are safety glasses and puncture and slash resistant footwear and gloves.
Vehicular-use hazards include both operator hazards such as rollover and engulfment hazards and collision hazards with workers on the ground. Any vehicle that works on unsound or irregular surfaces should be equipped with rollover cages that will support the vehicle and allow the operator to survive. Pedestrian and vehicular traffic should be separated to the extent possible into distinct traffic areas, particularly where visibility is limited such as during open burning, at night and in composting yards where dense ground fogs may develop in cold weather.
Reports of increased atopic bronchopulmonary reactions such as asthma (Sigsgaard, Bach and Malmros 1990) and skin reactions can occur in waste workers, particularly where organic dust exposure levels are high.
Process-specific Hazards
Dispersion
Dispersion includes dumping waste into bodies of water, evaporation into the air or dumping with no effort at containment. Ocean dumping of MSW and hazardous wastes is rapidly declining. However, an estimated 30 to 50% of MSW is not collected in the cities of developing countries (Cointreau-Levine 1994) and is commonly burned or dumped in canals and streets, where it presents a significant public health threat.
Evaporation, sometimes with active heating at low temperatures, is used as a cost-saving alternative to incinerators or kilns, especially for volatile liquid organic contaminants such as solvents or fuel which are mixed with non-combustible wastes such as soil. Workers may face confined-space entry hazards and explosive atmospheres, especially in maintenance operations. Such operations should incorporate appropriate air emissions controls.
Storage/isolation
Isolation involves a combination of remote locations and physical containment in increasingly secure landfills. Typical sanitary landfills involve excavation with earth moving equipment, dumping of waste, compaction and daily cover with soil or compost to reduce pest infestations, odours and dispersion. Clay or impervious plastic caps and/or liners may be installed to limit water infiltration and leachate into groundwater. Test wells may be used to evaluate off-site leachate migration and to allow monitoring of leachate within the landfill. Workers include heavy equipment operators, truck drivers, spotters who may be responsible for rejecting hazardous waste and directing vehicle traffic flows and informal sector scavengers who may sort the waste and remove recyclables.
In areas dependent on coal or wood for fuel, ash can constitute a significant portion of the waste. Quenching prior to dumping, or segregation into ash monofills, may be necessary to avoid fires. Ash can cause skin irritation and caustic burns. Fly ash presents a variety of health hazards including respiratory and mucosal irritation as well as acute respiratory distress (Shrivastava et al. 1994). Low density fly ash can also constitute an engulfment hazard and can be unstable under heavy equipment and in excavations.
In many nations waste disposal continues to consist of simple dumping with open burning, which may be combined with informal scavenging of reusable or recyclable components with value. These informal sector workers face serious safety and health hazards. It is estimated that in Manila, Philippines, 7,000 scavengers work at the MSW dump, 8,000 in Jakarta and 10,000 in Mexico City (Cointreau-Levine 1994). Because of the difficulties in controlling work practices in informal work, an important step in controlling these hazards is to move separation of recyclables and reusables into the formal waste collection process. This may be performed by the waste generators, including consumers or household workers, by collection/sorting workers (e.g., in Mexico City collection workers officially spend 10% of their time sorting waste for sale of recyclables, and in Bangkok 40% (Beede and Bloom 1995)) or in pre-disposal waste separation operations (e.g., magnetic separation of metallic waste).
Open burning exposes workers to a potentially toxic mix of degradation products as discussed below. Because open burning can be used by informal scavengers to assist in separating metal and glass from combustible waste, it may be necessary to recover materials with salvage value prior to dumping in order to eliminate such open burning.
As hazardous wastes are successfully segregated from the waste stream, risks of MSW workers are reduced while quantities handled by hazardous waste site workers increase. Highly secure hazardous waste treatment and disposal sites depend on detailed manifesting of waste composition, high levels of worker PPE, and extensive worker training to control hazards. Secure landfills have unique hazards including slip and fall hazards where excavations are lined with plastic or polymer gels to reduce migration of leachate, potentially serious dermatological problems, heat stress related to work for extended periods in impermeable suits and supplied air quality control. Heavy equipment operators, labourers and technicians depend largely on PPE to minimize their exposures.
Oxidation (incineration and composting)
Open burning, incineration and waste-derived fuel are the most obvious examples of oxidation. Where the moisture content is low enough and the combustible content is high enough, increasing effort is made to utilize the fuel value in MSW either through the generation of waste-derived fuel as compressed briquettes or by incorporating electrical cogeneration or steam plants into municipal waste incinerators. Such operations can involve high levels of dry dusts due to efforts to produce a fuel with consistent heat value. Residual ash must still be disposed of, usually in landfills.
MSW incinerators involve a variety of safety hazards (Knop 1975). Swedish MSW incinerator workers showed increased ischemic heart disease (Gustavsson 1989), while a study of US incinerator workers in Philadelphia, Pennsylvania, failed to show a correlation between health outcomes and exposure groups (Bresnitz et al. 1992). Somewhat elevated blood lead levels have been identified in incinerator workers, primarily related to exposures to electrostatic precipitator ash (Malkin et al. 1992).
Ash exposures (e.g., crystalline silica, radioisotopes, heavy metals) can be significant not only in incinerator operations, but also at landfills and lightweight concrete plants where ash is used as aggregate. Although crystalline silica and heavy metal content vary with the fuel, this may present serious silicosis risk. Schilling (1988) observed lung function and respiratory symptom effects in ash exposed workers, but no changes observable by x ray.
Thermal degradation on pyrolysis products resulting from incomplete oxidation of many waste products can pose significant health risks. These products can include hydrogen chloride, phosgene, dioxins and dibenzofurans from chlorinated wastes, such as polyvinyl chloride (PVC) plastics and solvents. Non-halogenated wastes also can produce hazardous degradation products, including polyaromatic hydrocarbons, acrolein, cyanide from wools and silk, isocyanates from polyurethane and organotin compounds from a variety of plastics. These complex mixtures of degradation products can vary tremendously with waste composition, feed rates, temperature and available oxygen during combustion. While these degradation products are a significant concern in open burning, exposures in MSW incinerator workers appear to be relatively low (Angerer et al. 1992).
In MSW and hazardous waste incinerators and rotary kilns, control of combustion parameters and the residence time for waste vapours and solids at high temperatures is critical in destruction of wastes while minimizing the generation of more hazardous degradation products. Workers are involved in incinerator operation, loading and waste transfer into the incinerator, waste delivery and unloading from trucks, equipment maintenance, housekeeping and ash and slag removal. While incinerator design can limit necessary manual labour and worker exposures, with less capital-intensive designs there may be significant worker exposures and a need for regular confined space entry (e.g., chipping for removal of slag from glass waste from incinerator grates).
Composting
In aerobic biological processes the temperature and speed of oxidation are lower than incineration, but it is nevertheless oxidation. Composting of agricultural and yard wastes, sewage sludge, MSW and food wastes is increasingly common in city-scale operations. Rapidly developing technologies for biological remediation of hazardous and industrial wastes often involve a sequence of aerobic and anaerobic digestion processes.
Composting usually occurs either in wind rows (long piles) or in large vessels which provide aeration and mixing. The objective of composting operations is to create a mix of waste with optimum ratios of carbon and nitrogen (30:1) and then maintain moisture at 40 to 60% by weight, greater than 5% oxygen and temperature levels 32 to 60oC so that aerobic bacteria and other organisms can grow (Cobb and Rosenfield 1991). Following separation of recyclables and hazardous wastes (which typically involves hand sorting), MSW is shredded to create more surface area for biological action. Shredding can produce high noise and dust levels and significant mechanical guarding concerns. Some operations use ganged hammer-mills to allow reduced front-end sorting.
In-vessel or drum composting operations are capital intensive but allow more effective odour and process control. Confined space entry is a significant hazard for maintenance workers as high levels of CO2 may be released causing oxygen deficiency. Lockout of equipment prior to maintenance is also critical as mechanisms include internal screw-drives and conveyors.
In less capital intensive wind row composting operations, waste is shredded and placed in long piles which are mechanically aerated through perforated pipes or simply by turning, either with front-end loaders or manually. Wind rows may be covered or roofed to facilitate maintenance of constant moisture content. Where specialized wind row turning equipment is used, chain mixing-flails rotate at high speed through the compost and should be well guarded from human contact. As these flails rotate through the wind row, they eject objects which can become dangerous projectiles. Operators must assure safe clearance distances around and behind the equipment.
Regular temperature measurements with probes allow monitoring the progress of composting and assure high enough temperatures to kill pathogens while allowing adequate survival of beneficial organisms. At moisture contents of 20 to 45% when the temperature exceeds 93oC there can also be a spontaneous combustion fire hazard (much like a silo fire). This is most likely to occur when piles exceed 4 m in height. Fires can be avoided by keeping pile heights below 3 m, and turning when the temperature exceeds 60°C. Facilities should provide water hydrants and adequate access between wind rows for control of fires.
Hazards in composting operations include vehicle and mechanical hazards resulting from tractors and trucks involved in turning wind-rows of waste to maintain aeration and moisture content. In cooler climates the elevated temperatures of compost can produce dense ground fogs in a work area occupied by heavy equipment operators and pedestrian workers. Compost workers report more nausea, headache and diarrhoea than their counterparts in a drinking water plant (Lundholm and Rylander 1980). Odour problems can occur as a result of poor control of the moisture and air required for the composting to progress. If anaerobic conditions are allowed to occur, hydrogen sulphide, amines and other odorous materials are generated. In addition to typical disposal worker concerns, composting involving actively growing organisms can raise MSW temperatures high enough to kill pathogens, but can also produce exposures to moulds and fungi and their spores and toxins, especially in compost bagging operations and where compost is allowed to dry. Several studies have evaluated airborne fungi, bacteria, endotoxins and other contaminants (Belin 1985; Clark, Rylander and Larsson 1983; Heida, Bartman and van der Zee 1975; Lacey et al. 1990; Millner et al. 1994; van der Werf 1996; Weber et al. 1993) in composting operations. There is some indication of increased respiratory disorders and hypersensitivity reactions in compost workers (Brown et al. 1995; Sigsgaard et al. 1994). Certainly bacterial and fungal respiratory infections (Kramer, Kurup and Fink 1989) are a concern for immune-suppressed workers such as those with AIDS and those receiving cancer chemotherapy.
Reduction (hydrogenation and anaerobic digestion)
Anaerobic digestion for sewage and agricultural waste involves closed tanks, often with rotating brush contacts if nutrients are dilute, which can pose serious confined space entry concerns for maintenance workers. Anaerobic digesters are also commonly used in many countries as methane generators which may be fuelled with agricultural, sanitary or food wastes. Methane collection from MSW landfills and burning or compression for use is now required in many countries when methane generation exceeds specified thresholds, but most landfills have inadequate moisture for anaerobic digestion to proceed efficiently. Hydrogen sulphide generation is also a common result of anaerobic digestion and can cause eye irritation and olfactory fatigue at low levels.
More recently, high temperature reduction/hydrogenation has become a treatment option for organic chemical wastes. This can involve smaller, and therefore potentially mobile, installations with less energy input than a high temperature incinerator because metallic catalysts allow hydrogenation to proceed at lower temperatures. Organic wastes can be converted into methane and used as fuel to continue the process. Critical worker safety concerns include explosive atmospheres and confined space entry for cleaning, sludge removal and maintenance, hazards of transporting and loading the liquid feed wastes and spill response.
Summary
As wastes are viewed as resources for recycling and reuse, waste processing increases, resulting in rapid change in the waste disposal industry globally. Occupational health and safety risks of waste disposal operations often go beyond obvious safety hazards to a variety of chronic and acute health concerns. These hazards are often faced with minimal PPE and inadequate sanitary and wash-up facilities. Industrial waste reduction and pollution prevention efforts are increasingly shifting recycling and reuse processes away from contracted or external waste disposal operations and into production work areas.
Top priorities in controlling occupational safety and health hazards in this rapidly changing industry sector should include:
- integrating informal sector work into the formal work process
- providing adequate toilet and wash-up facilities and safe drinking water
- eliminating open burning and waste dispersion into the environment
- segregating waste streams to facilitate characterization of wastes and identification of appropriate control measures and work practices
- minimizing mixed vehicular and pedestrian traffic in work areas
- following appropriate excavation practices for soil and waste characteristics
- anticipating and controlling hazards prior to entry into confined spaces
- minimizing respirable dust exposures in high dust operations
- using safety glasses and slash and puncture resistant shoes and gloves
- integrating occupational safety and health concerns when introducing process change plans, particularly during transitions from open dumping and landfills to more complex and potentially more hazardous enclosed operations such as composting, mechanical or manual separation for recycling, waste to energy operations or incinerators.
In this period of rapid change in the industry, significant improvements in worker health and safety can be made at low cost.
Wood Handling
Wood may arrive at a pulp mill woodyard in the form of raw logs or as chips from a lumber mill. Some pulp mill operations have on-site sawmills (often called “woodrooms”) which produce both marketable lumber and stock for the pulp mill. Sawmilling is discussed in detail in the chapter Lumber. This article discusses those elements of wood preparation which are specific to pulp mill operations.
The wood preparation area of a pulp mill has several basic functions: to receive and meter the wood supply to the pulping process at the rate demanded by the mill; to prepare the wood so that it meets the mill’s feed specifications for species, cleanliness and dimensions; and to collect any material rejected by the previous operations and send it to final disposal. Wood is converted into chips or logs suitable for pulping in a series of steps which may include debarking, sawing, chipping and screening.
Logs are debarked because bark contains little fibre, has a high extractives content, is dark, and often carries large quantities of grit. Debarking can be done hydraulically with high-pressure water jets, or mechanically by rubbing logs against each other or with metal cutting tools. Hydraulic debarkers may be used in coastal areas; however, the effluent generated is difficult to treat and contributes to water pollution.
Debarked logs may be sawn into short lengths (1 to 6 metres) for stone groundwood pulping or chipped for refiner mechanical or chemical pulping methods. Chippers tend to produce chips with a considerable size range, but pulping requires chips of very specific dimensions to ensure constant flow through refiners and uniform cooking in digesters. Chips are therefore passed over a series of screens whose function is to separate chips on the basis of length or thickness. Oversized chips are rechipped, while undersized chips are either used as waste fuel or are metered back into the chip flow.
The requirements of the particular pulping process and chip conditions will dictate the duration of chip storage (figure 1; note the different types of chips available for pulping). Depending on fibre supply and mill demand, a mill will maintain a 2 to 6 week unscreened chip inventory, usually in large outdoor chip piles. Chips may degrade through auto-oxidation and hydrolysis reactions or fungal attack of the wood components. In order to avoid contamination, short-term inventories (hours to days) of screened chips are stored in chip silos or bins. Chips for sulphite pulping may be stored outside for several months to allow volatilization of extractives which may cause problems in subsequent operations. Chips used in kraft mills where turpentine and tall oil are recovered as commercial products typically proceed directly to pulping.
Figure 1. Chip storage area with front end loaders

George Astrakianakis
Fibre Sources for Pulp and Paper
The basic structure of pulp and paper sheets is a felted mat of cellulose fibres held together by hydrogen bonds. Cellulose is a polysaccharide with 600 to 1,500 repeated sugar units. The fibres have high tensile strength, will absorb the additives used to modify pulp into paper and board products, and are supple, chemically stable and white. The purpose of pulping is to separate cellulose fibres from the other components of the fibre source. In the case of wood, these include hemicelluloses (with 15 to 90 repeated sugar units), lignins (highly polymerized and complex, mainly phenyl propane units; they act as the “glue” that cements the fibres together), extractives (fats, waxes, alcohols, phenols, aromatic acids, essential oils, oleoresins, stearols, alkaloids and pigments), and minerals and other inorganics. As shown in table 1, the relative proportions of these components vary according to the fibre source.
Table 1. Chemical constituents of pulp and paper fibre sources (%)
|
Softwoods |
Hardwoods |
Straw |
Bamboo |
Cotton |
|
|
Carbohydrates |
|||||
|
a-cellulose |
38–46 |
38–49 |
28–42 |
26–43 |
80–85 |
|
Hemicellulose |
23–31 |
20–40 |
23–38 |
15–26 |
nd |
|
Lignin |
22–34 |
16–30 |
12–21 |
20–32 |
nd |
|
Extractives |
1–5 |
2–8 |
1–2 |
0.2–5 |
nd |
|
Minerals and other |
|
|
|
|
|
nd = no data available.
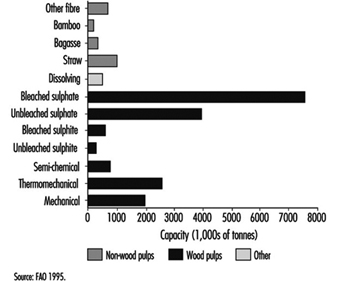
Coniferous and deciduous trees are the major fibre sources for pulp and paper. Secondary sources include straws from wheat, rye and rice; canes, such as bagasse; woody stalks from bamboo, flax and hemp; and seed, leaf or bast fibres, such as cotton, abaca and sisal. The majority of pulp is made from virgin fibre, but recycled paper accounts for an increasing proportion of production, up from 20% in 1970 to 33% in 1991. Wood-based production accounted for 88% of worldwide pulp capacity in 1994 (176 million tonnes, figure 1); therefore, the description of pulp and paper processes in the following article focuses on wood-based production. The basic principles apply to other fibres as well.
Figure 1. Worldwide pulp capacities, by pulp type
Municipal Recycling Industry
Overview
Recycling means different things to different people. To consumers, recycling may mean putting out bottles and cans for curbside collection. To a product maker—a manufacturer of raw materials or fabricator of goods—it means including recycled materials in the process. To recycling service providers, recycling can mean providing cost-efficient collection, sorting and shipping services. For scavengers, it means culling recyclable materials from garbage and waste cans and selling them to recycling depots. To public policy makers in all levels of government, it means establishing regulations governing collection and utilization as well as reducing the volume of waste to be disposed of and deriving revenue from the sale of the recycled materials. For recycling to work effectively and safely, these diverse groups must be educated to work together and share responsibility for its success.
The recycling industry had been growing steadily since its inception a century ago. Until the 1970s, it remained basically unchanged as a voluntary private sector effort conducted largely by scrap dealers. With the advent of incineration in the 1970s, it became desirable to separate out certain materials before putting waste into the furnaces. This concept was introduced to address the emission problems created by metals, batteries, plastics and other materials discarded in urban wastes which were causing many old incinerators to be shut down as environmental polluters. The increasing concern about the environment provided the primary impetus for the organized separation of plastics, aluminium, tin, paper and cardboard from the residential waste stream. Initially, the recycling industry was not economically viable as a self-sustaining business, but by the mid 1980s, the need for the materials and the increase in their prices led to the development of many new material recycling facilities (MRFs) to handle commingled recyclable materials across the US and Europe.
Work Force
The broad range of skills and expertise makes the range of employment for a MRF very wide. Whether it is a full-service MRF or a single sorting-line operation, the following groups of workers are generally employed:
- Operators of heavy equipment (front end loaders, grapples, bull-dozers, etc.) work on the tipping floor, coordinating the movement of waste from the staging area of the tipping floor to the area where the materials are sorted.
- Material sorters, the majority of the workforce, segregate and sort recyclable materials by product and/or colour. This may be done entirely by hand or with the assistance of equipment. The sorted materials are then baled or crated.
- Forklift operators are responsible for moving finished bales from the throat of the baler to the storage area and from there to the trucks or other means of transportation.
- Maintenance workers are becoming increasingly important as the technology advances and the machines and equipment become more complicated.
Processes and Facilities
The recycling industry has been growing very rapidly and has evolved many different processes and procedures as the technology of sorting recyclable materials has advanced. The most common types of installation include full-service MRFs, non-waste stream MRFs and simple sorting and processing systems.
Full-service MRFs
The full-service MRF receives recyclable materials mixed in the residential waste streams. Typically, the resident places the recyclables in coloured plastic bags which are then placed in the residential waste container. This allows the community to combine recyclable materials with other residential wastes, eliminating the need for separate collection vehicles and containers. A typical sequence of operations includes the following procedures:
- The waste and recyclables bags are dropped from the collection vehicle onto the tipping/collection floor.
- The mixture of waste and recyclables is moved either by a grapple or a front-end loader to an in-floor conveyer.
- The conveyer moves the material into the sorting area where a rotating trommel (a cylindrical sieve) opens the bags and allows the very small particles of dirt, sand and gravel to pass through the openings to a collection container for discarding.
- The remaining materials are semi-automatically sorted by screens or disks according to weight and bulkiness. Glass is sorted by its heavier weight, plastics by their lighter weight and paper fibre materials by their bulk.
- Employees hand sort materials, typically from an elevated position above bunkers into which the materials can be stored. Materials are sorted according to the grade of paper, the colour of glass, the physical properties of plastic and so on.
- Refuse and other wastes are collected and removed by tractor-trailer loads.
- The separated materials are moved from the bunkers by forklift or by a “walking floor” (i.e., a conveyer) to a baler or a shredding and baling operation.
- The formed bale is discharged from the baler and moved to the storage area by a forklift.
- Collected bales are shipped either by rail or a tractor-trailer. Instead of baling, some MRFs loose load the materials into a rail car or a tractor trailer.
Non-waste stream MRF
In this system, only the recyclables are delivered to the MRF; the residential wastes go elsewhere. It involves an advanced, semi-automated sorting and processing process system in which all of the steps are the same as those described above. Because of the smaller volume, fewer employees are involved.
Simple sorting/processing system
This is a labour-intensive system in which the sorting is performed manually. Typically, a conveyer belt is used to move material from one work station to another with each sorter removing one type of material as the belt passes his station. A typical sequence for such a simple, inexpensive processing system would include these processes:
- Mixed recyclables are received on a tipping floor and are moved by a front-end loader to the main sorting conveyor belt.
- Glass bottles are separated manually by colour (flint, amber, green and so forth).
- Plastic containers are sorted by grade and accumulated for baling.
- Aluminium cans are removed manually and fed to either a compactor or baler.
- The remaining materials are discharged into a residue pile or container for disposal.
Equipment and machinery
The machinery and equipment used in a MRF is determined by the type of process and the volumes of materials handled. In a typical semi-automated MRF, it would include:
- bag openers
- magnetic separators
- screens (disks, shakers or trommel)
- material classification equipment (mechanical or pneumatic)
- glass crushers
- balers and compactors
- eddy current separators (for non-ferrous metal separation)
- conveyer belts
- rolling stock.
Health and safety hazards
MRF workers face a large variety of environmental and work hazards, many of which are unpredictable since the content of the waste changes continually. Prominent among them are:
- infectious disease from biological and medical wastes
- acute and chronic toxicity from household chemicals, solvents and other chemicals being discarded. This risk is not very great (except when industrial wastes find their way into the residential stream) since household chemicals are usually not very toxic and only relatively small amounts are present.
- solvents and fuel and exhaust fumes (especially vehicle operators and maintenance workers)
- exposures to heat, cold and bad weather since many MRFs are exposed to the elements
- noise at harmful levels when heavy machines operate in confined spaces
- physical hazards such as slips and falls, puncture wounds, lacerations and abrasions, muscular strains, sprains and repetitive motion injuries. Sorters usually stand continuously, while vehicle operators must sometimes contend with poorly designed seats and operating controls.
- airborne dust and particles.
Table 1 lists the most common types of injury in the recycling industry.
Table 1. Most frequent injuries in the recycling industry.
|
Injury type |
Cause of injury |
Body part affected |
|
Cuts, abrasions and lacerations |
Contact with sharp materials |
Hands and forearms |
|
Strain |
Lifting |
Lower back |
|
Particles in eye |
Airborne dust and flying objects |
Eye |
|
Repetitive motion |
Manual sorting |
Upper extremities |
Prevention
MRF workers have the potential to be exposed to whatever wastes are delivered to it, as well as the ever-changing environment in which they work. The management of the facility must constantly be aware of the content of the material being delivered, the training and supervision of the workers and their compliance with safety rules and regulations, the proper use of PPE and the maintenance of machinery and equipment. The following safety considerations deserve constant close attention:
- lockout/tagout precautions
- general housekeeping
- egress maintenance
- emergency preparedness and, when needed, access to first-aid and medical assistance
- hearing conservation programmes
- protection against blood-borne pathogens
- preventive maintenance of machines and equipment
- traffic patterns and danger to pedestrians from the rolling stock
- confined spaces
- fire prevention and training and equipment for fire-fighting
- household hazardous waste management
- availability and use of high-quality, properly-sized PPE.
Conclusion
Municipal recycling is a relatively new industry that is changing rapidly as it grows and its technology advances. The health and safety of its workforce depend on proper design of processes and equipment and the proper training and supervision of its workers.
General Profile
Evolution and Structure of the Industry
Papermaking is thought to have originated in China in about 100 A.D. using rags, hemp and grasses as the raw material, and beating against stone mortars as the original fibre separation process. Although mechanization increased over the intervening years, batch production methods and agricultural fibre sources remained in use until the 1800s. Continuous papermaking machines were patented at the turn of that century. Methods for pulping wood, a more abundant fibre source than rags and grasses, were developed between 1844 and 1884, and included mechanical abrasion as well as the soda, sulphite, and sulphate (kraft) chemical methods. These changes initiated the modern pulp and paper manufacturing era.
Figure 1 illustrates the major pulp and paper making processes in the current era: mechanical pulping; chemical pulping; repulping waste paper; papermaking; and converting. The industry today can be divided into two main sectors according to the types of products manufactured. Pulp is generally manufactured in large mills in the same regions as the fibre harvest (i.e., mainly forest regions). Most of these mills also manufacture paper - for example, newsprint, writing, printing or tissue papers; or they may manufacture paperboards. (Figure 2 shows such a mill, which produces bleached kraft pulp, thermomechanical pulp and newsprint. Note the rail yard and dock for shipping, chip storage area, chip conveyors leading to digester, recovery boiler (tall white building) and effluent clarifying ponds). Separate converting operations are usually situated close to consumer markets and use market pulp or paper to manufacture bags, paperboards, containers, tissues, wrapping papers, decorative materials, business products and so on.
Figure 1. Illustration of process flow in pulp and paper manufacturing operations
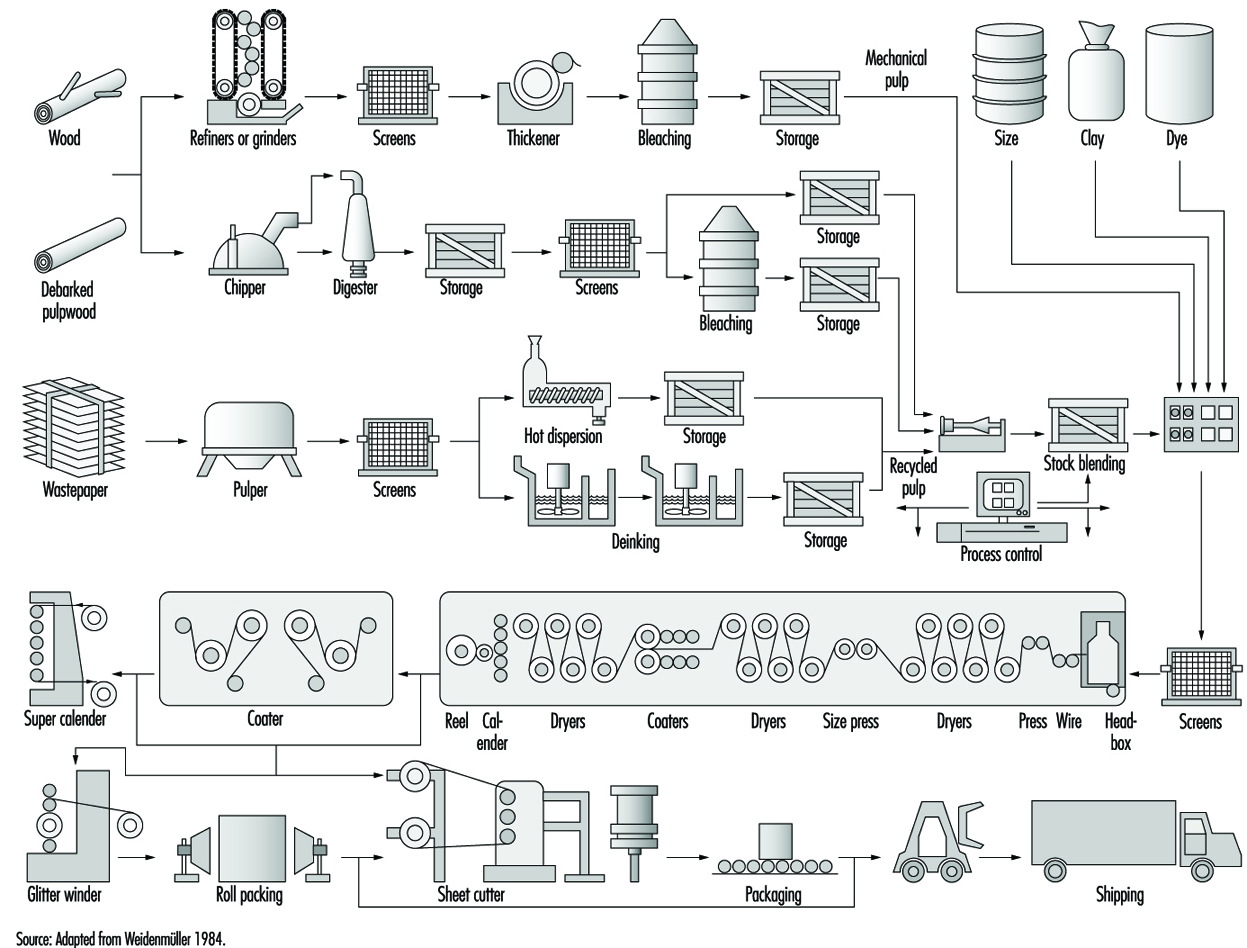
Figure 2. Modern pulp and paper mill complex situated on a coastal waterway

Canfor Library
There has been a trend in recent years for pulp and paper operations to become part of large, integrated forest product companies. These companies have control of forest harvesting operations (see the Forestry chapter), lumber milling (see the Lumber industry chapter), pulp and paper manufacturing, as well as converting operations. This structure ensures that the company has an ongoing source of fibre, efficient use of wood waste and assured buyers, which often leads to increased market share. Integration has been operating in tandem with increasing concentration of the industry into fewer companies and increasing globalization as companies pursue international investments. The financial burden of plant development in this industry has encouraged these trends to allow economies of scale. Some companies have now reached production levels of 10 million tonnes, similar to the output of countries with the highest production. Many companies are multinational, some with plants in 20 or more countries worldwide. However, even though many of the smaller mills and companies are disappearing, the industry still has hundreds of participants. As an illustration, the top 150 companies account for two-thirds of pulp and paper output and only one-third of the industry’s employees.
Economic Importance
The manufacture of pulp, paper and paper products ranks among the world’s largest industries. Mills are found in more than 100 countries in every region of the world, and directly employ more than 3.5 million people. The major pulp and paper producing nations include the United States, Canada, Japan, China, Finland, Sweden, Germany, Brazil and France (each produced more than 10 million tonnes in 1994; see table 1).
Table 1. Employment and production in pulp, paper, and paperboard operations in 1994, selected countries.
|
|
Number |
|
|
||
|
Number |
Production (1,000 |
Number |
Production (1,000 tonnes) |
||
|
Austria |
10,000 |
11 |
1,595 |
28 |
3,603 |
|
Bangladesh |
15,000 |
7 |
84 |
17 |
160 |
|
Brazil |
70,000 |
35 |
6,106 |
182 |
5,698 |
|
Canada |
64,000 |
39 |
24,547 |
117 |
18,316 |
|
China |
1,500,000 |
8,000 |
17,054 |
10,000 |
21,354 |
|
Czech Republic |
18,000 |
9 |
516 |
32 |
662 |
|
Finland |
37,000 |
43 |
9,962 |
44 |
10,910 |
|
Former USSR** |
|
|
|
|
|
|
France |
48,000 |
20 |
2,787 |
146 |
8,678 |
|
Germany |
48,000 |
19 |
1,934 |
222 |
14,458 |
|
India |
300,000 |
245 |
1,400 |
380 |
2,300 |
|
Italy |
26,000 |
19 |
535 |
295 |
6,689 |
|
Japan |
55,000 |
49 |
10,579 |
442 |
28,527 |
|
Korea, |
|
|
|
|
|
|
Mexico |
26,000 |
10 |
276 |
59 |
2,860 |
|
Pakistan |
65,000 |
2 |
138 |
68 |
235 |
|
Poland** |
46,000 |
5 |
893 |
27 |
1,343 |
|
Romania |
25,000 |
17 |
202 |
15 |
288 |
|
Slovakia |
14,000 |
3 |
304 |
6 |
422 |
|
South Africa |
19,000 |
9 |
2,165 |
20 |
1,684 |
|
Spain |
20,180 |
21 |
626 |
141 |
5,528 |
|
Sweden |
32,000 |
49 |
10,867 |
50 |
9,354 |
|
Taiwan |
18,000 |
2 |
326 |
156 |
4,199 |
|
Thailand |
12,000 |
3 |
240 |
45 |
1,664 |
|
Turkey |
12,000 |
11 |
416 |
34 |
1,102 |
|
United |
|
|
|
|
|
|
United States |
230,000 |
190 |
58,724 |
534 |
80,656 |
|
Total |
|
|
|
|
|
* Countries included if more than 10,000 people were employed in the industry.
** Data for 1989/90 (ILO 1992).
Source: Data for table adapted from PPI 1995.
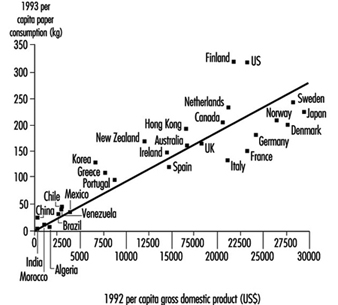
Every country is a consumer. Worldwide production of pulp, paper and paperboard was about 400 million tonnes in 1993. Despite predictions of decreased paper use in the face of the electronic age, there has been a fairly steady 2.5% annual rate of growth in production since 1980 (figure 3). In addition to its economic benefits, the consumption of paper has cultural value resulting from its function in the recording and dissemination of information. Because of this, pulp and paper consumption rates have been used as an indicator of a nation’s socioeconomic development (figure 4).
Figure 3. Pulp and paper production worldwide, 1980 to 1993
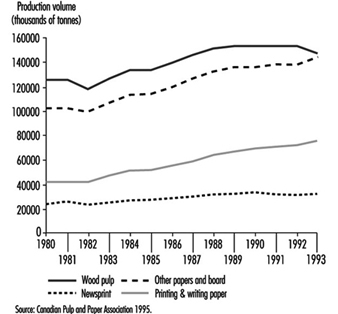
Figure 4. Paper and paperboard consumption as an indicator of economic development
The main source of fibre for pulp production over the last century has been wood from temperate coniferous forests, though more recently the use of tropical and boreal woods has been increasing (see the chapter Lumber for data on industrial roundwood harvesting worldwide). Because forested regions of the world are generally sparsely populated, there tends to be a dichotomy between the producing and using areas of the world. Pressure from environmental groups to preserve forest resources by using recycled paper stocks, agricultural crops and short-rotation plantation forests as fibre sources may change the distribution of pulp and paper production facilities throughout the world over the coming decades. Other forces, including increased paper consumption in the developing world and globalization, are also expected to play a role in relocating the industry.
Characteristics of the Workforce
Table 1 indicates the size of the workforce directly employed in pulp and paper production and converting operations in 27 countries, which together represent about 85% of world pulp and paper employment and over 90% of mills and production. In countries which consume most of what they produce (e.g., United States, Germany, France), converting operations provide two jobs for every one in pulp and paper production.
The labour force in the pulp and paper industry mainly holds full-time jobs within traditional management structures, though some mills in Finland, the United States and elsewhere have had success with flexible working hours and self-managed job-rotation teams. Because of their high capital costs, most pulping operations run continuously and require shift work; this is not true of converting plants. Working hours vary with the patterns of employment prevalent in each country, with a range from about 1,500 to more than 2,000 hours per year. In 1991, incomes in the industry ranged from US$1,300 (unskilled workers in Kenya) to US$70,000 per year (skilled production personnel in the United States) (ILO 1992). Male workers predominate in this industry, with women usually representing only 10 to 20% of the labour force. China and India may form the upper and lower ends of the range with 35% and 5% women respectively.
Management and engineering personnel at pulp and paper mills usually have university-level training. In European countries, most of the skilled blue-collar workforce (e.g., papermakers) and many of the unskilled workforce have had several years of trade-school education. In Japan, formal in-house training and upgrading is the norm; this approach is being adopted by some Latin American and North American companies. However, in many operations in North America and in the developing world, informal on-the-job training is more common for blue-collar jobs. Surveys have shown that, in some operations, many workers have literacy problems and are poorly prepared for the life-long learning required in the dynamic and potentially hazardous environment of this industry.
The capital costs of building modern pulp and paper plants are extremely high (e.g., a bleached kraft mill employing 750 people might cost US$1.5 billion to build; a chemi-thermomechanical pulp (CTMP) mill employing 100 people might cost US$400 million), so there are great economies of scale with high-capacity facilities. New and refitted plants usually use mechanized and continuous processes, as well as electronic monitors and computer controls. They require relatively few employees per unit production (e.g., 1 to 1.2 working hours per tonne of pulp in new Indonesian, Finnish and Chilean mills). Over the last 10 to 20 years, output per employee has increased as a result of incremental advances in technology. The newer equipment allows easier change-overs between product runs, lower inventories and customer-driven just-in-time production. Productivity gains have resulted in job losses in many producing nations in the developed world. However, there have been increases in employment in developing countries, where new mills being constructed, even if sparsely staffed, represent new forays into the industry.
From the 1970s to 1990, there was a decline of about 10% in the proportion of blue-collar jobs in European and North American operations, so that they now represent between 70 and 80% of the workforce (ILO 1992). The use of contract labour for mill construction, maintenance and wood-harvesting operations has been increasing; many operations have reported that 10 to 15% of their on-site workforce are contractors.
Street Cleaning
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Prevention of dirt-borne disease, prevention of damage to vehicles by harmful objects and the joy of viewing a neat, attractive city are all benefits derived from clean streets. Herded animals or animal-drawn vehicles, which in earlier times caused unsanitary conditions, have generally ceased to be a problem; however, the expansion in world population with the resultant upsurge in waste generated, the increase in the number and size of factories, the growth in the number of vehicles and newspapers and the introduction of disposable containers and products have all contributed to the amount of street refuse and added to the street-cleaning problem.
Organization and Processes
Municipal authorities recognizing the threat to health posed by dirty streets have sought to minimise the danger by organizing street cleaning sections in the public works departments. In these sections, a superintendent responsible for scheduling frequency of cleaning various districts will have forepeople responsible for specific cleaning operations.
Normally, business districts will be swept daily while arterial roads and residential areas will be swept weekly. Frequency will depend upon rain or snowfall, topography and the education of the populace toward prevention of litter.
The superintendent will also decide the most effective means of achieving clean streets. These could be hand sweeping by one worker or a group, hose flushing or machine sweeping or flushing. Generally a combination of methods, depending on the availability of equipment, type of dirt encountered and other factors will be used. In areas of heavy snowfall, special snow-clearing equipment may be used on occasion.
Hand sweeping is generally done in the daytime and confined to cleaning of gutters or spot cleaning of pavements or adjacent areas. The equipment used consists of brooms, scrapers and shovels. One sweeper generally patrols a specified route and cleans about 9 km of curb per shift under favourable conditions; however, this may be reduced in congested business districts.
Dirt collected by one-person sweeping is placed in a cart which he or she pushes ahead and dumps in boxes placed at intervals along his or her route; these boxes are emptied periodically into refuse trucks. In group sweeping, dirt is swept into piles along the gutters and loaded directly into trucks. Normally a group of 8 sweepers will have 2 workers assigned as loaders. Group sweeping is particularly effective for massive clean-up jobs such as after storms, parades or other special events.
Advantages of hand sweeping are: it is easily adjusted to meet changing cleaning loads; it can be used in areas inaccessible to machines; it can be conducted in heavy traffic with minimum interference with vehicle movement; it can be done in freezing weather and it can be used on pavements where surface conditions do not permit machine cleaning. Disadvantages are: the work is dangerous in traffic; it raises dust; dirt piled in gutters may be dispersed by wind or traffic if not collected promptly; and hand sweeping may be costly in labour-expensive areas.
Hose flushing is not considered an economical operation today; however, it is effective where there is a large amount of dirt or mud adhering to the pavement surfaces, where there are large numbers of parked vehicles or in market areas. It is generally done at night by a two-person crew, one of whom handles the hose nozzle and directs the stream and the other connects hose to the hydrant. Equipment consists of hoses, hose nozzles and hydrant wrenches.
Machine sweepers consist of motorized chassis mounted with brushes, conveyors, sprinklers and storage bins. They are generally used in late evening or early morning hours in business districts and during the day in residential areas. Cleaning action is confined to the gutters and adjacent areas where most dirt accumulates.
The machine is operated by one worker and can be expected to clean approximately 36 km of curb during an 8 hour shift. Factors affecting output are: number of times and distance which must be travelled to dump dirt or pick up sprinkling water; traffic density; and amount of dirt collected.
The advantages of machine sweepers are: they clean well, rapidly and raise no dust when sprinklers are used; they pick up the dirt as they clean; they can be used at night; and they are relatively economical. The disadvantages are: they cannot clean under parked cars or in off-pavement areas; they are not effective on rough, wet or muddy streets; the sprinkler cannot be used in freezing weather and dry sweeping raises dust; and they require skilled operators and maintenance personnel.
Flushing machines are essentially water tanks mounted on a motorized chassis which is fitted with a pump and nozzle to provide pressure and direct the stream of water against the pavement surface. The machine can be expected to clean about 36 km of 7 m wide pavement during an 8 hour shift.
The advantages of flushing machines are: they can be used effectively on wet or muddy pavements; they clean rapidly, well and under parked cars without raising dust; and they can operate at night or in light traffic. The disadvantages are: they require additional cleaning to be effective where street, litter or sewer conditions are not favourable; they annoy pedestrians or vehicle operators who are splashed; they cannot be used in freezing weather; and they require skilled operators and maintenance personnel.
Hazards and Their Prevention
Street cleaning is a hazardous occupation due to the fact that it is conducted in traffic and is concerned with dirt and refuse, with the possibility of infection, cuts from broken glass, tins and so on. In crowded areas, hand sweepers may be exposed to a considerable amount of carbon monoxide and to a high level of noise.
Traffic hazards are protected against by training sweepers in ways of avoiding danger, such as arranging work against the traffic flow and providing them with highly visible clothing as well as attaching red flags or other warning devices to their carts. Machine sweepers and flushers are made visible by fitting them with flashing lights, waving flags and painting them distinctively.
Street cleaners, and in particular hand sweepers, are exposed to all the vagaries of weather and occasionally may have to work in very severe conditions. Illness, infection and handling accidents can in part be prevented by the use of PPE and in part by training. Mechanical equipment such as that used for snow cleaning should be operated only by trained workers.
There should be a conveniently accessible central point providing good washing facilities (including showers where practicable), a cloakroom with arrangements for changing and drying clothes, a messroom and a first-aid room. Periodical medical examination is desirable.
Environmental Concerns of Snow Disposal
Snow removal and disposal introduces a set of environmental concerns related to the potential deposition of debris, salts, oil, metals and particulates in local waterbodies. A particular danger exists from the concentration of particulates, such as lead, that originate in atmospheric emissions from industrialized areas and automobiles. The danger of melt-water runoff to aquatic organisms and the risk of soil and groundwater contamination has been countered by the adoption of safe handling practices that protect sensitive areas from exposure. Snow disposal guidelines have been adopted in several Canadian provinces (e.g., Quebec, Ontario, Manitoba).
Sewage Treatment
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Waste water is treated in order to remove pollutants and to comply with the limits set by law. For this purpose an attempt is made to render the pollutants in the water insoluble in the form of solids (e.g., sludge), liquids (e.g., oil) or gases (e.g., nitrogen) by applying appropriate treatments. Well known techniques are then used to separate the treated waste water to be returned to the natural waterways from the pollutants rendered insoluble. The gases are dispersed into the atmosphere, while the liquid and solid residues (sludge, oil, grease) are usually digested before being submitted to further treatment. There may be single or multi-stage treatments according to the characteristics of the waste water and to the degree of purification required. Waste water treatment may be subdivided into physical (primary), biological (secondary) and tertiary processes.
Physical Processes
The various physical treatment processes are designed to remove insoluble pollutants.
Screening
The sewage is made to pass through screens which retain coarse solids that may block or damage the treatment works equipment (e.g., valves and pumps). The screenings are processed according to local situations.
Sand removal
The sand contained in the waste water has to be removed as it tends to settle in the pipework on account of its high density and cause abrasion to the equipment (e.g., centrifugal separators and turbines). Sand is generally removed by passing the waste water through a channel of constant cross-section at a velocity of 15 to 30 cm/s. The sand collects on the channel bottom and may be used, after washing to remove putrescible matter, as an inert material, such as for road building.
Oil removal
Oils and non-emulsifiable fats have to be removed because they would adhere to the equipment of the treatment works (e.g., basins and clarifiers) and interfere with the subsequent biological treatment. Oil and fat particles are made to collect on the surface by passing the waste water at an appropriate velocity through tanks of rectangular cross-section; they are skimmed off mechanically and may be used as a fuel. Multi-plate separators of compact design and high efficiency are frequently used for oil removal: the sewage is made to pass from above through stacks of flat inclined plates; the oil adheres to the bottom surfaces of the plates and moves to the top where it is collected. With both these processes, the de-oiled water is discharged at the bottom.
Sedimentation, flotation and coagulation
These processes enable the solids to be removed from the waste water, heavy ones (greater than 0.4 μm in diameter) by sedimentation and light ones (less than 0.4 μm) by flotation. This treatment, too, relies on the differences in density of the solids and of the flowing waste water which is passed through sedimentation tanks and flotation tanks made of concrete or steel. The particles to be separated collect in the bottom or at the surface, settling or rising at velocities which are proportional to the square of the particle radius and to the difference between the particle density and the apparent waste water density. Colloidal particles (e.g., proteins, latexes and oily emulsions) with sizes from 0.4 to 0.001 μm are not separated, as these colloids become hydrated and usually negatively charged by adsorption of ions. Consequently the particles repel each other so that they cannot coagulate and separate. However, if these particles are “destabilized”, they coagulate to form flocks greater than 4 μm, which can be separated as sludge in conventional sedimentation or flotation tanks. Destabilization is obtained by coagulation, that is, by adding 30 to 60 mg/l of an inorganic coagulant (aluminium sulphate, iron (II) sulphate or iron (III) chloride). The coagulant hydrolyses under given pH (acidity) conditions and forms positive polyvalent metal ions, which neutralize the negative charge of the colloid. Flocculation (the agglomeration of coagulated particles in flocks) is facilitated by adding 1 to 3 mg/l of organic polyelectrolytes (flocculation agents), resulting in flocks of 0.3 to 1 μm diameter which are easier to separate. Sedimentation tanks of the horizontal-flow type may be used; they have rectangular cross-section and flat or sloping bottoms. The waste water enters along one of the head sides, and the clarified water leaves over the edge at the opposite side. Also vertical flow sedimentation tanks can be used which are cylindrical in shape and have a bottom like an inverted right circular cone; the waste water enters in the middle, and the clarified water leaves the tank over the top indented edge to be collected into an external circumferential channel. With the two types of tank, the sludge settles on the bottom and is conveyed (if necessary by means of a raking gear) into a collector. The solids concentration in the sludge is 2 to 10%, whereas that of the clarified water is 20 to 80 mg/l.
The flotation tanks are usually cylindrical in shape and have fine bubble air diffusers installed in their bottoms, the sewage entering the tanks in the centre. The particles adhere to the bubbles, float to the surface and are skimmed off, while the clarified water is discharged below. In the case of the more efficient “dissolved-air floating tanks”, the waste water is saturated with air under a pressure of 2 to 5 bars and then allowed to expand in the centre of the floating tank, where the minute bubbles resulting from the decompression make the particles float to the surface.
Compared to sedimentation, flotation yields a thicker sludge at a higher particle separation velocity, and the equipment required is therefore smaller. On the other hand, the operating cost and the concentration of solids in the clarified water are higher.
Several tanks arranged in series are required for coagulating and flocculating a colloidal system. An inorganic coagulant and, if necessary, an acid or an alkali to correct the pH value are added to the waste water in the first tank, which is equipped with an agitator. The suspension is then passed into a second tank equipped with a high-speed agitator; here, the polyelectrolyte is added and dissolved within a few minutes. The flock growth takes place in a third tank with a slow-running agitator and is carried out for 10 to 15 minutes.
Biological Processes
Biological treatment processes remove organic biodegradable pollutants by use of micro-organisms. These organisms digest the pollutant by an aerobic or anaerobic process (with or without supply of atmospheric oxygen) and convert it into water, gases (carbon dioxide and methane) and a solid insoluble microbic mass which can be separated from the treated water. Especially in the case of industrial effluents proper conditions for the development of micro-organisms must be assured: presence of nitrogen and phosphorus compounds, traces of microelements, absence of toxic substances (heavy metals, etc.), optimum temperature and pH value. Biological treatment includes aerobic and anaerobic processes.
Aerobic processes
The aerobic processes are more or less complex according to the space available, the degree of purification required and the composition of the waste water.
Stabilization ponds
These are generally rectangular and 3 to 4 m deep. The sewage enters at one end, is left for 10 to 60 days and leaves the pond partly at the opposite end, partly by evaporation and partly by infiltration into the ground. The purification efficiency ranges from 10 to 90% according to the type of effluent and to the residual 5-day biological oxygen demand (BOD5) content (<40 mg/l). Oxygen is supplied from the atmosphere by diffusion through the surface of the water and from photosynthetic algae. The solids in suspension in the waste water and those produced by microbial activity settle on the bottom, where they are stabilized by aerobic and/or anaerobic processes according to the depth of the ponds which affects the diffusion both of oxygen and sunlight. The oxygen diffusion is frequently accelerated by surface aerators, which enable the volume of the ponds to be reduced.
This type of treatment is very economical if space is available, but requires clay-like soil to prevent the pollution of underground water by toxic effluents.
Activated sludge
This is used for an accelerated treatment carried out in concrete or steel tanks of 3 to 5 m depth where the waste water comes into contact with a suspension of micro-organisms (2 to 10 g/l) which is oxygenated by means of surface aerators or by blowing in air. After 3 to 24 hours, the mixture of treated water and micro-organisms is passed into a sedimentation tank where the sludge made up by micro-organisms is separated from the water. The micro-organisms are partly returned to the aerated tank and partly evacuated.
There are various types of activated-sludge processes (e.g., contact-stabilization systems and use of pure oxygen) which yield purification efficiencies of greater than 95% even for industrial effluents but they require accurate controls and high energy consumption for oxygen supply.
Percolating filters
With this technique the micro-organisms are not kept in suspension in the waste water, but adhere to the surface of a filling material over which the sewage is sprayed. Air circulates through the material and supplies the required oxygen without any energy consumption. According to the type of waste water and to increase efficiency, part of the treated water is recirculated to the top of the filter bed.
Where land is available, low-cost filling materials of appropriate size (e.g., crushed stone, clinker and limestone) are used, and on account of the weight of the bed the percolating filter is generally constructed as a 1 m high concrete tank usually sunk in the ground. If there is not enough land, more costly lightweight packing materials such as high-rate plastic honeycomb media, with up to 250 square metres of surface area/cubic metre of media, are stacked in percolating towers up to 10 m high.
The waste water is distributed over the filter bed by a mobile or fixed sparging mechanism and collected in the floor to be eventually recirculated to the top and to be passed into a sedimentation tank where the sludge formed can settle. Openings at the bottom of the percolating filter allow for air circulation through the filter bed. Pollutants removal efficiencies of 30 to 90% are achieved. In many cases several filters are arranged in series. This technique, which requires little energy and is easy to operate, has found widespread use and is recommended for cases where land is available, for instance, in developing countries.
Biodiscs
A set of flat plastic discs mounted parallel on a horizontal rotating shaft are partially immersed in the waste water contained in a tank. Due to the rotation the biological felt that covers the discs is brought into contact with the effluents and atmospheric oxygen. The biological sludge coming off the biodiscs remains in suspension in the waste water, and the system acts as activated sludge and sedimentation tank at the same time. Biodiscs are suitable for small to medium-sized industrial factories and communities, take up little space, are easy to operate, require little energy and yield efficiencies of up to 90%.
Anaerobic processes
Anaerobic processes are carried out by two groups of micro-organisms—hydrolytic bacteria, which decompose complex substances (polysaccharides, proteins, lipids, etc.) to acetic acid, hydrogen, carbon dioxide and water; and methanogenic bacteria, which convert these substances to a biomass (that can be removed from the treated sewage by sedimentation) and to biogas containing 65 to 70% methane, the remainder being carbon dioxide, and having a high heat value.
These two groups of micro-organisms, which are very sensitive to toxic contaminants, act simultaneously in the absence of air at an almost neutral pH value, some requiring a temperature of 20 to 38oC (mesophilic bacteria) and other, more delicate ones, 60 to 65oC (thermophilic bacteria). The process is carried out in stirred, closed concrete or steel digesters, where the required temperature is held by thermostats. Typical is the contact process, where the digester is followed by a sedimentation tank to separate the sludge, which is partially recirculated to the digester, from the treated water.
Anaerobic processes need neither oxygen nor power for oxygen supply and yield biogas, which can be used as a fuel (low operating costs). On the other hand, they are less efficient than aerobic processes (residual BOD5: 100 to 1,500 mg/l), are slower and more difficult to control, but enable faecal and pathogenic micro-organisms to be destroyed. They are used for treating strong wastes, such as sedimentation sludge from sewage, sludge in excess from activated sludge or percolating-filter treatments and industrial effluents with a BOD5 up to 30,000 mg/l (e.g., from distilleries, breweries, sugar refineries, abattoirs and paper mills).
Tertiary Processes
The more complex and more expensive tertiary processes make use of chemical reactions or specific chemicophysical or physical techniques to remove water-soluble non-biodegradable pollutants, both organic (e.g., dyes and phenols) and inorganic (e.g., copper, mercury, nickel, phosphates, fluorides, nitrates and cyanides), especially from industrial waste water, because they cannot be removed by other treatments. Tertiary treatment also enables a high degree of water purification to be obtained, and the water thus treated may be used as drinking water or for manufacturing processes (steam generation, cooling systems, process water for particular purposes). The most important tertiary processes are as follows.
Precipitation
Precipitation is carried out in reactors made of an appropriate material and equipped with agitators where chemical reagents are added at a controlled temperature and pH value to convert the pollutant to an insoluble product. The precipitate obtained in the form of sludge is separated by conventional techniques from the treated water. In waste water from the fertilizer industry, for instance, phosphates and fluorides are rendered insoluble by reaction with lime at ambient temperature and at an alkaline pH; chromium (tanning industry), nickel and copper (electroplating shops) are precipitated as hydroxides at an alkaline pH after having been reduced with m-disulphite at a pH of 3 or lower.
Chemical oxidation
The organic pollutant is oxidized with reagents in reactors similar to those used for precipitation. The reaction is generally continued until water and carbon dioxide are obtained as final products. Cyanides, for instance, are destroyed at ambient temperature by adding sodium hypochlorite and calcium hypochlorite at alkaline pH, whereas azo- and anthraquinone-dyes are decomposed by hydrogen peroxide and ferrous sulphate at pH 4.5. Coloured effluents from the chemical industry containing 5 to 10% non-biodegradable organic substance are oxidized at 200 to 300°C at high pressure in reactors made of special materials by blowing air and oxygen into the liquid (wet oxidation); catalysts are sometimes used. Pathogens left in urban sewage after treatment are oxidized by chlorination or ozonisation to render the water drinkable.
Absorption
Some pollutants (e.g., phenols in waste water from coking plants, dyes in water for industrial or drinking purposes and surfactants) are effectively removed by absorption on activated carbon powder or granules which are highly porous and have a large specific surface area (of 1000 m2/g or more). The activated carbon powder is added in metered quantities to the waste water in stirred tanks, and 30 to 60 minutes later the spent powder is removed as a sludge. Granulated activated carbon is used in towers arranged in series through which the polluted water is passed. The spent carbon is regenerated in these towers, that is, the absorbed pollutant is removed either by chemical treatment (e.g., phenols are washed out with soda) or by thermal oxidation (e.g., dyes).
Ion exchange
Certain natural substances (e.g., zeolites) or artificial compounds (e.g., Permutit and resins) exchange, in a stoichiometric and reversible manner, the ions bound to them with those contained, even strongly diluted, in the waste water. Copper, chromium, nickel, nitrates and ammonia, for instance, are removed from waste water by percolation through columns packed with resins. When the resins are spent, they are reactivated by washing with regenerating solutions. Metals are thus recovered in a concentrated solution. This treatment, though costly, is efficient and advisable in cases where a high degree of purity is required (e.g., for waste water contaminated by toxic metals).
Reverse osmosis
In special cases it is possible to extract water of high purity, suitable for drinking, from diluted waste water by passing it through semi-permeable membranes. On the waste water side of the membrane the pollutants (chlorides, sulphates, phosphates, dyes, certain metals) are left as concentrated solutions which have to be disposed of or treated for recovery. The diluted waste water is subjected to pressures up to 50 bars in special plant containing synthetic membranes made of cellulose acetate or other polymers. The operating cost of this process is low, and separation efficiencies of greater than 95% may be obtained.
Sludge Treatment
Rendering pollutants insoluble during waste water treatment results in the production of considerable amounts of sludge (20 to 30% of the removed chemical oxygen demand (COD) which is strongly diluted (90 to 99% water)). The disposal of this sludge in a manner acceptable to the environment presupposes treatments with a cost of up to 50% of those required for waste water purification. The types of treatment depend on the destination of the sludge, depending in turn on its characteristics and on local situations. Sludge may be destined for:
- fertilization or dumping at sea if it is substantially free from toxic substances and contains nitrogen and phosphorus compounds (sludge from biological treatment), using fixed outfalls, lorries or barges
- sanitary landfill into pits dug in the ground, alternating layers of sludge and soil. Impermeabilisation of peats is required if the sludge contains toxic substances that may be washed out by atmospheric precipitations. The pits should be remote from water-bearing strata. Non-stabilized organic sludge is usually mixed with 10 to 15% lime to retard putrefaction.
- incineration in rotary or fluidized-bed furnaces if the sludge is rich in organic substances and free from volatile metals; if necessary, fuel is added, and the smoke emitted is purified.
The sludge is dewatered before its disposal to reduce both its volume and the cost of its treatment, and it is frequently stabilized to prevent its putrefaction and to render harmless any toxic substances it may contain.
Dewatering
Dewatering includes previous thickening in thickeners, similar to sedimentation tanks, where the sludge is left for 12 to 24 hours and loses part of the water which collects on the surface, while the thickened sludge is discharged below. The thickened sludge is dewatered, for example, by centrifugal separation or by filtration (under vacuum or pressure) with conventional equipment, or by exposure to the air in layers of 30 cm thick in sludge-drying beds consisting of rectangular concrete lagoons, approximately 50 cm deep, with a sloped bottom covered with a layer of sand to facilitate water drainage. Sludge containing colloidal substances should be previously destabilized by coagulation and flocculation, according to already described techniques.
Stabilization
Stabilization includes digestion and detoxification. Digestion is a long-term treatment of the sludge during which it loses 30 to 50% of its organic matter, accompanied by an increase in its mineral salt content. This sludge is no longer putrescible, any pathogens are destroyed and the filtrability is improved. Digestion may be of the aerobic type when the sludge is aerated during 8 to 15 days at ambient temperature in concrete tanks, the process being similar to activated-sludge treatment. It may be of the anaerobic type if the sludge is digested in plants similar to those used for the anaerobic waste treatment, at 35 to 40°C during 30 to 40 days, with the production of biogas. Digestion can be of the thermal type when the sludge is treated with hot air at 200 to 250°C and at a pressure of more than 100 bars during 15 to 30 minutes (wet combustion), or when it is treated, in the absence of air, at 180°C and at autogenous pressure, for 30 to 45 minutes.
Detoxification renders harmless sludge containing metals (e.g., chromium, nickel and lead), which are solidified by treatment with sodium silicate and autothermically converted into the corresponding insoluble silicates.
Domestic Waste Collection
In many locations domestic waste collection is performed by municipal employees. In others, by private companies. This article provides an overview of processes and hazards that are based on observations and experiences in the Province of Quebec, Canada. Editor.
Overview
Besides the few workers employed by municipalities in the Province of Quebec, Canada, that have their own waste collection boards, thousands of waste collectors and drivers are employed in hundreds of companies in the private sector.
Many private enterprises rely, either wholly or partially, upon jobbers who rent or own trucks and are responsible for the collectors who work for them. Competition in the sector is high, as municipal contracts are awarded to the lowest bidder, and there is a regular annual turnover of enterprises. The high competition also results in low and stable domestic waste-collection rates, and waste collection accounts for the lowest proportion of municipal taxes. However, as the existing landfills fill up, landfill costs rise, obliging municipalities to consider integrated waste-management systems. All municipal workers are unionized. Unionization of private-sector workers began in the 1980s, and 20 to 30% of them are now unionized.
Work Processes
Waste collection is a dangerous trade. If we recognize that garbage trucks are similar to hydraulic presses, it follows that waste collection is like working on a mobile industrial press under conditions much more demanding than those encountered in most factories. In waste collection, the machine travels through traffic in all seasons and workers must feed it by running behind it and tossing irregular objects of variable volume and weight, containing invisible and hazardous objects, into it. On average, collectors handle 2.4 tonnes of waste per hour. The efficiency of waste collection operations is entirely dependent on determinants of work rate and rhythm. The need to avoid rush-hour traffic and bridge line-ups creates time pressures at collection points and during transport. Speed is again of importance during unloading at landfills and incinerators.
Several aspects of waste collection influence workload and hazards. First, remuneration is on a flat-rate basis, that is, the territory specified by contract must be completely cleared of domestic waste on collection day. Since the volume of waste depends on residents’ activities and varies from day to day and from season to season, the workload varies enormously. Secondly, workers are in direct contact with the objects and waste collected. This is quite different from the situation in the commercial and industrial waste-collection sectors, where waste-filled containers are collected by either front-loading trucks equipped with automated fork-lifts or by roll-off trucks. This means that workers in those sectors do not handle the waste containers and are not in direct contact with the waste. Working conditions for these collectors therefore more closely resemble those of domestic waste drivers, rather than domestic waste collectors.
Residential collection (also known as domestic collection) is, on the other hand, primarily manual, and workers continue to handle a wide variety of objects and containers of variable size, nature and weight. A few suburban and rural municipalities have implemented semi-automated collection, involving the use of mobile domestic waste bins and side-loading collectors (figure 1). However, most domestic waste continues to be collected manually, especially in cities. The principal characteristic of this job is thus significant physical exertion.
Figure 1. Automatic, side-loading refuse collector.

Pak Mor Manufacturing Company
Hazards
A study involving field observations and measurements, interviews with management and workers, statistical analysis of 755 occupational accidents and analysis of video sequences revealed a number of potential hazards (Bourdouxhe, Cloutier and Guertin 1992).
Workload
On average, waste collectors handle 16,000 kg spread out over 500 collection points every day, equivalent to a collection density of 550 kg/km. Collection takes almost 6 hours, equivalent to 2.4 tonnes/hour, and involves walking 11 km during a total work day of 9 hours. Collection speed averages 4.6 km/h, over a territory of almost 30 km of sidewalks, streets and lanes. Rest periods are limited to a few minutes precariously balanced on the rear platform, or, in the case of driver-collectors of side-loading trucks, at the wheel. This demanding workload is exacerbated by such factors as the frequency of truck dismounts and mounts, the distance covered, travel modes, the static effort required to maintain one’s balance on the rear platform (a minimum of 13 kg of force), the frequency of handling operations per unit time, the variety of postures required (bending movements), the frequency of tosses and twisting movements of the trunk and the high collection rate per unit time in some sectors. The fact that the Association française de normalisation (AFNOR) adapted weight standard for manual handling was exceeded in 23% of observed trips is eloquent testimony of the impact of these factors. When workers’ capacities (established to be 3.0 tonnes/hour for rear-loading trucks, and 1.9 tonnes/hour for side-loading ones) are taken into account, the frequency with which the AFNOR standard is exceeded rises to 37%.
Diversity and nature of objects handled
Manipulation of objects and containers of variable weight and volume interrupts the smooth flow of operations and breaks work rhythms. Objects in this category, often hidden by residents, include heavy, large or bulky objects, sharp or pointed objects and hazardous materials. The most frequently encountered hazards are listed in table 1.
Table 1. Hazardous objects found in domestic waste collections.
Glass, window panes, fluorescent tubing
Battery acid, cans of solvent or paint, aerosol containers, gas cylinders, motor oil
Construction waste, dust, plaster, sawdust, hearth cinders
Pieces of wood with nails in them
Syringes, medical waste
Garden waste, grass, rocks, earth
Furniture, electrical appliances, other large domestic trash
Pre-compacted waste (in apartment buildings)
Excessive numbers of small containers from small businesses and restaurants
Large amounts of vegetable and animal waste in rural sectors
Extra-large bags
Prohibited containers (e.g., no handles, excessive weight, 55-gallon oil drums, thin-necked drums, garbage cans without covers)
Small, apparently light bags that are in fact heavy
Excessive numbers of small bags
Paper bags and boxes that rip
All waste that is hidden because of its excessive weight or toxicity, or that surprises unprepared workers
Commercial containers that must be emptied with an improvised system, which is often inappropriate and dangerous
Workers are greatly helped by having residents sort waste into colour-coded bags and mobile domestic bins which facilitate the collection and allow better control of work rhythm and effort.
Climatic conditions and the nature of objects transported
Wet paper bags and poor-quality plastic bags that rip and scatter their contents over the sidewalk, frozen garbage cans and domestic bins stuck in snow banks can cause mishaps and dangerous recovery manoeuvres.
Work schedule
The need to rush, traffic problems, parked cars and crowded streets all can contribute to dangerous situations.
In an attempt to reduce their workload and maintain a high but constant work rhythm in the face of these constraints, workers often attempt to save time or effort by adopting work strategies that may be hazardous. The most commonly observed strategies included kicking bags or cardboard boxes towards the truck, zigzagging across the road to collect from both sides of the street, grabbing bags while the truck is in motion, carrying bags under the arm or against the body, using the thigh to help load bags and garbage cans, hand-picking of waste scattered on the ground and manual compaction (pushing garbage overflowing the hopper with the hands when the compacting system is incapable of processing the load rapidly enough). For example, in suburban collection with a rear-loading truck, almost 1,500 situations were observed per hour that could result in accidents or increase workload. These included:
- 53 mounts and dismounts from the truck’s rear platform
- 38 short runs
- 482 bending movements
- 203 tosses
- 159 twisting movements
- 277 potentially hazardous actions (including 255 work strategies aimed at reducing workload by saving time or effort)
- 285 instances of increased workload, including 11 mishap- recovery activities
- 274 dangerous or heavy objects or containers.
Collection with side-loading trucks (see figure 1) or small mobile domestic bins reduces the manipulation of heavy or dangerous objects and the frequency of situations that could result in accidents or an increase in workload.
Use of public thoroughfares
The street is the collectors’ workplace. This exposes them to such hazards as vehicular traffic, blocked access to residents’ waste receptacles, accumulation of water, snow, ice and neighbourhood dogs.
Vehicles
Rear-loading trucks (figure 2) often have excessively high or shallow steps and rear platforms that are difficult to mount and render descents perilously similar to jumps. Hand-rails that are too high or too close to the truck body only worsen the situation. These conditions increase the frequency of falls and of collisions with structures adjacent to the rear platform. In addition, the upper edge of the hopper is very high, and shorter workers must expend additional energy lifting objects into it from the ground. In some cases, workers use their legs or thighs for support or additional power when loading the hopper.
Figure 2. Back-loading enclosed compactor truck.

National Safety Council (US) The packer-blade comes down within centimetres of the edge of the platform. The blade has the capacity to cut protruding objects.
The characteristics of side-loading trucks and the operations related to their loading result in specific repetitive movements likely to cause muscle and joint problems in the shoulder and upper back. Driver-collectors of side-loading trucks have an additional constraint, as they must cope with both the physical strain of collection and the mental strain of driving.
Personal protective equipment
While the theoretical value of PPE is beyond question, it may nevertheless prove inadequate in practice. In concrete terms, the equipment may be inappropriate for the conditions under which collection is carried out. Boots, in particular, are incompatible with the narrow utilizable height of rear platforms and the high work rhythm necessitated by the manner in which collection is organized. Strong, puncture-resistant yet flexible gloves are valuable in protecting against hand injuries.
Work organization
Some aspects of work organization increase workload and, by extension, hazards. In common with most flat-rate situations, the main advantage to workers of this system is the ability to manage their work time and save time by adopting a rapid work rhythm as they see fit. This explains why attempts, based on safety considerations, to slow down the pace of work have been unsuccessful. Some work schedules exceed workers’ capacities.
The role of the myriad variations of residents’ behaviour in the creation of additional hazards merits a study in itself. Prohibited or dangerous wastes skilfully hidden in regular waste, non-standard containers, excessively large or heavy objects, disagreements over collection times and non-conformity with bylaws all increase the number of hazards—and the potential for conflicts between residents and collectors. Collectors are often reduced to the role of “garbage police”, educators and buffers between municipalities, enterprises and residents.
Collection of materials for recycling is not without its own problems despite a low waste density and collection rates far below those of traditional collection (with the exception of the collection of leaves for composting). The hourly frequency of situations that could result in accidents is often high. The fact that this is a new type of work for which few workers have been trained should be borne in mind.
In several cases, workers are obliged to perform such dangerous activities as mounting the truck’s compaction box to get into the compartments and move piles of paper and cardboard with their feet. Several work strategies aimed at speeding up work rhythm have also been observed, e.g., hand re-sorting of the material to be recycled and removing objects from the recycling box and carrying them to the truck, rather than carrying the box to the truck. The frequency of mishaps and disruptions of normal work activity in this type of collection is particularly high. These mishaps result from workers doing ad hoc activities that are themselves dangerous.
Occupational Accidents and Prevention
Domestic waste collection is a dangerous trade. Statistics support this impression. The average annual accident rate in this industry, for all types of enterprise, truck and trade, is almost 80 accidents for every 2,000 hours of collection. This is equivalent to 8 workers of every 10 suffering an injury at least once a year. Four accidents occur for every 1,000 10-tonne truckloads. On average, each accident results in 10 lost workdays and accident compensation of $820 (Canadian). Indices of injury frequency and severity vary among enterprises, with higher rates observed in municipal enterprises (74 accidents/100 workers versus 57/100 workers in private enterprises) (Bourdouxhe, Cloutier and Guertin 1992). The most common accidents are listed in table 2.
Table 2. Most common accidents in domestic waste collection, Quebec, Canada.
|
Injury |
Cause |
Per cent of accidents studied |
|
Back or shoulder pain |
Tossing or twisting movements during collection of bags |
19 |
|
Back injuries |
Excessive efforts while lifting objects |
18 |
|
Ankle sprains |
Falls or slips while dismounting from the truck or moving in its vicinity |
18 |
|
Crushed hands, fingers, arms or knees |
Struck by containers or heavy objects, being caught between the vehicle and containers, or collisions with part of the vehicle or parked cars |
18 |
|
Hand and thigh lacerations of variable depth |
Glass, nails, or syringes, occurring during hopper loading |
15 |
|
Scrapes and bruises |
Contact or collisions |
5 |
|
Eye or respiratory-tract irritation |
Dust or splashes of liquids occurring during work near the hopper during compaction |
5 |
|
Other |
2 |
Collectors typically suffer hand and thigh lacerations, drivers typically suffer sprained ankles resulting from falls during cabin dismounts and driver-collectors of side-loading trucks typically suffer shoulder and upper back pain resulting from tossing movements. The nature of the accidents also depends on the type of truck, although this can also be seen as a reflection of the specific trades associated with rear- and side-loading trucks. These differences are related to equipment design, the type of movements required and the nature and density of waste collected in the sectors in which these two types of truck are used.
Prevention
The following are ten categories in which improvements could make domestic waste collection safer:
- management of health and safety (for instance, the development of accident-prevention programmes based on workers’ knowledge of occupational hazards which are better adapted to actual tasks)
- training and hiring
- work organization, organization of collection and workload
- vehicles
- training and work conditions of auxiliary, occasional and temporary workers
- collection contracts
- public management
- collaboration between employer associations (municipal and private), workers and municipal or regional decision-making bodies
- stability of the workforce
- research on personal protective equipment, ergonomic design of trucks, subcontracting jobbers and safety.
Conclusion
Domestic waste collection is an important but hazardous activity. Protection of workers is made more difficult where this service is contracted out to private sector enterprises which, as in the province of Quebec, may subcontract the work to many smaller jobbers. A large number of ergonomic and accident hazards, compounded by work quotas, adverse weather and local street and traffic problems must be confronted and controlled if workers’ health and safety are to be maintained.
Beekeeping, Insect Raising and Silk Production
Some information on the silk industry was adapted from the article by J. Kubota in the 3rd edition of this Encyclopaedia.
More than a million species of insects exist in the world, and the global mass of insects exceeds the total mass of all other terrestrial animals. Insects such as crickets, grasshoppers, locusts, termites, beetle larvae, wasps, bees and moth caterpillars are among about 500 species that form part of the regular diet of people around the world. Usually humans hunt or gather insects for food rather than intentionally rearing and harvesting them.
In addition to food, humans use insects as sources of pollination, biological controls of pests and fibre. Different uses depend on the four stages of the insect’s life cycle, which consist of egg, larva, pupa and adult. Examples of commercial uses of insects include beekeeping (nearly 1 billion tonnes of honey produced annually and pollination of fruit and seed crops), insect rearing (more than 500 species in culture, including those used for insect biological control), shellac production (36,000 tonnes annually) and silk production (180,000 tonnes annually).
Beekeeping
Beekeepers raise the honey-bee in apiaries, a collection of hives that house bee colonies. The honey-bee is a source of flower pollination, honey and wax. Bees are important pollinators, making more than 46,430 foraging trips per bee for each kilogram of honey that they produce. During each foraging trip, the honey-bee will visit 500 flowers within a 25-minute period. The honey-bee’s source of honey is flower nectar. The bee uses the enzyme invertase to convert sucrose in the nectar into glucose and fructose and, with water evaporation, honey is produced. In addition, bumble-bees and cutter bees are grown for pollinating, respectively, tomato plants and alfalfa.
The honey-bee colony collects around a single queen bee, and they will colonize in boxes—artificial hives. Beekeepers establish an infant colony of about 10,000 bees in the bottom box of the hive, called a brood chamber. Each chamber contains ten panels with cells that are used for either storing honey or laying eggs. The queen lays about 1,500 eggs per day. The beekeeper then adds a food chamber super (a box placed on top of the brood box), which becomes the storage chamber for honey, on which the bees will survive through the winter. The colony continues to multiply, becoming mature at about 60,000 bees. The beekeeper adds a queen excluder (a flat panel that the larger queen cannot enter) on top of the food super to prevent the queen from laying eggs in additional shallow supers that will be stacked on top of the excluder. These additional supers are designed for harvesting only honey without the eggs.
The beekeeper moves the hives to where flowers are budding. A honey-bee colony can forage over an area of 48 hectares, and 1 hectare can support about two hives. The honey is harvested during the summer from the shallow supers, which can be stacked seven high as the colony grows and the bees fill the panels with honey. The supers with honey-laden panels are transported to the honey “house” for extraction. A sharp, warm knife, called an uncapping knife, is used to remove the wax caps that the bees have placed over the honeycombs within the panels. The honey is then extracted from the panels with a centrifugal force machine. The honey is collected and bottled for sale (Vivian 1986).
At the end of the season, the beekeeper winterizes the hives, wrapping them in tar paper to protect the colonies from the winter wind and to absorb the solar heat. The beekeeper also provides the bees with medicated sugar syrup for their winter consumption. In the spring, the hives are opened to begin production as mature honeybee colonies. If the colony becomes crowded, the colony will create another queen through special feeding, and the old queen will swarm with about half of the colony to find another accommodation. The beekeeper may capture the swarm and treat it as an infant colony.
Beekeepers are exposed to two related hazards from honey-bee stings. One hazard is sting envenomation. The other is venom hypersensitivity reaction and possible anaphylactic shock. Males at 40 years of age and older are at highest risk of fatal reactions. About 2% of the general population is thought to be allergic to venom, but systemic reactions in beekeepers and their immediate family members are estimated at 8.9%. The reaction incidence varies inversely to the numbers of stings received. Anaphylactic reactions to bumble-bee venom are rare except among bumble bee keepers, and their risk is greater if they have been sensitized to honey bee venom.
If a honey-bee stings the beekeeper, the stinger should be removed, and the sting site should be washed. Ice or a paste of baking soda and water should be applied to the site of envenomation. The victim should be watched for signs of systemic reaction, which can be a medical emergency. For anaphylactic reactions, epinephrine is administered subcutaneously at the first sign of symptoms. To assure safe beekeeping, the beekeeper should use smoke at the beehive to neutralize the bees’ protective behaviour and should wear a protective hood and veil, thin gloves and log sleeves or coveralls. Bees are attracted to sweat for the moisture, so beekeepers should not wear watch bands or belts where sweat collects. In extracting the honey, the beekeeper should keep his or her thumb and fingers clear of the cutting motion of the uncapping knife.
Mass Insect Raising
More than 500 species of arthropods are reared in the laboratory, including ants, beetles, mites, flies, moths, spiders and ticks. An important use of these arthropods is as biological controls for other animal species. For example, 2,000 years ago, markets in China sold nests of weaver ants to place in citrus orchards to prey on crop pests. Today, more than 5,000 species of insects have been identified worldwide as possible biological controls for crop pests, and 300 are successfully used regularly in 60 countries. Disease vectors have also become targets for biological control. As an example, the carnivorous mosquito from Southeast Asia, Toxorhynchites spp., also called the “tox” mosquito, has a larva that feeds on the larvae of the tiger mosquito, Aedesspp., which transmits diseases such as dengue fever to humans (O’Toole 1995).
Mass rearing facilities have been developed to raise sterile insects as a non-chemical pest-suppression tool. One such facility in Egypt rears a billion fruit flies (about 7 tonnes) each week. This rearing industry has two major cycles. One is the feed conversion or larval incubation cycle, and the other is the propagation or egg-production cycle. The sterile insect technique was first used to eliminate the screw worm, which preyed on cattle. Sterilization is accomplished by irradiating the pupae just prior to adult emergence from the cocoon with either x rays or gamma rays. This technique takes mass quantities of reared, sterile insects and releases them into infested areas where the sterile males mate with the wild, fertile females. Breaking the insect’s life cycle has dramatically reduced the fertility rate of these pests. This technique is used on screw worms, gypsy moths, boll weevils and fruit flies (Kok, Lomaliza and Shivhara 1988).
A typical sterile insect facility has an airlock system to restrict unwanted insect entry and fertile insect escape. Rearing tasks include mopping and sweeping, egg stacking, tray washing, diet preparation, inoculation (placing eggs into agar), pupae dyeing, emergence tending, packing, quarantining, irradiating, screening and weighing. In the pupae room, vermiculite is mixed with water and placed in trays. The trays are stacked, and the vermiculite dust is swept with a broom. The pupae are separated from the vermiculite with a sieve. The insect pupae chosen for the sterile insect technique are transported in trays stacked on racks to the irradiation chamber in a different area or facility, where they are irradiated and rendered sterile (Froehlich 1995; Kiefer 1996).
Insect workers, including silkworm workers, may have an allergic reaction to arthropod allergens (scales, hairs, other body parts). Initial symptoms are itchy eyes and irritation of the nose followed by intermittent episodes of wheezing, coughing and breathlessness. Subsequent asthma attacks are triggered by re-exposure to the allergen.
Entomologists and workers in sterile fly facilities are exposed to a variety of potentially hazardous, flammable agents. These agents include: in entomology laboratories, isopropyl alcohol, ethyl alcohol and xylene; in the diet preparation room, isopropyl alcohol is used in water solution to sterilize walls and ceilings with a sprayer. Vermiculite dust poses respiratory concerns. Some vermiculites are contaminated with asbestos. Air-handling units in these facilities emit noise that may be damaging to employee hearing. Proper exhaust ventilation and personal respiratory protection can be used in facilities to control exposure to airborne allergens and dusts. Non-dusty working materials should be used. Air conditioning and frequent changes of filters may help reduce airborne levels of spines and hairs. X rays or gamma rays (ionizing radiation) can damage genetic material. Protection is needed against x rays or gamma rays and their sources in the irradiation facilities (Froehlich 1995; Kiefer 1996).
Silkworm Raising
Vermiculture, the raising of worms, has a long history in some cultures. Worms, especially the meal worm (which is a larva rather than a true worm) from the darkling beetle, are raised by the billions as animal fodder for laboratory animals and pets. Worms are also used in composting operations (vermi-composting).
Sericulture is the term used for silkworm cocoon production, which includes silkworm feeding and cocoon formation. Cultivation of the silkworm and the silk moth caterpillar dates back to 3000 BC in China. Silkworm farmers have domesticated the silkworm moth; there are no remaining wild populations. Silkworms eat only white mulberry leaves. Fibre production thus has historically depended upon the leafing season of the mulberry tree. Artificial foods have been developed for the silkworm so that production can extend the year around. Silkworms are raised on trays sometimes mounted on racks. The worms take about 42 days of feeding at a constant temperature of 25 °C. Artificial heating may be required. Silk is a secretion from the silkworm’s mouth that solidifies upon contact with air. The silkworm secretes about 2 km of silk fibre to form a cocoon during the pupal stage (Johnson 1982). After the cocoon is formed, the silkworm farmer kills the pupa in a hot oven, and ships the cocoon to a factory. At the factory, silk is harvested from the cocoon and spun into thread and yarn.
Nine per cent of silkworm workers manifest asthma in response to silkworm moth scales, although most asthma in silkworm workers is attributed to inhalation of silkworm faeces. In addition, contact of the skin with silkworm caterpillar hairs may produce a primary irritant contact-dermatitis. Contact with raw silk may also produce allergic skin reactions. For silk moth production, hyposensitization therapy (for moth scales and faeces) provides improvement for 79.4% of recipients. Corticosteroids may reverse the effects of inhaled antigens. Skin lesions may respond to topical corticosteroid lotions and creams. Oral antihistamines relieve itching and burning. Carbon monoxide poisoning has been identified among some silkworm farmers in their homes, where they are maintaining warmth with charcoal fires as they raise the silkworms. Charcoal fires and kerosene heaters should be replaced with electric heaters to avoid carbon monoxide exposures.
Fish Farming and Aquaculture
Background
Rearing marine organisms for food has been a widespread practice since ancient times. However, large-scale farming of molluscs, crustaceans and bony fishes has rapidly gained momentum since the early 1980s, with 20% of the world’s seafood harvest now farmed; this is projected to increase to 25% by 2000 (Douglas 1995; Crowley 1995). Expansion of world markets contemporaneous with depletion of wild stocks has resulted in very rapid growth of this industry.
Land-based aquaculture takes place in tanks and ponds, while water-based culture systems generally employ screened cages or moored net pens of widely varying designs (Kuo and Beveridge 1990) in salt water (mariculture) or fresh rivers.
Aquaculture is performed as either an extensive or intensive practice. Extensive aquaculture entails some form of environmental enhancement for naturally produced species of fish, shellfish or aquatic plants. An example of such a practice would be laying down oyster shells to be used as attachment substrate for juvenile oysters. Intensive aquaculture incorporates more complex technology and capital investment in the culture of aquatic organisms. A salmon hatchery that uses concrete tanks supplied with water via some delivery system is an example. Intensive aquaculture also requires greater allocation of labour in the operation.
The process of intensive aquaculture includes the acquisition of broodstock adults used for production of gametes, gamete collection and fertilization, incubation of eggs and juvenile rearing; it may include rearing of adults to market size or release of the organism into the environment. Herein lies the difference between farming and enhancement aquaculture. Farming means rearing the organism to market size, generally in an enclosed system. Aquaculture for enhancement requires the release of the organism into the natural environment to be harvested at a later date. The essential role of enhancement is to produce a specific organism as a supplement to natural production, not as a replacement. Aquaculture can also be in the form of mitigation for loss of natural production caused by a natural or human-made event—for example, construction of a salmon hatchery to replace lost natural production caused by the damming of a stream for hydroelectric power production.
Aquaculture can occur in land-based facilities, on-bottom marine and freshwater environments and floating structures. Floating net pens are used for fish farming, and cages suspended from raft or buoy flotation are commonly used for shellfish culture.
Land-based operations require the construction of dams and/or excavation of holes for ponds and raceways for water flushing. Mariculture can involve the construction and maintenance of complex structures in harsh environments. Handling of smolt (for bony fishes) or tiny invertebrates, feed, chemical treatments for water and the animals being raised and wastes have all evolved into highly specialized activities as the industry has developed.
Hazards and Controls
Injuries
Fish farming operations afford many injury risks, combining some of those common to all modern agriculture operations (e.g., entanglement in large machinery, hearing loss from prolonged exposure to loud engines) with some hazards unique to these operations. Slips and falls can have particularly bad outcomes if they occur near raceways or pens, as there are the dual added risks of drowning and biological or chemical contamination from polluted water.
Severe lacerations and even amputations may take place during roe-stripping, fish butchering and mollusc shelling and can be prevented by the use of guards, protective gloves and equipment designed specifically for each task. Lacerations contaminated by fish slime and blood can cause serious local and even systemic infections (“fish poisoning”). Prompt disinfection and debridement is essential for these injuries.
Electrofishing (used to stun fish during survey counts, and increasingly in collection of broodstock at hatcheries) carries a high potential for electrical shock to the operators and bystanders (National Safety Council 1985) and should be done only by trained operators, with personnel trained in cardiopulmonary resuscitation (CPR) on site. Only equipment specifically designed for electrofishing operations in water should be employed and scrupulous attention must be paid to establishing and maintaining good insulation and grounding.
All water poses drowning risks, while cold waters pose the additional hazard of hypothermia. Accidental immersions due to falls overboard must be guarded against, as must potential for ensnarement or entrapment in nets. Approved personal flotation devices should be worn by all workers at all times on or near the water, and some thermal protection should also be worn when working around cold waters (Lincoln and Klatt 1994). Mariculture personnel should be trained in marine survival and rescue techniques, as well as CPR.
Repetitive strain injuries may also occur in butchering and hand-feeding operations and can be largely avoided by attention to ergonomics (via task analysis and equipment modifications as necessary) and frequent task rotations of manual workers. Those workers developing repetitive strain injury symptoms should receive prompt evaluation and treatment and possible reassignment.
Sleep deprivation can be a risk factor for injuries in aquaculture facilities requiring intensive labour over a short duration of time (e.g., egg harvest at salmon hatcheries).
Health hazards
Diving is frequently required in construction and maintenance of fishpens. Predictably, decompression illness (“bends”) has been observed among divers not carefully observing depth/time limits (“dive tables”). There have also been reports of decompression illness occurring in divers observing these limits but making many repetitive short dives; alternative methods (not using divers) should be developed for clearing dead fish from and maintaining pens (Douglas and Milne 1991). When diving is deemed necessary, observing published dive tables, avoiding repetitive dives, always diving with a second diver (“buddy diving”) and rapid evaluation of decompression-like illnesses for possible hyperbaric oxygen therapy should be regular practices.
Severe organophosphate poisoning has occurred in workers incidental to pesticidal treatment of sea lice on salmon (Douglas 1995). Algicides deployed to control blooms may be toxic to workers, and toxic marine and freshwater algae themselves may afford worker hazards (Baxter 1991). Bath treatments for fungal infections in fish may use formaldehyde and other toxic agents (Douglas 1995). Workers must receive adequate instruction and allotment of time for safe handling of all agricultural chemicals and hygienic practices around contaminated waters.
Respiratory illnesses ranging from rhinitis to severe bronchospasm (asthma-like symptoms) have occurred due to sensitization to putative endotoxins of gram-negative bacteria contaminating farmed trout during gutting operations (Sherson, Hansen and Sigsgaard 1989), and respiratory sensitization may occur to antibiotics in medicated fish feeds. Careful attention to personal cleanliness, keeping seafood clean during butchering and handling and respiratory protection will help ensure against these problems. Workers developing sensitivity should avoid subsequent exposures to the implicated antigens. Constant immersion of hands can facilitate dermal sensitization to agricultural chemicals and foreign (fish) proteins. Hygienic practice and use of task-appropriate gloves (such as cuffed, insulated, waterproof neoprene during cold butchering operations) will reduce this risk.
Sunburn and keratotic (chronic) skin injury may result from exposure to sunlight. Wearing hats, adequate clothing and sunscreen should be de rigueur for all outdoor agricultural workers.
Large quantities of stored fish feeds are often raided by or infested with rats and other rodents, posing a risk for leptospirosis (Weil’s disease). Workers handling fish feeds must be vigilant about feed storage and rodent control and protect abraded skin and mucous membranes from contact with potentially contaminated feeds and soiled pond waters. Feeds with known contamination with rat urine should be handled as potentially infectious, and discarded promptly (Ferguson and Path 1993; Benenson 1995; Robertson et al. 1981).
Eczema and dermatitis can easily evolve from inflammation of skin macerated by constant water contact. Also, this inflammation and wet conditions can foster reproduction of human papillaviridae, leading to rapid spread of skin warts (Verruca vulgaris). Prevention is best accomplished by keeping hands as dry as possible and using appropriate gloves. Emollients are of some value in the management of minor skin irritation from water contact, but topical treatment with corticosteroids or antibiotic creams (after evaluation by a physician) may be necessary if initial treatment is unsuccessful.
Environmental Impacts
Demand for fresh water can be extremely high in all of these systems, with estimates centring on 40,000 litres required for each 0.5 kg of bony fish raised to maturity (Crowley 1995). Recirculation with filtration can greatly reduce demand, but requires intensive application of new technologies (e.g., zeolites to attract ammonia).
Fish farm discharges can include as much faecal waste as that from small cities, and regulations are rapidly proliferating for control of these discharges (Crowley 1995).
Consumption of plankton and krill, and side effects of mariculture such as algal blooms, can lead to major disruptions in species balance in the local ecosystems surrounding fish farms.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."