- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Healthcare Workers and Infectious Diseases
Natural Felt Products
Felt is a fibrous material made by interlocking fibres of fur, hair or wool through the application of heat, moisture, friction and other processes into an unwoven, densely matted fabric. There are also needleloom felts, in which the felt is attached to a loosely woven backing fabric, usually made of wool or jute.
Fur Felt Processing
Fur felt, used most frequently in hats, is usually made from the fur of rodents (e.g., rabbits, hares, muskrats, coypus and beavers), with other animals used less frequently. After sorting, the skins are carroted using hydrogen peroxide and sulphuric acid, and then the following processes are performed: cutting of hair, hardening and dyeing. For dyeing, synthetic dyestuffs are usually used (e.g., acid dyes or dyes containing complex metal compounds). The dyed felt is weighted using a shellac or vinyl polyacetate.
Wool Felt Processing
Wool used for felt manufacture may be unused or reclaimed. Jute, generally obtained from old sacks, is used for certain needlefelts, and other fibres such as cotton, silk and synthetic fibres may be added.
The wool is sorted and selected. To separate the fibres, it is ragged in a rag-grinding machine, a spiked cylinder that rotates and tears up the fabric, and then garnetted in a machine that has rollers and cylinders covered with fine saw-toothed wires. The fibres are carbonized in an 18% sulphuric acid solution and, after drying at a temperature of 100 ºC, they are blended and, when necessary, oiled with mineral oil with emulsifier. After teasing and carding, which further blends the fibres and arranges them more or less parallel to one another, the material is deposited on a moving belt as layers of a fine web that are wound up on poles to form batts. The loose batts are taken to the hardening room, where they are sprinkled with water and pressed between two heavy plates, the top one of which vibrates, causing the fibres to curl and cling together.
To complete the felting, the material is placed in bowls of dilute sulphuric acid and pounded by heavy wooden hammers. It is washed (with the addition of tetrachloroethylene), dewatered and dyed, usually with synthetic dyestuffs. Chemicals may be added to make the felt rot-resistant. The final steps include drying (at 65 °C for soft felts, 112 °C for hard felts), shearing, sanding, brushing, pressing and trimming.
Safety and Health Hazards
Accidents
The machines used in felt manufacturing have driving belts, chain and sprocket drives, rotating shafts, spiked drums and rollers used in garnetting and teasing, heavy presses, rollers and hammers, and so on, all of which must be properly guarded and have lockout/tagout systems to prevent injuries when they are being serviced or cleaned. Good housekeeping is also necessary to avoid slips and falls.
Noise
Many of the operations are noisy; when safe noise levels cannot be maintained by enclosures, baffles and proper lubrication, personal hearing protection must be made available. A hearing conservation programme featuring periodic audiograms is required in many countries.
Dust
Felt workplaces are dusty and are not recommended for persons with chronic respiratory diseases. While, fortunately, the dust is not associated with any specific disease, adequate exhaust ventilation is necessary. Animal hair can evoke allergic reactions in sensitive individuals, but bronchial asthma appears to be infrequent. Dust also can be a fire hazard.
Chemicals
The sulphuric acid solution used in felt making is usually dilute, but care is needed when diluting the supply of concentrated acid to the desired level. The danger of splashes and spills requires that eyewash facilities be nearby and that workers be fitted with protective clothing (e.g., goggles, aprons, gloves and shoes).
Tanning of certain papermakers’ felts may involve the use of quinone, which can cause severe damage to skin and mucous membranes. The dust or vapour of this compound can cause staining of the conjunctivae and cornea of the eye and, with prolonged or repeated exposures, may affect vision. Quinone powder should be dampened to prevent dusting, and it should be handled in enclosed hoods or chambers fitted with LEV, by workers fitted with hand, arm, face and eye protection.
Heat and fire
The high temperature of the material (60 °C) involved in the manual hat-shaping process dictates the use of hand skin protection by the workers.
Fire is a common hazard during the early, dusty stages of felt manufacture. It may be caused by matches or sparks from metallic objects left in the waste wool, hot-running bearings or faulty electrical connections. It may also occur in finishing operations, when vapours of flammable solvents may collect in the drying ovens. Because it damages the material and corrodes the equipment, water is less popular for fire extinguishing than dry-powder extinguishers. Modern equipment is fitted with vents through which the extinguishing material can be sprayed, or with an automatic carbon dioxide releasing device.
Anthrax
Although rare, cases of anthrax have occurred as a result of exposure to contaminated wool imported from areas where this bacillus is endemic.
Synthetic Fibres
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Synthetic fibres are made from polymers that have been synthetically produced from chemical elements or compounds developed by the petrochemical industry. Unlike natural fibres (wool, cotton and silk), which date back to antiquity, synthetic fibres have a relatively short history dating back to the perfection of the viscose process in 1891 by Cross and Bevan, two British scientists. A few years later, rayon production started on a limited basis, and by the early 1900s, it was being produced commercially. Since then, a large variety of synthetic fibres has been developed, each designed with special characteristics that make it suitable for a particular kind of fabric, either alone or in combination with other fibres. Keeping track of them is made difficult by the fact that the same fibre may have different trade names in different countries.
The fibres are made by forcing liquid polymers through the holes of a spinneret to produce a continuous filament. The filament can be directly woven into cloth or, to give it the characteristics of natural fibres, it can, for example, be textured to add bulkiness, or it can be chopped into staple and spun.
Classes of Synthetic Fibres
The main classes of synthetic fibres used commercially include:
- Polyamides (nylons). The names of the long-chain polymeric amides are distinguished by a number which indicates the number of carbon atoms in their chemical constituents, the diamine being considered first. Thus, the original nylon produced from hexamethylene diamine and adipic acid is known in the United States and the United Kingdom as nylon 66 or 6.6, since both the diamine and the dibasic acid contain 6 carbon atoms. In Germany, it is marketed as Perlon T, in Italy as Nailon, in Switzerland as Mylsuisse, in Spain as Anid and in the Argentine as Ducilo.
- Polyesters. First introduced in 1941, polyesters are made by reacting ethylene glycol with terephthalic acid to form a plastic material made of long chains of molecules, which is pumped in molten form from spinnerets, allowing the filament to harden in cold air. A drawing or stretching process follows. Polyesters are known, for example, as Terylene in the UK, Dacron in the United States, Tergal in France, Terital and Wistel in Italy, Lavsan in the Russian Federation, and Tetoran in Japan.
- Polyvinyls. Polyacrylonitrile or acrylic fibre, first produced in 1948, is the most important member of this group. It is known under a variety of trade names: Acrilan and Orlon in the United States, Crylor in France, Leacril and Velicren in Italy, Amanian in Poland, Courtelle in the UK and so on.
- Polyolefins. The most common fibre in this group, known as Courlene in the UK, is made by a process similar to that for nylon. The molten polymer at 300 °C is forced through spinnerets and cooled in either air or water to form the filament. It is then drawn or stretched.
- Polypropylenes. This polymer, known as Hostalen in Germany, Meraklon in Italy and Ulstron in the UK, is melt spun, stretched or drawn, and then annealed.
- Polyurethanes. First produced in 1943 as Perlon D by the reaction of 1,4 butanediol with hexamethylene diisocyanate, the polyurethanes have become the basis of a new type of highly elastic fibre called spandex. These fibres are sometimes called snap-back or elastomeric on account of their rubber-like elasticity. They are manufactured from a linear polyurethane gum, which is cured by heating at very high temperatures and pressures to produce a “vulcanized” cross-linked polyurethane which is extruded as a monofil. The thread, which is widely used in garments requiring elasticity, can be covered by rayon or nylon to improve its appearance while the inner thread provides the “stretch”. Spandex yarns are known, for example, as Lycra, Vyrene and Glospan in the United States and Spandrell in the UK.
Special Processes
Stapling
Silk is the only natural fibre that comes in a continuous filament; other natural fibres come in short lengths or “staples”. Cotton has a staple of about 2.6 cm, wool of 6 to 10 cm and flax from 30 to 50 cm. The continuous synthetic filaments are sometimes passed through a cutting or stapling machine to produce short staples like the natural fibres. They can then be re-spun on cotton or wool spinning machines in order to produce a finish free of the glassy appearance of some synthetic fibres. During the spinning, combinations of synthetic and natural fibres or mixtures of synthetic fibres may be made.
Crimping
To give synthetic fibres the look and feel of wool, the twisted and tangled cut or stapled fibres are crimped by one of a number of methods. They may be passed through a crimping machine, in which hot, fluted rollers impart a permanent crimp. Crimping can also be done chemically, by controlling the coagulation of the filament so as to produce a fibre with an asymmetrical cross section (i.e., one side being thick-skinned and the other thin). When this fibre is wet, the thick side tends to curl, producing a crimp. To make crinkled yarn, known in the United States as non-torque yarn, the synthetic yarn is knitted into a fabric, set and then wound from the fabric by back-winding. The newest method passes two nylon threads through a heater, which raises their temperature to 180 °C and then passes them through a high-speed revolving spindle to impart the crimp. The spindles in the first machine ran at 60,000 revolutions per minute (rpm), but newer models have speeds of the order of 1.5 million rpm.
Synthetic Fibres for Work Clothes
The chemical resistance of polyester cloth makes the fabric particularly suitable for protective clothing for acid-handling operations. Polyolefin fabrics are suitable for protection against long exposures to both acids and alkalis. High-temperature-resistant nylon is well adapted for clothing to protect against fire and heat; it has good resistance at room temperature to solvents such as benzene, acetone, trichlorethylene and carbon tetrachloride. The resistance of certain propylene fabrics to a wide range of corrosive substances makes them suitable for work and laboratory clothing.
The light weight of these synthetic fabrics makes them preferable to the heavy rubberized or plastic-coated fabrics that would otherwise be required for comparable protection. They are also much more comfortable to wear in hot and humid atmospheres. In selecting protective clothing made from synthetic fibres, care should be taken to determine the generic name of the fibre and to verify such properties as shrinkage; sensitivity to light, dry-cleaning agents and detergents; resistance to oil, corrosive chemicals and common solvents; resistance to heat; and susceptibility to electrostatic charging.
Hazards and Their Prevention
Accidents
In addition to good housekeeping, which means keeping floors and passageways clean and dry to minimize slips and falls (vats must be leak proof and, where possible, have baffles to contain splashes), machines, drive belts, pulleys and shaftings must be properly guarded. Machines for spinning, carding, winding and warping operations should be fenced to keep materials and parts from flying out and to prevent workers’ hands from entering the dangerous zones. Lockout devices must be in place to prevent restart of machines while they are being cleaned or serviced.
Fire and explosion
The synthetic-fibres industry uses large amounts of toxic and flammable materials. Storage facilities for flammable substances should be out in the open or in a special fire-resistant structure, and they should be enclosed in bunds or dykes to localize spills. Automation of the delivery of toxic, flammable substances by a well-maintained system of pumps and pipes will reduce the hazard of moving and emptying containers. Appropriate fire-fighting equipment and clothing should be readily available and workers trained in their use through periodic drills, preferably conducted in concert with or under the observation of local fire-fighting authorities.
As the filaments emerge from the spinnerets to be dried in air or by means of spinning, large amounts of solvent vapours are released. These constitute a considerable toxic and explosion hazard and must be removed by LEV. Their concentration must be monitored to be sure that it remains below the solvent’s explosive limits. The exhausted vapours may be distilled and recovered for further use or they may be burned off; on no account should they be released into the general environmental atmosphere.
Where flammable solvents are used, smoking should be prohibited and open lights, flames and sparks eliminated. Electrical equipment should be of certified flameproof construction, and machines should be earthed (grounded) to prevent the build-up of static electricity, which might lead to catastrophic sparks.
Toxic hazards
Exposures to potentially toxic solvents and chemicals should be maintained below the relevant maximum allowable concentrations by adequate LEV. Respiratory protective equipment should be available for use by maintenance and repair crews and by workers charged with responding to emergencies caused by leaks, spillage and/or fire.
Viscose (Rayon)
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Rayon is a synthetic fibre produced from cellulose (wood pulp) that has been chemically treated. It is used alone or in blends with other synthetic or natural fibres to make fabrics that are strong, highly absorbent and soft, and which can be dyed in brilliant, long-lasting colours.
The manufacture of rayon had its origins in the quest for an artificial silk. In 1664, Robert Hooke, a British scientist noted for his observations of plant cells, predicted the possibility of duplicating silk by artificial means; almost two centuries later, in 1855, fibres were made from a mixture of mulberry twigs and nitric acid. The first successful commercial process was developed in 1884 by the French inventor Hilaire de Chardonnet, and in 1891, the British scientists Cross and Bevan perfected the viscose process. By 1895, rayon was being produced commercially on a rather small scale, and its use grew rapidly.
Production Methods
Rayon is made by a number of processes, depending on its intended use.
In the viscose process, cellulose derived from wood pulp is steeped in a sodium hydroxide solution, and the excess liquid is squeezed out by compression to form alkali cellulose. Impurities are removed and, after being torn into shreds similar to white crumbs that are allowed to age for several days at a controlled temperature, the shredded alkali cellulose is transferred to another tank where it is treated with carbon disulphide to form golden-orange crumbs of cellulose xanthate. These are dissolved in dilute sodium hydroxide to form a viscous orange liquid called viscose. Different batches of viscose are blended to obtain uniform quality. The mixture is filtered and ripened by several days of storage at rigidly controlled temperature and humidity. It is then extruded through metal nozzles with fine holes (spinnerets) into a bath of about 10% sulphuric acid. It can be wound as a continuous filament (cakes) or cut into the required lengths and spun like cotton or wool. Viscose rayon is used to make wearing apparel and heavy fabrics.
In the cuprammonium process, used to make silk-like fabrics and sheer hosiery, the cellulose pulp dissolved in the sodium hydroxide solution is treated with copper oxide and ammonia. The filaments come out of the spinnerets into a spinning funnel and are then stretched to the required fineness by the action of a jet stream of water.
In the viscose and cuprammonium processes, the cellulose is reconstituted, but acetate and triacetate are esters of the cellulose and are considered by some to be a separate class of fibre. Acetate fabrics are known for their ability to take brilliant colours and to drape well, features that make them particularly desirable for apparel. Short fibres of acetate are used as fillers in pillows, mattress pads and quilts. Triacetate yarns have many of the same properties as acetate but are particularly favoured for their ability to retain creases and pleats in garments.
Hazards and Their Prevention
The principal hazards in the viscose process are the exposures to carbon disulphide and hydrogen sulphide. Both have a variety of toxic effects depending on the intensity and duration of the exposure and the organ(s) affected; they range from fatigue and giddiness, respiratory irritation and gastrointestinal symptoms to profound neuropsychiatric disturbances, auditory and visual disorders, deep unconsciousness and death.
Moreover, with a flashpoint below –30 °C and explosive limits between 1.0 and 50%, carbon disulphide has a high risk of fire and explosion.
The acids and alkalis used in the process are fairly dilute, but there is always danger from the preparing of the proper dilutions and splashes into the eyes. The alkaline crumbs produced during the shredding process may irritate workers’ hands and eyes, while the acid fumes and hydrogen sulphide gas emanating from the spinning bath may cause a kerato-conjunctivitis characterized by excessive lachrimation, photophobia and severe ocular pain.
Keeping the concentrations of carbon disulphide and hydrogen sulphide below the safe exposure limits requires diligent monitoring such as may be provided by an automatic continuous recording apparatus. Complete enclosure of the machinery with efficient LEV (with intakes at floor levels since these gases are heavier than air) is advisable. Workers must be trained in emergency responses in the event of leaks, and, in addition to being provided with proper personal protective equipment, maintenance and repair workers must be carefully schooled and supervised to avoid unnecessary levels of exposure.
Rest rooms and washing up facilities are necessities rather than mere amenities. Medical surveillance through preplacement and periodic medical examinations is desirable.
Silk Industry
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Silk is a lustrous, tough, elastic fibre produced by the larvae of silkworms; the term also covers the thread or cloth made from this fibre. The silk industry originated in China, as early as 2640 BC according to tradition. Towards the 3rd century AD, knowledge of the silkworm and its product reached Japan through Korea; it probably spread to India a little later. From there silk production was slowly carried westward through Europe to the New World.
The production process involves a sequence of steps not necessarily carried out in a single enterprise or plant. They include:
- Sericulture. The production of cocoons for their raw silk filament is known as sericulture, a term which covers feeding, cocoon formation and so on. The first essential is a stock of mulberry trees adequate to feed the worms in their larval state. The trays on which the worms are reared have to be kept in a room with a constant temperature of 25 °C; this involves artificial heating in colder countries and seasons. The cocoons are spun after about 42 days of feeding.
- Spinning or filature. The distinctive process in silk spinning is called reeling, in which the filaments from the cocoon are formed into a continuous, uniform and regular strand. First, the natural gum (sericin) is softened in scalding water. Then, in a bath or basin of hot water, the ends of the filaments from several cocoons are caught together, drawn up, attached to a reeling wheel and wound to form raw silk.
- Throwing. In this process, the threads are twisted and doubled into more substantial yarns.
- Degumming. In this phase, the raw silk is boiled in a solution of soap and water at approximately 95 °C.
- Bleaching. The raw or boiled silk is then bleached in hydrogen peroxide or sodium peroxide.
- Weaving. The silk thread is next woven into fabric; this usually takes place in separate factories.
- Dyeing. Silk may be dyed while in the filament or thread form, or it may be dyed as a fabric.
Health and Safety Hazards
Carbon monoxide
Symptoms of carbon monoxide toxicity consisting of headache, vertigo and sometimes nausea and vomiting, usually not severe, have been reported in Japan, where sericulture is a common home industry, as a result of the use of charcoal fires in poorly ventilated rearing rooms.
Dermatitis
Mal des bassines, a dermatitis of the hands of female workers reeling raw silk, was quite common, particularly in Japan, where, in the 1920s, a morbidity rate of 30 to 50% among reeling workers was reported. Fourteen per cent of the affected workers lost an average of three working days each year. The skin lesions, localized mainly on fingers, wrists and forearms, were characterized by erythema covered with small vesicles which became chronic, pustular or eczematous and extremely painful. The cause of this condition was usually attributed to the decomposition products of the dead chrysalis and to a parasite in the cocoon.
More recently, however, Japanese observations have showed that it is probably related to the temperature of the reeling bath: until 1960 almost all reeling baths were kept at 65 °C, but, since the introduction of new installations with a bath temperature of 30 to 45 °C, there have been no reports of the typical skin lesions among reel workers.
The handling of raw silk may produce allergic skin reactions in some reel workers. Facial swelling and ocular inflammation have been observed where there was no direct local contact with the reeling bath. Similarly, dermatitis has been found among silk throwers.
Respiratory tract problems
In the former Soviet Union, an unusual outbreak of tonsillitis among silk spinners was traced to bacteria in the water of reeling basins and in the ambient air of the cocoon department. Disinfection and frequent replacement of reel bath water, combined with exhaust ventilation at the cocoon reels, brought about a swift improvement.
Extensive long-term epidemiological observations also carried out in the former USSR have shown that workers in the natural silk industry may develop respiratory allergy featuring bronchial asthma, asthmatiform bronchitis and/or allergic rhinitis. It appears that natural silk can cause sensitization during all stages of production.
A situation causing respiratory distress among spinning-frame workers when packaging or repackaging silk on a spinning or winding frame has also been reported. Depending upon the speed of the machinery, it is possible to aerosolize the proteinaceous substance surrounding the silk filament. This aerosol, when respirable in size, will cause a lung reaction very similar to that of the byssinotic reaction to cotton dust.
Noise
Noise exposure can reach harmful levels for workers at machines spinning and winding the silk threads, and at looms where fabric is woven. Adequate lubrication of the equipment and the interposition of sound baffles may reduce the noise level somewhat, but the continuing exposure throughout the working day can have a cumulative effect. If effective abatement is not obtained, resort will have to be made to personal protective devices. As with all workers exposed to noise, a hearing protection programme featuring periodic audiograms is desirable.
Safety and Health Measures
Control of temperature, humidity and ventilation are important at all stages of the silk industry. Home workers should not escape supervision. Adequate ventilation of rearing rooms should be ensured, and charcoal or kerosene stoves should be replaced by electric heaters or other warming devices.
Lowering the temperature of reeling baths may be effective in preventing dermatitis. The water should be replaced frequently, and exhaust ventilation is desirable. Direct skin contact with raw silk immersed in reeling baths should be avoided as far as possible.
The provision of good sanitary facilities and attention to personal hygiene are essential. Hand washing with a 3% acetic acid solution has been found effective in Japan.
The medical examination of new entrants and medical supervision thereafter are desirable.
The hazards from machinery in silk manufacture are similar to those in the textile industry in general. Accident prevention is best achieved by good housekeeping, adequate guarding of moving parts, continuing worker training and effective supervision. Power looms should be provided with guards to prevent accidents from flying shuttles. Very good lighting is required for the yarn preparation and weaving processes.
Wool Industry
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
The origins of the wool industry are lost in antiquity. Sheep were easily domesticated by our remote ancestors and were important in satisfying their basic needs for food and clothing. Early human societies rubbed together the fibres collected from the sheep to form a yarn, and from this basic principle the processes of manipulating the fibre have increased in complexity. The wool textile industry has been in the forefront in developing and adapting mechanical methods and was therefore one of the early industries in the development of the factory system of production.
Raw Materials
The length of fibre when taken from the animal is the dominant, but not the only, factor determining how it is processed. The type of wool available may be broadly classified into (a) merino or botany, (b) crossbreds—fine, medium or coarse and (c) carpet wools. Within each group, however, there are various grades. Merino usually has the finest diameter and a short length, while the carpet wools are long-fibred, with a coarser diameter. Today, increasing quantities of synthetic fibres simulating wool are blended with the natural fibre and are processed in the same manner. Hair from other animals—for example, mohair (goat), alpaca (llama), cashmere (goat, camel), angora (goat) and vicuña (wild llama)—also plays an important, although subsidiary, role in the industry; it is relatively expensive and is usually processed by specialized firms.
Production
The industry has two distinctive processing systems—woollen and the worsted. The machinery is in many ways similar, but the purposes are distinct. In essence, the worsted system uses the longer stapled wools and in the carding, preparing, gilling and combing processes the fibres are kept parallel and the shorter fibres are rejected. Spinning produces a strong yarn of fine diameter, which then is woven to yield a light fabric with the familiar smooth and firm appearance of men’s suits. In the woollen system, the aim is to intermingle and intertwine the fibres to form a soft and fluffy yarn, which is woven to give a cloth of full and bulky character with a “woolly” surface—for example, tweeds, blankets and heavy overcoatings. Since uniformity of fibre is not necessary in the woollen system, the manufacturer can blend together new wool, shorter fibres rejected by the worsted process, wools recovered from tearing up old wool garments and so on; “shoddy” is obtained from soft, and “mungo” from hard waste material.
It should be borne in mind, however, that the industry is particularly complex and that the condition and type of the raw material used and the specification for the finished cloth will influence the method of processing at each stage and the sequence of those stages. For example, wool may be dyed before processing, at the yarn stage or towards the end of the process when in the woven piece. Moreover, some of the processes may be carried on in separate establishments.
Hazards and Their Prevention
As in every section of the textile industry, large machines with rapidly moving parts pose both noise and mechanical injury hazards. Dust can also be a problem. The highest practicable form of guarding or enclosure should be provided for such generic parts of the equipment as spur gear wheels, chains and sprockets, revolving shafting, belts and pulleys, and for the following parts of machinery used specifically in the wool textile trade:
- feed rollers and swifts of various types of preparatory opening machines (e.g., teasers, willeys, garnetts, rag-grinding machines and so on)
- licker-in or taker-in and adjacent rollers of scribbling and carding machines
- intake between swift and doffer cylinders of scribbling, carding and garnetting machines
- rollers and fallers of gill-boxes
- back shafts of drawing and roving frames
- traps between the carriage and headstock of mules
- projecting pins, bolts and other securing devices used on the beaming-off motion of warping machines
- squeeze rollers of scouring, milling and cloth-wringing machines
- intake between cloth and wrapper and roller of blowing machines
- revolving-knife cylinder of cropping machines
- blades of fans in pneumatic conveying systems (any inspection panel in the ducting of such a system should be at a safe distance from the fan, and the worker should have indelibly impressed on his or her memory the length of time it takes for the machine to slow and come to a stop after the power has been cut off; this is particularly important since the worker clearing a blockage in the system usually cannot see the moving blades)
- the flying shuttle, which presents a special problem (looms should be provided with well-designed guards to prevent the shuttle from flying out of the shed and to limit the distance it might travel should it fly).
The guarding of such dangerous parts presents practical problems. The design of the guard should take into account the working practices connected with the particular process and particularly should preclude possible removal of the guard when the operator is at the greatest risk (e.g., lockout arrangements). Special training and close supervision are required to prevent waste removal and cleaning while machinery is in motion. Much of the responsibility devolves on machinery manufacturers, who should ensure that such safety features are incorporated into new machines at the design stage, and on supervisory personnel, who should ensure that workers are adequately trained in safe handling of equipment.
Spacing of machinery
The risk of accidents is increased if insufficient space is allowed between the machines. Many older premises squeezed the maximum number of machines into the available floor area, thereby reducing the space available for aisles and passageways and for the temporary storage of raw and finished materials within the workroom. In some old mills, the gangways between the carding machines are so narrow that enclosure of the driving belts within a guard is impracticable and recourse has to be made to “wedge” guarding between the belt and the pulley at the in-running point; a well-made and smooth belt fastener is particularly important in these circumstances. Minimum spacing standards, as recommended by a British Government committee for certain wool textile machinery, are required.
Materials handling
When modern mechanical load-handling methods are not employed, there remains the risk of injury from the lifting of heavy loads. Materials handling should be mechanized to the fullest extent possible. Where this is not available, the precautions discussed elsewhere in this Encyclopaedia should be employed. Proper lifting technique is particularly important for workers who manipulate heavy beams into and out of looms or who handle heavy and cumbersome bales of wool in the early preparatory processes. Wherever possible, hand-trucks and movable carts or skids should be used to move such bulky and heavy loads.
Fire
Fire is a serious hazard, especially in old multistorey mills. The mill structure and layout should conform to local regulations governing unobstructed gangways and exits, fire-alarm systems, fire extinguishers and hoses, emergency lights and so on. Cleanliness and good housekeeping will prevent accumulations of dust and fluff, which encourage the spread of fire. No repairs involving the use of flame cutting or flame-burning equipment should be carried on during working hours. Training of all staff in procedures in case of fire are necessary; fire drills, conducted if possible in concert with local fire, police and emergency medical services, should be practised at appropriate intervals.
General safety
Emphasis has been placed on those accident situations which are especially to be found in the wool textile industry. However, it should be noted that the majority of accidents in mills occur in circumstances that are common to all factories—for example, falls of persons and objects, handling of goods, use of hand tools and so on—and that the relevant fundamental safety principles to be followed apply no less in the wool industry than in most other industries.
Health Problems
Anthrax
The industrial disease usually associated with wool textiles is anthrax. It was at one time a great danger, particularly to wool sorters, but has been almost completely controlled in the wool textile industry as a result of:
- improvements in production methods in exporting countries where anthrax is endemic
- disinfection of materials liable to be carrying anthrax spores
- improvements in handling the possibly infected material under exhaust ventilation in the preparatory processes
- microwaving the wool bale sufficiently long to a temperature that will kill any fungi. This treatment also assists in the recovery of lanolin associated with the wool.
- significant advances in medical treatment, including immunization of workers in high-risk situations
- education and training of workers and the provision of washing facilities and, when necessary, personal protective equipment.
Besides anthrax fungal spores, it is known that spores of the fungus Coccidiodes immitis can be found in wool, especially from the southwestern United States. This fungus can cause the disease known as coccidioidomycosis, which, along with the respiratory disease from anthrax, usually has a poor prognosis. Anthrax has the added hazard of causing a malignant ulcer or carbuncle with a black centre when entering the body through a break in the skin barrier.
Chemical substances
Various chemicals are used—for example, for degreasing (diethylene dioxide, synthetic detergents, trichloroethylene and, in the past, carbon tetrachloride), disinfection (formaldehyde), bleaching (sulphur dioxide, chlorine) and dyeing (potassium chlorate, anilines). The risks include gassing, poisoning, irritation of the eyes, mucous membranes and lungs, and skin conditions. In general, prevention relies on:
- substitution of a less dangerous chemical
- local exhaust ventilation
- care in labelling, storage and transport of corrosive or noxious liquids
- personal protective equipment
- good washing facilities (including shower baths where practicable)
- strict personal hygiene.
Other hazards
Noise, inadequate lighting, and the high temperatures and humidity levels required for wool processing may have a deleterious effect on general health unless they are strictly controlled. In many countries, standards are prescribed. Steam and condensation may be difficult to control effectively in dyeing sheds, and expert engineering advice is often needed. In weaving sheds, noise control presents a serious problem on which much work remains to be done. A high standard of lighting is necessary everywhere, particularly where dark fabrics are being manufactured.
Dust
As well as the specific risk of anthrax spores in the dust produced in the earlier processes, dust in high quantities sufficient to induce irritation of the respiratory tract mucosae is produced at many machines, especially those with a tearing or carding action, and should be removed by effective LEV.
Noise
With all the moving parts in the machinery, particularly the looms, woollen mills are often very noisy places. While attenuation can be achieved by proper lubrication, the introduction of sound baffles and other engineering approaches should be considered as well. By and large, prevention of occupational hearing loss depends on the workers’ use of ear plugs or muffs. It is essential that workers be trained in the proper use of such protective equipment and supervised to verify that they are using it. A hearing conservation programme with periodic audiograms is required in many countries. As equipment is replaced or repaired, appropriate noise-reduction steps should be taken.
Work stress
Work stress, with its attendant effects on workers’ health and well-being, is a common problem in this industry. Since many of the mills operate around the clock, shift work is frequently required. To meet the production quotas, the machines operate continuously, with each worker being “tied” to one or more pieces of equipment and unable to leave it for bathroom or rest breaks until a “floater” has taken his or her place. Coupled with the ambient noise and use of noise protectors, their heavily routinized, repetitive activity makes for de facto isolation of the workers and a lack of social interaction that many find stressful. The quality of supervision and the availability of workplace amenities have a great influence on workers’ job stress levels.
Conclusion
While larger enterprises are able to invest in new technological developments, many smaller and older mills continue to operate in old plants with out-dated but still functioning equipment. Economic imperatives dictate less rather than greater attention to workers’ safety and health. Indeed, in many developed areas, mills are being abandoned in favour of new plants in developing countries and areas where cheaper labour is readily available and where health and safety regulations are either non-existent or are generally ignored. Worldwide, this is an important labour-intensive industry in which reasonable investments to workers’ health and well-being can bring significant dividends to both the enterprise and its workforce.
Cotton Yarn Manufacturing
Cotton accounts for almost 50% of the worldwide consumption of textile fibre. China, the United States, the Russian Federation, India and Japan are the major cotton-consuming countries. Consumption is measured by the amount of raw cotton fibre purchased and used to manufacture textile materials. Worldwide cotton production is annually about 80 to 90 million bales (17.4 to 19.6 billion kg). China, the United States, India, Pakistan and Uzbekistan are the major cotton-producing countries, accounting for over 70% of world cotton production. The rest is produced by about 75 other countries. Raw cotton is exported from about 57 countries and cotton textiles from about 65 countries. Many countries emphasize domestic production to reduce their reliance on imports.
Yarn manufacturing is a sequence of processes that convert raw cotton fibres into yarn suitable for use in various end-products. A number of processes are required to obtain the clean, strong, uniform yarns required in modern textile markets. Beginning with a dense package of tangled fibres (cotton bale) containing varying amounts of non-lint materials and unusable fibre (foreign matter, plant trash, motes and so on), continuous operations of opening, blending, mixing, cleaning, carding, drawing, roving and spinning are performed to transform the cotton fibres into yarn.
Even though the current manufacturing processes are highly developed, competitive pressure continues to spur industry groups and individuals to seek new, more efficient methods and machines for processing cotton which, one day, may supplant today’s systems. However, for the foreseeable future, the current conventional systems of blending, carding, drawing, roving and spinning will continue to be used. Only the cotton picking process seems clearly destined for elimination in the near future.
Yarn manufacturing produces yarns for various woven or knitted end-products (e.g., apparel or industrial fabrics) and for sewing thread and cordage. Yarns are produced with different diameters and different weights per unit length. While the basic yarn manufacturing process has remained unchanged for a number of years, processing speeds, control technology and package sizes have increased. Yarn properties and processing efficiency are related to the properties of the cotton fibres processed. End-use properties of the yarn are also a function of processing conditions.
Yarn Manufacturing Processes
Opening, blending, mixing and cleaning
Typically, mills select bale mixes with the properties needed to produce yarn for a specific end-use. The number of bales used by different mills in each mix ranges from 6 or 12 to over 50. Processing begins when the bales to be mixed are brought to the opening room, where bagging and ties are removed. Layers of cotton are removed from the bales by hand and placed in feeders equipped with conveyors studded with spiked teeth, or entire bales are placed on platforms which move them back and forth under or over a plucking mechanism. The aim is to begin the sequential production process by converting the compacted layers of baled cotton into small, light, fluffy tufts that will facilitate the removal of foreign matter. This initial process is referred to as “opening”. Since bales arrive at the mill in various degrees of density, it is common for bale ties to be cut approximately 24 hours before the bales are to be processed, in order to allow them to “bloom”. This enhances opening and helps regulate the feeding rate. The cleaning machines in mills perform the functions of opening and first-level cleaning.
Carding and combing
The card is the most important machine in the yarn manufacturing process. It performs second- and final-level cleaning functions in an overwhelming majority of cotton textile mills. The card is composed of a system of three wire-covered cylinders and a series of flat, wire-covered bars that successively work small clumps and tufts of fibres into a high degree of separation or openness, remove a very high percentage of trash and other foreign matter, collect the fibres into a rope-like form called a “sliver” and deliver this sliver in a container for use in the subsequent process (see figure 1).
Figure 1. Carding
Wilawan Juengprasert, Ministry of Public Health, Thailand
Historically, cotton has been fed to the card in the form of a “picker lap”, which is formed on a “picker”, a combination of feed rolls and beaters with a mechanism made up of cylindrical screens on which opened tufts of cotton are collected and rolled into a batt (see figure 2). The batt is removed from the screens in an even, flat sheet and then is rolled into a lap. However, labour requirements and the availability of automated handling systems with the potential for improved quality are contributing to the obsolescence of the picker.
Figure 2. A modern picker
Wilawan Juengprasert, Ministry of Public Health, Thailand
The elimination of the picking process has been made possible by the installation of more efficient opening and cleaning equipment and chute-feed systems on the cards. The latter distribute opened and cleaned tufts of fibres to cards pneumatically through ducts. This action contributes to processing consistency and improved quality and reduces the number of workers required.
A small number of mills produce combed yarn, the cleanest and most uniform cotton yarn. Combing provides more extensive cleaning than is provided by the card. The purpose of combing is to remove short fibres, neps and trash so that the resulting sliver is very clean and lustrous. The comber is a complicated machine composed of grooved feed rolls and a cylinder that is partially covered with needles to comb out short fibres (see figure 3).
Figure 3. Combing

Wilawan Juengprasert, Ministry of Public Health, Thailand
Drawing and roving
Drawing is the first process in yarn manufacturing that employs roller drafting. In drawing, practically all draft results from the action of rollers. Containers of sliver from the carding process are staked in the creel of the drawing frame. Drafting occurs when a sliver is fed into a system of paired rollers moving at different speeds. Drawing straightens the fibres in the sliver by drafting to make more of the fibres parallel to the axis of the sliver. Parallelization is necessary to obtain the properties desired when the fibres are subsequently twisted into yarn. Drawing also produces a sliver that is more uniform in weight per unit of length and helps to achieve greater blending capabilities. The fibres that are produced by the final drawing process, called finisher drawing, are nearly straight and parallel to the axis of the sliver. Weight per unit length of a finisher-drawing sliver is too high to permit drafting into yarn on conventional ring-spinning systems.
The roving process reduces the weight of the sliver to a suitable size for spinning into yarn and inserting twist, which maintains the integrity of the draft strands. Cans of slivers from finisher drawing or combing are placed in the creel, and individual slivers are fed through two sets of rollers, the second of which rotates faster, thus reducing the size of the sliver from about 2.5 cm in diameter to that of the diameter of a standard pencil. Twist is imparted to the fibres by passing the bundle of fibres through a roving “flyer”. The product is now called “roving”, which is packaged on a bobbin about 37.5 cm long with a diameter of about 14 cm.
Spinning
Spinning is the single most costly step in converting cotton fibres to yarn. Currently, over 85% of the world’s yarn is produced on ring-spinning frames, which are designed to draft the roving into the desired yarn size, or count, and to impart the desired amount of twist. The amount of twist is proportional to the strength of the yarn. The ratio of the length to the length fed can vary on the order of 10 to 50. Bobbins of roving are placed onto holders that allow the roving to feed freely into the drafting roller of the ring-spinning frame. Following the drafting zone, the yarn passes through a “traveller” onto a spinning bobbin. The spindle holding this bobbin rotates at high speed, causing the yarn to balloon as twist is imparted. The lengths of yarn on the bobbins are too short for use in subsequent processes and are doffed into “spinning boxes” and delivered to the next process, which may be spooling or winding.
In the modern production of heavier or coarse yarns, open-end spinning is replacing ring spinning. A sliver of fibres is fed into a high-speed rotor. Here the centrifugal force converts the fibres into yarns. There is no need for the bobbin, and the yarn is taken up on the package required by the next step in the process.
Considerable research and development efforts are being devoted to radical new methods of yarn production. A number of new spinning systems currently under development may revolutionize yarn manufacturing and could cause changes in the relative importance of fibre properties as they are now perceived. In general, four of the different approaches used in the new systems appear practical for use on cotton. Core-spun systems are currently in use to produce a variety of specialty yarns and sewing threads. Twistless yarns have been produced commercially on a limited basis by a system that bonds the fibres together with a polyvinyl alcohol or some other bonding agent. The twistless yarn system offers potentially high production rates and very uniform yarns. Knit and other apparel fabrics from twistless yarn have excellent appearance. In air-vortex spinning, currently under study by several machinery manufacturers, drawing sliver is presented to an opening roller, similar to rotor spinning. Air-vortex spinning is capable of very high production speeds, but prototype models are particularly sensitive to fibre length variations and foreign matter content such as trash particles.
Winding and spooling
Once the yarn is spun, the manufacturers must prepare a correct package. The type of package depends on whether the yarn will be used for weaving or knitting. Winding, spooling, twisting and quilling are considered preparatory steps for weaving and knitting yarn. In general, the product of spooling will be used as warp yarns (the yarns that run lengthwise in woven fabric) and the product of winding will be used as filling yarns, or weft yarns (the yarns that run across the fabric). The products from open-end spinning by-pass these steps and are packaged for either the filling or warp. Twisting produces ply yarns, where two or more yarns are twisted together before further processing. In the quilling process yarn is wound onto small bobbins, small enough to fit inside the shuttle of a box loom. Sometimes the quilling process takes place at the loom. (See also the article “Weaving and knitting” in this chapter.)
Waste handling
In modern textile mills where control of dust is important, the handling of waste is given greater emphasis. In classical textile operations, waste was collected manually and delivered to a “wastehouse” if it could not be recycled into the system. Here it was accumulated until there was enough of one type to make a bale. In the present state of the art, central vacuum systems automatically return waste from opening, picking, carding, drawing and roving. The central vacuum system is used for cleaning of machinery, automatically collecting waste from under machinery such as fly and motes from carding, and for returning unusable floor sweeps and wastes from filter condensers. The classical baler is a vertical upstroke press which still forms a typical 227-kg bale. In modern wastehouse technology, wastes are accumulated from the central vacuum system in a receiving tank which feeds a horizontal bale press. The various waste products of the yarn manufacturing industry can be recycled or reused by other industries. For example, spinning can be used in the waste spinning industry to make mop yarns, garnetting can be used in the cotton batting industry to make batting for mattresses or upholstered furniture.
Safety and Health Concerns
Machinery
Accidents may occur on all types of cotton textile machinery, though the frequency rate is not high. Effective guarding of the multiplicity of moving parts presents many problems and needs constant attention. Training of operators in safe practices is also essential, in particular to avoid attempting repairs while the machinery is in motion, the cause of many of the accidents.
Each piece of machinery may have sources of energy (electrical, mechanical, pneumatic, hydraulic, inertial and so on) that need to be controlled before any repair or maintenance work is attempted. The facility should identify energy sources, provide necessary equipment and train personnel to ensure that all hazardous energy sources are turned off while working on equipment. An inspection should be performed on a regular basis to ensure that all lockout/tagout procedures are being followed and correctly applied.
Cotton dust inhalation (byssinosis)
Inhalation of the dust generated where cotton fibre is converted into yarn and fabric has been shown to cause an occupational lung disease, byssinosis, in a small number of textile workers. It usually takes 15 to 20 years of exposure to higher levels of dust (above 0.5 to 1.0 mg/m3) for workers to become reactors. OSHA and the American Conference of Governmental Industrial Hygienists (ACGIH) standards set 0.2 mg/m3 respirable cotton dust as measured by the vertical elutriator as the limit for occupational exposure to cotton dust in textile yarn manufacturing. The dust, an airborne particulate released into the atmosphere as cotton is handled or processed, is a heterogeneous, complex mixture of botanical trash, soil and microbiological material (i.e., bacteria and fungi), which varies in composition and biological activity. The aetiological agent and pathogenesis of byssinosis are not known. Cotton plant trash associated with the fibre and the endotoxin from gram-negative bacteria on the fibre and plant trash are thought to be the cause or to contain the causative agent. The cotton fibre itself, which is mainly cellulose, is not the cause, since cellulose is an inert dust that does not cause respiratory disease. Appropriate engineering controls in cotton textile processing areas (see figure 4) along with work practices, medical surveillance and PPE can, for the most part, eliminate the byssinosis. A mild water washing of cotton by batch kier washing systems and continuous batt systems reduces the residual level of endotoxin in both lint and airborne dust to levels below those associated with the acute reduction in pulmonary function as measured by the 1-second forced expiratory volume.
Figure 4. Dust extraction system for a carding machine
Noise
Noise can be a problem in some processes in yarn manufacturing, but in a few modern textile mills the levels are below 90 dBA, which is the US standard but which exceeds noise exposure standards in many countries. Thanks to the abatement efforts of machinery manufacturers and industrial noise engineers, noise levels are continuing to decrease as machinery speeds increase. The solution for high noise levels is the introduction of more modern, quieter equipment. In the United States, a hearing conservation programme is required when noise levels exceed 85 dBA; this would include noise-level monitoring, audiometric testing and making hearing protection available to all employees when noise levels cannot be engineered below 90 dBA.
Heat stress
Since spinning sometimes requires high temperatures and artificial humidificaton of the air, careful monitoring attention is always necessary to ensure that permissible limits are not exceeded. Well designed and maintained air-conditioning plants are increasingly used in place of more primitive methods of temperature and humidity regulation.
Occupational safety and health management systems
Many of the more modern textile yarn manufacturing mills find it useful to have some type of occupational safety and health management system in place to control the workplace hazards that workers may encounter. This can be a voluntary programme like the “Quest for the Best in Health and Safety” developed by the American Textile Manufacturers Institute, or one that is mandated by regulations such as the US State of California Occupational Injury and Illness Prevention Program (Title 8, California Code of Regulations, Section 3203). When a safety and health management system is used, it should be flexible and adaptable enough to allow the mill to tailor it to its own needs.
Production and Ginning of Cotton
Cotton Production
Cotton production practices begin after the previous crop is harvested. The first operations usually include shredding stalks, ripping out roots and disking the soil. Fertilizer and herbicides generally are applied and incorporated into the soil before the land is bedded in preparation for needed irrigation or planting. Since soil characteristics and past fertilization and cropping practices can cause a wide range of fertility levels in cotton soils, fertility programmes should be based on soil test analyses. Control of weeds is essential to obtain high lint yield and quality. Cotton yields and harvesting efficiency can be reduced by as much as 30% by weeds. Herbicides have been widely used in many countries for weed control since the early 1960s. Application methods include pre-planting treatment to foliage of existing weeds, incorporation into pre-plant soil and treatment at pre-emergence and post-emergence stages.
Several factors that play an important role in achieving a good stand of cotton plants include seed-bed preparation, soil moisture, soil temperature, seed quality, seedling disease infestation, fungicides and soil salinity. Planting high-quality seed in a well-prepared seed-bed is a key factor in achieving early, uniform stands of vigorous seedlings. High-quality planting seed should have a germination rate of 50% or higher in a cool test. In a cool/warm test, the seed vigour index should be 140 or higher. Seeding rates of 12 to 18 seeds/metre of row are recommended to obtain a plant population of 14,000 to 20,000 plants/hectare. A suitable planter metering system should be used to ensure uniform spacing of seed regardless of seed size. Seed germination and seedling emergence rates are closely associated with a temperature range of 15 to 38 ºC.
Early-season seedling diseases can hamper uniform stands and result in the need to replant. Important seedling disease pathogens such as Pythium, Rhizoctonia, Fusarium and Thielaviopsis can reduce plant stands and cause long skips between seedlings. Only seed that has been properly treated with one or more fungicides should be planted.
Cotton is similar to other crops with respect to water use during different plant developmental stages. Water use is generally less than 0.25 cm/day from emergence to the first square. During this period, loss of soil moisture by evaporation may exceed the amount of water transpired by the plant. Water use increases sharply as the first blooms appear and reaches a maximum level of 1 cm/day during the peak bloom stage. Water requirement refers to the total amount of water (rainfall and irrigation) needed to produce a crop of cotton.
Insect populations can have an important impact on cotton quality and yield. Early-season population management is important in promoting balanced fruiting/vegetative development of the crop. Protecting early fruit positions is essential to achieving a profitable crop. Over 80% of the yield is set in the first 3 to 4 weeks of fruiting. During the fruiting period, producers should scout their cotton at least twice a week to monitor insect activity and damage.
A well-managed defoliation programme reduces leaf trash that can adversely affect the grade of the harvested cotton. Growth regulators such as PIX are useful defoliators because they control vegetative growth and contribute to earlier fruiting.
Harvesting
Two types of mechanical harvesting equipment are used to harvest cotton: the spindle picker and the cotton stripper. The spindle picker is a selective-type harvester that uses tapered, barbed spindles to remove seed cotton from bolls. This harvester can be used on a field more than once to provide stratified harvests. On the other hand, the cotton stripper is a nonselective or once-over harvester that removes not only the well-opened bolls but also the cracked and unopened bolls along with the burs and other foreign matter.
Agronomic practices that produce a high-quality uniform crop will generally contribute to good harvesting efficiency. The field should be well drained and rows laid out for effective use of machinery. Row ends should be free of weeds and grass, and should have a field border of 7.6 to 9 m for turning and aligning the harvesters with the rows. The border also should be free of weeds and grass. Disking creates adverse conditions in rainy weather, so chemical weed control or mowing should be used instead. Plant height should not exceed about 1.2 m for cotton that is to be picked, and about 0.9 m for cotton that is to be stripped. Plant height can be controlled to some extent by using chemical growth regulators at the proper growth stage. Production practices that set the bottom boll at least 10 cm above the ground should be used. Culturing practices such as fertilization, cultivation and irrigation during the growing season should be carefully managed to produce a uniform crop of well-developed cotton.
Chemical defoliation is a culturing practice that induces abscission (shedding) of foliage. Defoliants may be applied to help minimize green-leaf-trash contamination and promote faster drying of early morning dew on the lint. Defoliants should not be applied until at least 60% of the bolls are open. After a defoliant is applied, the crop should not be harvested for at least 7 to 14 days (the period will vary depending on chemicals used and weather conditions). Chemical desiccants may also be used to prepare plants for harvest. Desiccation is the rapid loss of water from the plant tissue and subsequent death of the tissue. The dead foliage remains attached to the plant.
The current trend in cotton production is toward a shorter season and one-time harvest. Chemicals that accelerate the boll opening process are applied with the defoliant or soon after the leaves drop. These chemicals allow earlier harvests and increase the percentage of bolls that are ready to be harvested during the first harvest. Because these chemicals have the ability to open or partially open immature bolls, the quality of the crop may be severely impacted (i.e., the micronaire may be low) if the chemicals are applied too early.
Storage
The moisture content of cotton before and during storage is critical; excess moisture causes stored cotton to overheat, resulting in lint discolouration, lower seed germination and possibly spontaneous combustion. Seed cotton with a moisture content above 12% should not be stored. Also, the internal temperature of newly built modules should be monitored for the first 5 to 7 days of cotton storage; modules that experience a 11 ºC rise or are above 49 ºC should be ginned immediately to avoid the possibility of major loss.
Several variables affect seed and fibre quality during seed cotton storage. Moisture content is the most important. Other variables include length of storage, amount of high-moisture foreign matter, variation in moisture content throughout the stored mass, initial temperature of the seed cotton, temperature of the seed cotton during storage, weather factors during storage (temperature, relative humidity, rainfall) and protection of the cotton from rain and wet ground. Yellowing is accelerated at high temperatures. Both temperature rise and maximum temperature are important. Temperature rise is directly related to the heat generated by biological activity.
Ginning process
About 80 million bales of cotton are produced annually worldwide, of which about 20 million are produced by about 1,300 gins in the United States. The principal function of the cotton gin is to separate lint from seed, but the gin must also be equipped to remove a large percentage of the foreign matter from the cotton that would significantly reduce the value of the ginned lint. A ginner must have two objectives: (1) to produce lint of satisfactory quality for the grower’s market and (2) to gin the cotton with minimum reduction in fibre spinning quality, so that the cotton will meet the demands of its ultimate users, the spinner and the consumer. Accordingly, quality preservation during ginning requires the proper selection and operation of each machine in a ginning system. Mechanical handling and drying may modify the natural quality characteristics of cotton. At best, a ginner can only preserve the quality characteristics inherent in the cotton when it enters the gin. The following paragraphs briefly discuss the function of the major mechanical equipment and processes in the gin.
Seed-cotton machinery
Cotton is transported from a trailer or module into a green-boll trap in the gin, where green bolls, rocks and other heavy foreign matter are removed. The automatic feed control provides an even, well-dispersed flow of cotton so that the gin’s cleaning and drying system will operate more efficiently. Cotton that is not well dispersed can travel through the drying system in clumps, and only the surface of that cotton will be dried.
In the first stage of drying, heated air conveys the cotton through the shelves for 10 to 15 seconds. The temperature of the conveying air is regulated to control the amount of drying. To prevent fibre damage, the temperature to which the cotton is exposed during normal operation should never exceed 177 ºC. Temperatures above 150 ºC can cause permanent physical changes in cotton fibres. Dryer-temperature sensors should be located as near as possible to the point where cotton and heated air come together. If the temperature sensor is located near the exit of the tower dryer, the mixpoint temperature could actually be 55 to 110 ºC higher than the temperature at the downstream sensor. The temperature drop downstream results from the cooling effect of evaporation and from heat loss through the walls of machinery and piping. The drying continues as the warm air moves the seed cotton to the cylinder cleaner, which consists of 6 or 7 revolving spiked cylinders that rotate at 400 to 500 rpm. These cylinders scrub the cotton over a series of grid rods or screens, agitate the cotton and allow fine foreign materials, such as leaves, trash and dirt, to pass through the openings for disposal. Cylinder cleaners break up large wads and generally condition the cotton for additional cleaning and drying. Processing rates of about 6 bales per hour per metre of cylinder length are common.
The stick machine removes larger foreign matter, such as burs and sticks, from the cotton. Stick machines use the centrifugal force created by saw cylinders rotating at 300 to 400 rpm to “sling off” foreign material while the fibre is held by the saw. The foreign matter that is slung off the reclaimer feeds into the trash-handling system. Processing rates of 4.9 to 6.6 bales/hr/m of cylinder length are common.
Ginning (lint-seed separation)
After going through another stage of drying and cylinder cleaning, cotton is distributed to each gin stand by the conveyor-distributor. Located above the gin stand, the extractor-feeder meters seed cotton uniformly to the gin stand at controllable rates, and cleans seed cotton as a secondary function. The moisture content of cotton fibre at the extractor-feeder apron is critical. The moisture must be low enough that foreign matter can be easily removed in the gin stand. However, the moisture must not be so low (below 5%) as to result in the breakage of individual fibres as they are separated from the seed. This breakage causes an appreciable reduction both in fibre length and lint turnout. From a quality standpoint, cotton with a higher content of short fibres produces excessive waste at the textile mill and is less desirable. Excessive breakage of fibres can be avoided by maintaining a fibre moisture content of 6 to 7% at the extractor-feeder apron.
Two types of gins are in common use—the saw gin and the roller gin. In 1794, Eli Whitney invented a gin that removed fibre from the seed by means of spikes or saws on a cylinder. In 1796, Henry Ogden Holmes invented a gin having saws and ribs; this gin replaced Whitney’s gin and made ginning a continuous-flow process rather than a batch process. Cotton (usually Gossypium hirsutum) enters the saw gin stand through a huller front. The saws grasp the cotton and draw it through widely spaced ribs known as huller ribs. The locks of cotton are drawn from the huller ribs into the bottom of the roll box. The actual ginning process—separation of lint and seed—takes place in the roll box of the gin stand. The ginning action is caused by a set of saws rotating between ginning ribs. The saw teeth pass between the ribs at the ginning point. Here the leading edge of the teeth is approximately parallel to the rib, and the teeth pull the fibres from the seed, which are too large to pass between the ribs. Ginning at rates above those recommended by the manufacturer can cause fibre quality reduction, seed damage and choke-ups. Gin stand saw speeds are also important. High speeds tend to increase the fibre damage done during ginning.
Roller-type gins provided the first mechanically aided means of separating extra-long staple cotton (Gossypium barbadense) lint from seed. The Churka gin, which has an unknown origin, consisted of two hard rollers that ran together at the same surface speed, pinching the fibre from the seed and producing about 1 kg of lint/day. In 1840, Fones McCarthy invented a more efficient roller gin that consisted of a leather ginning roller, a stationary knife held tightly against the roller and a reciprocating knife that pulled the seed from the lint as the lint was held by the roller and stationary knife. In the late 1950s, a rotary-knife roller gin was developed by the US Department of Agriculture (USDA) Agricultural Research Service’s Southwestern Cotton Ginning Research Laboratory, US gin manufacturers and private ginneries. This gin is currently the only roller-type gin used in the United States.
Lint cleaning
Cotton is conveyed from the gin stand through lint ducts to condensers and formed again into a batt. The batt is removed from the condenser drum and fed into the saw-type lint cleaner. Inside the lint cleaner, cotton passes through the feed rollers and over the feed plate, which applies the fibres to the lint cleaner saw. The saw carries cotton under grid bars, which are aided by centrifugal force and remove immature seeds and foreign matter. It is important that the clearance between the saw tips and grid bars be properly set. The grid bars must be straight with a sharp leading edge to avoid reducing cleaning efficiency and increasing lint loss. Increasing the lint cleaner’s feed rate above the manufacturer’s recommended rate will decrease cleaning efficiency and increase loss of good fibre. Roller-ginned cotton is usually cleaned with non-aggressive, non-saw-type cleaners to minimize fibre damage.
Lint cleaners can improve the grade of cotton by removing foreign matter. In some cases, lint cleaners may improve the colour of a lightly spotted cotton by blending to produce a white grade. They may also improve the colour grade of a spotted cotton to light spotted or perhaps white colour grade.
Packaging
The cleaned cotton is compressed into bales, which must then be covered to protect them from contamination during transportation and storage. Three types of bales are produced: modified flat, compress universal density and gin universal density. These bales are packaged at densities of 224 and 449 kg/m3 for the modified flat and universal density bales, respectively. In most gins cotton is packaged in a “double-box” press wherein the lint is initially compacted in one press box by a mechanical or hydraulic tramper; then the press box is rotated, and the lint is further compressed to about 320 or 641 kg/m3 by modified flat or gin universal density presses, respectively. Modified flat bales are recompressed to become compress universal density bales in a later operation to achieve optimum freight rates. In 1995, about 98% of the bales in the United States were gin universal density bales.
Fibre quality
Cotton quality is affected by every production step, including selecting the variety, harvesting and ginning. Certain quality characteristics are highly influenced by genetics, while others are determined mainly by environmental conditions or by harvesting and ginning practices. Problems during any step of production or processing can cause irreversible damage to fibre quality and reduce profits for the producer as well as the textile manufacturer.
Fibre quality is highest the day a cotton boll opens. Weathering, mechanical harvesting, handling, ginning and manufacturing can diminish the natural quality. There are many factors that indicate the overall quality of cotton fibre. The most important ones include strength, fibre length, short fibre content (fibres shorter than 1.27 cm), length uniformity, maturity, fineness, trash content, colour, seedcoat fragment and nep content, and stickiness. The market generally recognizes these factors even though not all are measured on each bale.
The ginning process can significantly affect fibre length, uniformity and the content of seedcoat fragments, trash, short fibres and neps. The two ginning practices that have the most impact on quality are the regulation of fibre moisture during ginning and cleaning and the degree of saw-type lint cleaning used.
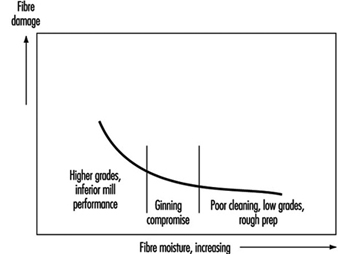
The recommended lint moisture range for ginning is 6 to 7%. Gin cleaners remove more trash at low moisture but not without more fibre damage. Higher fibre moisture preserves fibre length but results in ginning problems and poor cleaning, as illustrated in figure 1. If drying is increased to improve trash removal, yarn quality is reduced. Although yarn appearance improves with drying up to a point, because of increased foreign-matter removal, the effect of increased short-fibre content outweighs the benefits of foreign-matter removal.
Figure 1. Moisture-ginning cleaning compromise for cotton
Cleaning does little to change the true colour of the fibre, but combing the fibres and removing trash changes the perceived colour. Lint cleaning can sometimes blend fibre so that fewer bales are classified as spotted or light spotted. Ginning does not affect fineness and maturity. Each mechanical or pneumatic device used during cleaning and ginning increases the nep content, but lint cleaners have the most pronounced influence. The number of seedcoat fragments in ginned lint is affected by the seed condition and ginning action. Lint cleaners decrease the size but not the number of fragments. Yarn strength, yarn appearance and spinning-end breakage are three important spinning quality elements. All are affected by length uniformity and, therefore, by the proportion of short or broken fibres. These three elements are usually preserved best when cotton is ginned with minimum drying and cleaning machinery.
Recommendations for the sequence and amount of gin machinery to dry and clean spindle-harvested cotton were designed to achieve satisfactory bale value and to preserve the inherent quality of cotton. They have generally been followed and thus confirmed in the US cotton industry for several decades. The recommendations consider marketing-system premiums and discounts as well as the cleaning efficiency and fibre damage resulting from various gin machines. Some variation from these recommendations is necessary for special harvesting conditions.
When gin machinery is used in the recommended sequence, 75 to 85% of the foreign matter is usually removed from cotton. Unfortunately, this machinery also removes small quantities of good-quality cotton in the process of removing foreign matter, so the quantity of marketable cotton is reduced during cleaning. Cleaning cotton is therefore a compromise between foreign matter level and fibre loss and damage.
Safety and Health Concerns
The cotton ginning industry, like other processing industries, has many hazards. Information from workers’ compensation claims indicates that the number of injuries is highest for the hand/fingers, followed by back/spine, eye, foot/toes, arm/shoulder, leg, trunk and head injuries. While the industry has been active in hazard reduction and safety education, gin safety remains a major concern. The reasons for the concern include the high frequency of accidents and workers’ compensation claims, the large number of lost work days and the severity of the accidents. Total economic costs for gin injuries and health disorders include direct costs (medical and other compensation) and indirect costs (time lost from work, downtime, loss in earning power, higher insurance costs for workers’ compensation, loss of productivity and many other loss factors). Direct costs are easier to determine and much less expensive than indirect costs.
Many international safety and health regulations affecting cotton ginning are derived from US legislation administered by the Occupational Safety and Health Administration (OSHA) and the Environmental Protection Agency (EPA), which promulgates pesticides regulations.
Other agricultural regulations may also apply to a gin, including requirements for slow-moving vehicle emblems on trailers/tractors operating on public roadways, provisions for rollover protective structures on tractors operated by employees and provisions for proper living facilities for temporary labour. While gins are considered agricultural enterprises and are not specifically covered by many regulations, ginners will likely want to conform to other regulations, such as OSHA’s “Standards for General Industry, Part 1910”. There are three specific OSHA standards that ginners should consider: those for fire and other emergency plans (29 CFR 1910.38a), exits (29 CFR 1910.35-40) and occupational noise exposure (29 CFR 1910.95). Major exit requirements are given in 29 CFR 1910.36 and 29 CFR 1910.37. In other countries, where agricultural workers are included in mandatory coverage, such compliance will be compulsory. Compliance with noise and other safety and health standards is discussed elsewhere in this Encyclopaedia.
Employee participation in safety programmes
The most effective loss control programmes are those in which management motivates employees to be safety conscious. This motivation can be accomplished by establishing a safety policy that gets the employees involved in each element of the programme, by participating in safety training, by setting a good example and by providing employees with appropriate incentives.
Occupational health disorders are lessened by requiring that PPE be used in designated areas and that employees observe acceptable work practices. Hearing (plugs or muffs) and respiratory (dust mask) PPE should be used whenever working in areas having high noise or dust levels. Some people are more susceptible to noise and respiratory problems than others, and even with PPE should be reassigned to work areas with lower noise or dust levels. Health hazards associated with heavy lifting and excessive heat can be handled by training, use of materials-handling equipment, proper dress, ventilation and breaks from the heat.
All persons throughout the gin operation must be involved in gin safety. A safe work atmosphere can be established when everyone is motivated to participate fully in the loss control programme.
Global Trends in the Textile Industry
Human beings have relied on clothing and food to survive ever since they appeared on earth. The clothing or textile industry thus began very early in human history. While early people used their hands to weave and knit cotton or wool into fabric or cloth, it was not until the late 18th and early 19th centuries that the Industrial Revolution changed the way of making clothes. People started to use various kinds of energy to supply power. Nevertheless, cotton, wool and cellulose fibres remained the major raw materials. Since the Second World War, the production of synthetic fibres developed by the petrochemical industry has increased tremendously. The consumption volume of synthetic fibres of world textile products in 1994 was 17.7 million tons, 48.2% of all fibres, and it is expected to exceed 50% after 2000 (see figure 1).
Figure 1. Change in fibre supply in the textile industry before 1994 and projected through 2004.
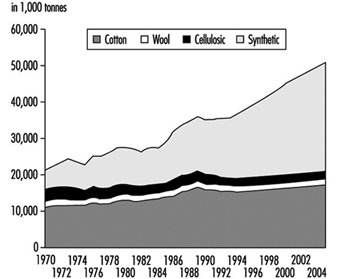
According to the world apparel fibre consumption survey by the Food and Agricultural Organization (FAO), the average annual rates of growth for textile consumption during 1969–89, 1979–89 and 1984–89 were 2.9%, 2.3% and 3.7% respectively. Based on the previous consumption trend, population growth, per capita GDP (gross domestic product) growth, and the increase of consumption of each textile product with rising income, the demand for textile products in 2000 and 2005 will be 42.2 million tons and 46.9 million tons, respectively, as shown in figure 1. The trend indicates that there is a consistent growing demand for textile products, and that the industry will still employ a large workforce.
Another major change is the progressive automation of weaving and knitting, which, combined with rising labour costs, has shifted the industry from the developed to the developing countries. Although the production of yarn and fabric products, as well as some upstream synthetic fibres, has remained in more developed countries, a large proportion of the labour-intensive downstream apparel industry has already moved to the developing countries. The Asia-Pacific region’s textile and clothing industry now accounts for approximately 70% of the world production; table 1 indicates a shifting trend of employment in this region. Thus, the occupational safety and health of textile workers has become a major issue in developing countries; figure 2, figure 3, figure 4 and figure 5, illustrate some textile industry processes as they are carried out in the developing world.
Table 1. Numbers of enterprises and employees in textile and apparel industries of selected countries and territories in the Asia-Pacific area in 1985 and 1995.
|
Number of |
Year |
Australia |
China |
Hong Kong |
India |
Indonesia |
Korea, Republic of |
Malaysia |
New Zealand |
Pakistan |
|
Enterprises |
1985 |
2,535 |
45,500 |
13,114 |
13,435 |
1,929 |
12,310 |
376 |
2,803 |
1,357 |
|
Employees (x10³) |
1985 |
96 |
4,396 |
375 |
1,753 |
432 |
684 |
58 |
31 |
N.A. |
Wilawan Juengprasert, Ministry of Public Health, Thailand
Wilawan Juengprasert, Ministry of Public Health, Thailand
Wilawan Juengprasert, Ministry of Public Health, Thailand

Wilawan Juengprasert, Ministry of Public Health, Thailand
The Textile Industry: History and Health and Safety
The Textile Industry
The term textile industry (from the Latin texere, to weave) was originally applied to the weaving of fabrics from fibres, but now it includes a broad range of other processes such as knitting, tufting, felting and so on. It has also been extended to include the making of yarn from natural or synthetic fibres as well as the finishing and dyeing of fabrics.
Yarn making
In prehistoric eras, animal hair, plants and seeds were used to make fibres. Silk was introduced in China around 2600 BC, and in the middle of the 18th century AD, the first synthetic fibres were created. While synthetic fibres made from cellulose or petrochemicals, either alone or in varied combinations with other synthetic and/or natural fibres, have seen increasingly widening use, they have not been able to totally eclipse fabrics made of natural fibres such as wool, cotton, flax and silk.
Silk is the only natural fibre formed in filaments which can be twisted together to make yarn. The other natural fibres must first be straightened, made parallel by combing and then drawn into a continuous yarn by spinning. The spindle is the earliest spinning tool; it was first mechanized in Europe around 1400 AD by the invention of the spinning wheel. The late 17th century saw the invention of the spinning jenny, which could operate a number of spindles simultaneously. Then, thanks to Richard Arkwright’s invention of the spinning frame in 1769 and Samuel Crompton’s introduction of the mule, which allowed one worker to operate 1,000 spindles at one time, yarn-making moved from being a cottage industry into the mills.
Making of fabric
The making of fabric had a similar history. Ever since its origins in antiquity, the hand loom has been the basic weaving machine. Mechanical improvements began in ancient times with the development of the heddle, to which alternate warp threads are tied; in the 13th century AD, the foot treadle, which could operate several sets of heddles, was introduced. With the addition of the frame-mounted batten, which beats the weft or filling yarns into place, the “mechanized” loom became the predominant weaving instrument in Europe and, except for traditional cultures where the original hand looms persisted, around the world.
John Kay’s invention of the flying shuttle in 1733, which allowed the weaver to send the shuttle across the width of the loom automatically, was the first step in mechanization of weaving. Edmund Cartwright developed the steam-powered loom and in 1788, with James Watt, built the first steam-driven textile mill in England. This freed the mills from their dependence on water-driven machinery and allowed them to be constructed anywhere. Another significant development was the punch-card system, developed in France in 1801 by Joseph Marie Jacquard; this allowed automated weaving of patterns. The earlier power looms made of wood were gradually replaced by looms made of steel and other metals. Since then, technological changes have focused on making them larger, faster and more highly automated.
Dyeing and printing
Natural dyes were originally used to impart colour to yarns and fabrics, but with the 19th-century discovery of coal-tar dyes and the 20th-century development of synthetic fibres, dyeing processes have become more complicated. Block printing was originally used to colour fabrics (silk-screen printing of fabrics was developed in the mid-1800s), but it soon was replaced by roller printing. Engraved copper rollers were first used in England in 1785, followed by rapid improvements that allowed roller printing in six colours all in perfect register. Modern roller printing can produce over 180 m of fabric printed in 16 or more colours in 1 minute.
Finishing
Early on, fabrics were finished by brushing or shearing the nap of the fabric, filling or sizing the cloth, or passing it through calender rolls to produce a glazed effect. Today, fabrics are pre-shrunk, mercerized (cotton yarns and fabrics are treated with caustic solutions to improve their strength and lustre) and treated by a variety of finishing processes that, for example, increase crease resistance, crease holding and resistance to water, flame and mildew.
Special treatments produce high-performance fibres, so called because of their extraordinary strength and extremely high temperature resistance. Thus, Aramid, a fibre similar to nylon, is stronger than steel, and Kevlar, a fibre made from Aramid, is used to make bullet-proof fabrics and clothing that is resistant both to heat and chemicals. Other synthetic fibres combined with carbon, boron, silicon, aluminium and other materials are used to produce the lightweight, superstrong structural materials used in airplanes, spacecraft, chemical resistant filters and membranes, and protective sports gear.
From hand craft to industry
Textile manufacture was originally a hand craft practised by cottage spinners and weavers and small groups of skilled artisans. With the technological developments, large and economically important textile enterprises emerged, primarily in the United Kingdom and the Western European countries. Early settlers in North America brought cloth mills to New England (Samuel Slater, who had been a mill supervisor in England, constructed from memory a spinning frame in Providence, Rhode Island, in 1790), and the invention of Eli Whitney’s cotton gin, which could clean harvested cotton with great speed, created a new demand for cotton fabrics.
This was accelerated by the commercialization of the sewing machine. In the early 18th century, a number of inventors produced machines that would stitch cloth. In France in 1830, Barthelemy Thimonnier received a patent for his sewing machine; in 1841, when 80 of his machines were busy sewing uniforms for the French army, his factory was destroyed by tailors who saw his machines as a threat to their livelihood. At about that time in England, Walter Hunt devised an improved machine but abandoned the project because he felt that it would throw poor seamstresses out of work. In 1848, Elias Howe received a US patent for a machine much like Hunt’s, but became embroiled in legal battles, which he ultimately won, charging many manufacturers with infringement of his patent. The invention of the modern sewing machine is credited to Isaac Merritt Singer, who devised the overhanging arm, the presser foot to hold down the cloth, a wheel to feed the fabric to the needle and a foot treadle instead of a hand crank, leaving both hands free to manoeuvre the fabric. In addition to designing and manufacturing the machine, he created the first large-scale consumer-appliance enterprise, which featured such innovations as an advertising campaign, selling the machines on the installment plan, and providing a service contract.
Thus, the technological advances during the 18th century were not only the impetus for the modern textile industry but they can be credited with the creation of the factory system and the profound changes in family and community life that have been labelled the Industrial Revolution. The changes continue today as large textile establishments move from the old industrialized areas to new regions that promise cheaper labour and sources of energy, while competition fosters continuing technological developments such as computer-controlled automation to reduce labour needs and improve quality. Meanwhile, politicians debate quotas, tariffs and other economic barriers to provide and/or retain competitive advantages for their countries. Thus, the textile industry not only provides products essential for the world’s growing population; it also has a profound influence on international trade and the economies of nations.
Safety and Health Concerns
As machines became larger, speedier and more complicated, they also introduced new potential hazards. As materials and processes became more complex, they infused the workplace with potential health hazards. And as workers had to cope with mechanization and the demand for increasing productivity, work stress, largely unrecognized or ignored, exerted an increasing influence on their well-being. Perhaps the greatest effect of the Industrial Revolution was on community life, as workers moved from the country to cities, where they had to contend with all of the ills of urbanization. These effects are being seen today as the textile and other industries move to developing countries and regions, except that the changes are more rapid.
The hazards encountered in different segments of the industry are summarized in the other articles in this chapter. They emphasize the importance of good housekeeping and proper maintenance of machines and equipment, the installation of effective guards and fences to prevent contact with moving parts, the use of local exhaust ventilation (LEV) as a supplement to good general ventilation and temperature control, and the provision of appropriate personal protective equipment (PPE) and clothing whenever a hazard cannot be completely controlled or prevented by design engineering and/or substitution of less hazardous materials. Repeated education and training of workers on all levels and effective supervision are recurrent themes.
Environmental Concerns
Environmental concerns raised by the textile industry stem from two sources: the processes involved in textile manufacture and hazards associated with the way the products are used.
Textile manufacture
The chief environmental problems created by textile manufacturing plants are toxic substances released into the atmosphere and into wastewater. In addition to potentially toxic agents, unpleasant odours are often a problem, especially where dyeing and printing plants are located near residential areas. Ventilation exhausts may contain vapours of solvents, formaldehyde, hydrocarbons, hydrogen sulphide and metallic compounds. Solvents may sometimes be captured and distilled for reuse. Particulates may be removed by filtration. Scrubbing is effective for water-soluble volatile compounds such as methanol, but it does not work in pigment printing, where hydrocarbons make up most of the emissions. Flammables may be burned off, although this is relatively expensive. The ultimate solution, however, is the use of materials that are as close to being emission-free as possible. This refers not only to the dyes, binders and cross-linking agents used in the printing, but also to the formaldehyde and residual monomer content of fabrics.
Contamination of wastewater by unfixed dyes is a serious environmental problem not only because of the potential health hazards to human and animal life, but also because of the discolouration that makes it highly visible. In ordinary dyeing, fixation of over 90% of the dyestuff can be achieved, but fixation levels of only 60% or less are common in printing with reactive dyes. This means that more than one-third of the reactive dye enters the wastewater during the washing-off of the printed fabric. Additional amounts of dyes are introduced into the wastewater during the washing of screens, printing blankets and drums.
Limits on wastewater discolouration have been set in a number of countries, but it is often very difficult to heed them without an expensive wastewater purification system. A solution is found in the use of dyestuffs with a lesser contaminating effect and the development of dyes and synthetic thickening agents that increase the degree of dye fixation, thereby reducing the amounts of the excess to be washed away (Grund 1995).
Environmental concerns in textile use
Residues of formaldehyde and some heavy-metal complexes (most of these are inert) may be sufficient to cause skin irritation and sensitization in persons wearing the dyed fabrics.
Formaldehyde and residual solvents in carpets and fabrics used for upholstery and curtains will continue to vaporize gradually for some time. In buildings that are sealed, where the air-conditioning system recirculates most of the air rather than exhausting it to the outside environment, these substances may reach levels high enough to produce symptoms in the occupants of the building, as discussed elsewhere in this Encyclopaedia.
To ensure the safety of fabrics, Marks and Spencer, the British/Canadian clothing retailer, led the way by setting limits for formaldehyde in garments they would purchase. Since then, other garment manufacturers, notably Levi Strauss in the United States, have followed suit. In a number of countries, these limits have been formalized in laws (e.g., Denmark, Finland, Germany and Japan), and, in response to consumer education, fabric manufacturers have been voluntarily adhering to such limits in order to be able to use eco labels (see figure 1).
Figure 1. Ecological labels used for textiles

Conclusion
Technological developments are continuing to enhance the range of fabrics produced by the textile industry and to increase its productivity. It is most important, however, that these developments be guided also by the imperative of enhancing the health, safety and well-being of the workers. But even then, there is the problem of implementing these developments in older enterprises that are marginally financially viable and unable to make the necessary investments, as well as in developing areas eager to have new industries even at the expense of the health and safety of the workers. Even under these circumstances, however, much can be achieved by education and training of the workers to minimize the risks to which they may be exposed.
Environmental Protection and Public Health Issues
The treatment and processing of animal skins and hides can be a source of considerable environmental impact. Discharged wastewater contains pollutants from the hides, products from their decomposition and chemicals and various spent solutions used for hide preparation and during the tanning process. Solid wastes and some atmospheric emissions also may arise.
The major public concern over tanneries has traditionally been about odours and water pollution from untreated discharges. Other issues have arisen more recently from the increasing use of synthetic chemicals such as pesticides, solvents, dyes, finishing agents and new processing chemicals which introduce problems of toxicity and persistence.
Simple measures intended to control pollution can themselves create secondary cross-media environmental impacts such as groundwater pollution, soil contamination, sludge dumping and chemical poisoning.
Tanning technology that is now available, based on a lower chemical and water consumption, has less impact on the environment than traditional processes. However, many obstacles remain to its widespread application.
Figure 1 presents the different wastes and environmental impacts associated with the various processes used in the tanning industry.
Figure 1. Environmental impacts & tannery operations
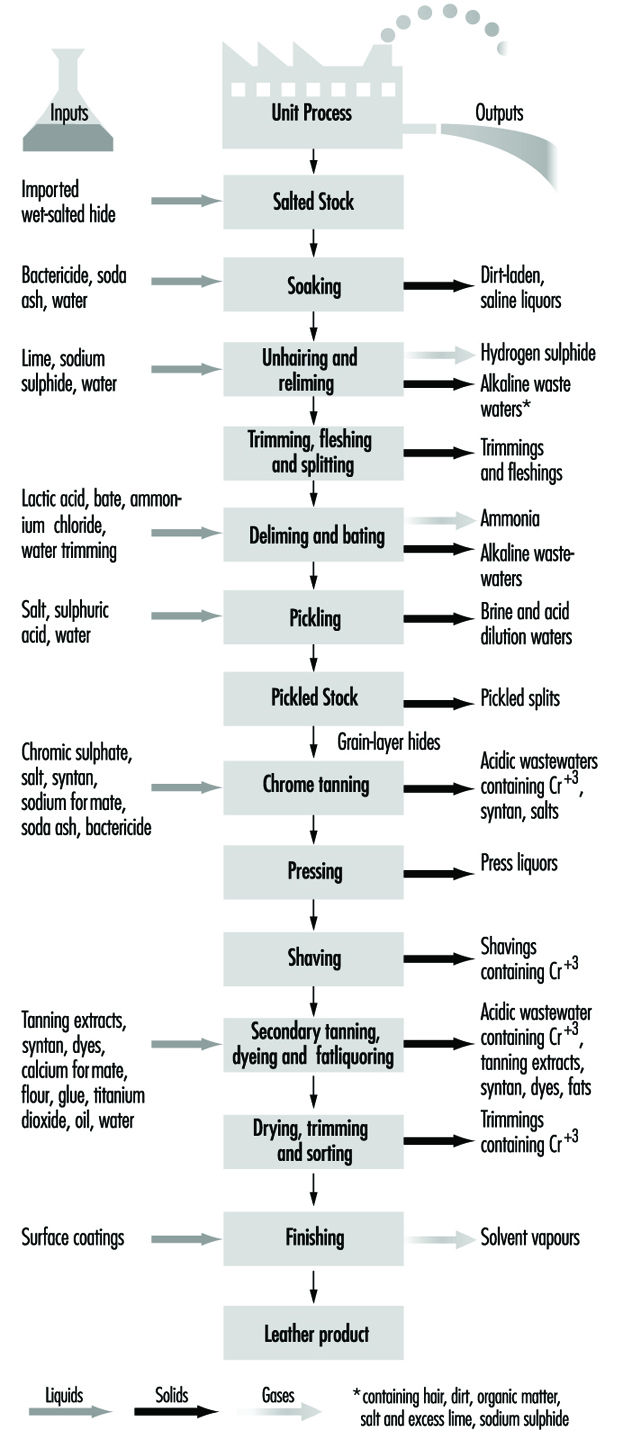
Pollution Control
Water pollution control
Untreated tannery wastes in surface waters can bring about a rapid deterioration of their physical, chemical and biological properties. Simple end-of-pipe effluent treatment processes can remove over 50% of suspended solids and biochemical oxygen demand (BOD) of effluent. More sophisticated measures are capable of higher levels of treatment.
As tannery effluents contain several chemical constituents that need to be treated, a sequence of treatment processes in turn must be used. Flow segregation is useful to allow separate treatment of concentrated waste streams.
Table 1 summarizes technological choices available for treatment of tannery effluents.
Table 1. Technological choices for treatment of tannery effluents
|
Pre-treatment settling |
Mechanical screening to remove coarse material Flow equalization (balancing) |
|
Primary treatment |
Sulphide removal from beamhouse effluents Chromium removal from tanning effluents Physical-chemical treatment for BOD removal and neutralization |
|
Secondary treatment |
Biological treatment Activated sludge (oxidation ditch) Activated sludge (conventional) Lagooning (aerated, facultative or anaerobic) |
|
Tertiary treatment |
Nitrification and denitrification |
|
Sedimentation and sludge handling |
Different shapes and dimensions of tanks and basins |
Air pollution control
Air emissions fall into three broad groups: odours, solvent vapours from finishing operations and gas emissions from the incineration of wastes.
Biological decomposition of organic matter as well as sulphide and ammonia emissions from wastewaters are responsible for the characteristic objectionable odours arising from tanneries. The siting of installations has been an issue because of the odours that have historically been associated with tanneries. Reduction of these odours is more a question of operational maintenance than of technology.
Solvent and other vapours from the finishing operations vary with the type of chemicals used and the technical methods employed to reduce their generation and release. Up to 30% of the solvent used may be wasted through emissions, while modern processes are available to reduce this to around 3% in many cases.
The practice by many tanneries of incinerating solid wastes and offcuts raises the importance of adopting good incinerator design and following careful operating practices.
Waste management
Treatment of sludge constitutes the largest disposal problem, apart from effluent. Sludges of organic composition, if free from chrome or sulphides, have value as a soil conditioner as well as a small fertilizer effect from nitrogenous compounds contained therein. These benefits are best realized by ploughing immediately after application. Agricultural use of chrome-containing soils has been a matter of controversy in various jurisdictions, where guidelines have determined acceptable applications.
Various markets exist for the conversion of trimmings and fleshings into by-products used for a variety of purposes, including the production of gelatin, glue, leatherboard, tallow grease and proteins for animal feed. Process effluents, subject to suitable treatment and quality control, are sometimes used for irrigation where water is in short supply and/or effluent disposal is severely restricted.
To avoid problems of leachate generation and odour, only solids and dewatered sludges should be disposed of at landfill sites. Care must be taken to ensure that tannery wastes do not react with other industrial residues, such as acidic wastes, which can react to create toxic hydrogen sulphide gas. Incineration under uncontrolled conditions may lead to unacceptable emissions and is not recommended.
Pollution Prevention
Improving production technologies to increase environmental performance can achieve a number of objectives, such as:
- increasing the efficiency of chemical utilization
- reducing water or energy consumption
- recovering or recycling rejected materials.
Water consumption can vary considerably, ranging from less than 25 l/kg of raw hide to greater than 80 l/kg. Water use efficiency can be improved through the application of techniques such as increased volume control of processing waters, “batch” versus “running water” washes, low float modification of existing equipment; low float techniques using updated equipment, re-use of wastewater in less critical processes and recycling of individual process liquors.
Traditional soaking and unhairing account for over 50% of the BOD and chemical oxygen demand (COD) loads in typical tanning effluents. Various methods can be employed to substitute for sulphide, to recycle lime/sulphide liquors and to incorporate hair-saving techniques.
Reduction in chromium pollution can be achieved through measures to increase the levels of chrome that are fixed in the tanning bath and reduce the amounts that are “bled out” in subsequent processes. Other methods to reduce release of chromium are through direct recycling of used chrome liquors (which also reduces salinity of waste effluent) and the treatment of collected chrome-bearing liquors with alkali to precipitate the chromium as hydroxide, which can then be recycled. An illustration of a communal chrome recovery operation is shown in figure 2.
Figure 2. Flow chart for a communal plant for chrome recovery
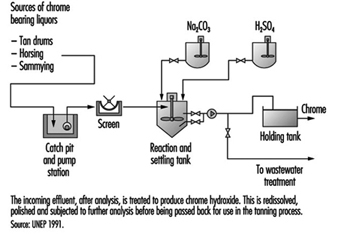
Where vegetable tanning is employed, preconditioning of hides can enhance the penetration and fixation of hides and contribute to decreased tannin concentrations in effluents. Other tanning agents such as titanium have been used as substitutes for chromium to produce salts of generally lower toxicity and to generate sludges that are inert and safer to handle.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."