Type and Frequency of Disasters
In 1990, the 44th General Assembly of the United Nations launched the decade for the reduction of frequency and impact of natural disasters (Lancet 1990). A committee of experts endorsed a definition of disasters as “a disruption of the human ecology that exceeds the capacity of the community to function normally”.
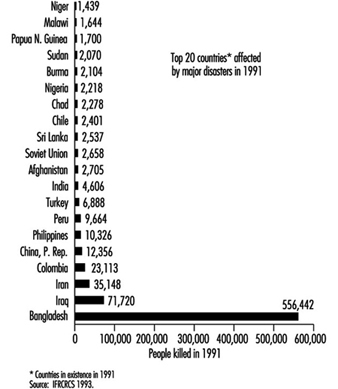
Over the past few decades, disaster data on a global level reveal a distinct pattern with two main features—an increase over time of the number of people affected, and a geographical correlation (International Federation of Red Cross and Red Crescent Societies (IFRCRCS) 1993). In figure 1, despite the great variation from year to year, a definite rising trend is quite visible. Figure 2 shows the countries most severely affected by major disasters in 1991. Disasters affect every country of the world, but it is the poorest countries where people most frequently lose their lives.
Figure 1. Number of persons affected worldwide by disasters per year during 1967-91
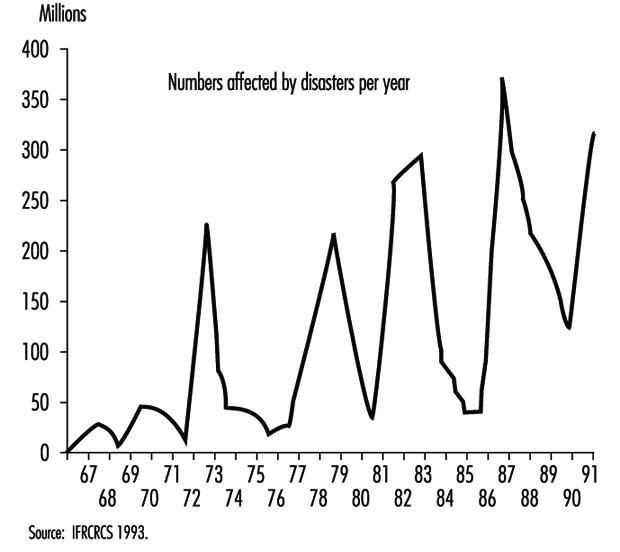
Figure 2. Number of people dead from major disasters in 1991: Top 20 countries
Numerous and different definitions and classifications of disasters are available and have been reviewed (Grisham 1986; Lechat 1990; Logue, Melick and Hansen 1981; Weiss and Clarkson 1986). Three of them are mentioned here as examples: The US Centers for Disease Control (CDC 1989) identified three major categories of disasters: geographical events such as earthquakes and volcanic eruptions; weather-related problems, including hurricanes, tornadoes, heat waves, cold environments and floods; and, finally, human-generated problems, which encompass famines, air pollutions, industrial disasters, fires and nuclear reactor incidents. Another classification by cause (Parrish, Falk and Melius 1987) included weather and geological events among natural disasters, whereas human-made causes were defined as non-natural, technological, purposeful events perpetuated by people (e.g., transportation, war, fire/explosion, chemical and radioactive release). A third classification (table1), compiled at the Centre for Research on the Epidemiology of Disaster in Louvain, Belgium, was based on a workshop convened by the UN Disaster Relief Organization in 1991 and was published in the World Disaster Report 1993 (IFRCRCS 1993).
Table 1. Definitions of disaster types
|
Sudden natural |
Long-term natural |
Sudden human-made |
Long-term human-made |
|
Avalanche Cold wave Earthquake Aftershock Floods Flash flood Dam collapse Volcanic eruption Glowing Heat wave High wind Storm Hail Sand storm Storm surges Thunder storm Tropical storm Tornado Insect infestation Landslide Earth flow Power shortage Tsunami and tidal |
Epidemics Drought Desertification Famine Food shortage or |
Structural collapse Building collapse Mine collapse or cave-in Air disaster Land disaster Sea disaster Industrial/technological Explosions Chemical explosions Nuclear explosion Mine explosions Pollution Acid rain Chemical pollution Atmosphere pollution Chlorofluoro-carbons Oil pollution Fires Forest/grassland fire |
National (civil strife, International Displaced population Displaced persons Refugees |
Source: IFRCRCS 1993.
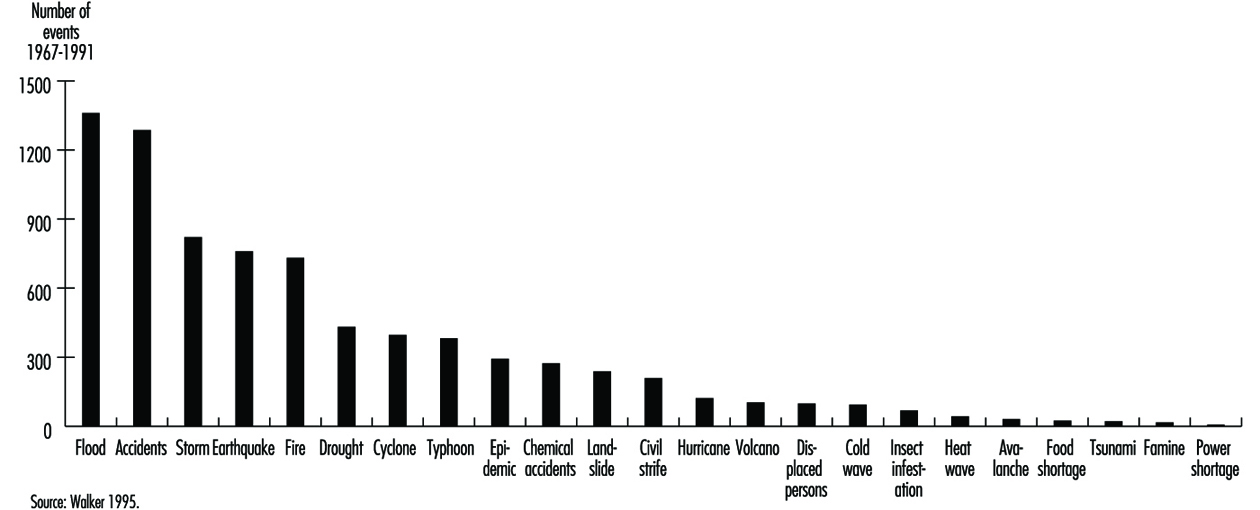
Figure 3 reports the number of events for individual disaster types. The item “Accidents” includes all sudden human-made events, and is second only to “Flood” in frequency. “Storm” is in third place, followed by “Earthquake” and “Fire”.
Figure 3. 1967-91: Total number of events for each type of disaster
Additional information on type, frequency and consequences of natural and non-natural disasters between 1969 and 1993 has been drawn from data of the IFRCRCS 1993.
Although agencies measure the severity of disasters by the number of people killed, it is becoming increasingly important also to look at the number affected. Across the world, almost a thousand times more people are affected by disaster than are killed and, for many of these people, survival after the disaster is becoming increasingly difficult, leaving them more vulnerable to future shocks. This point is relevant not only for natural disasters (table 2) but also human-made disasters (table 3), especially in the case of chemical accidents whose effects on exposed people may become apparent after years or even decades (Bertazzi 1989). Addressing human vulnerability to disaster is at the heart of disaster preparedness and prevention strategies.
Table 2. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
76,883 |
9,027 |
56,072 |
2,220 |
99 |
144,302 |
|
Injured |
1,013 |
14,944 |
27,023 |
3,521 |
100 |
46,601 |
|
Otherwise affected |
10,556,984 |
4,400,232 |
105,044,476 |
563,542 |
95,128 |
120,660,363 |
|
Homeless |
172,812 |
360,964 |
3,980,608 |
67,278 |
31,562 |
4,613,224 |
Source: Walker 1995.
Table 3. Number of victims of disasters with a non-natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
16,172 |
3,765 |
2,204 |
739 |
18 |
22,898 |
|
Injured |
236 |
1,030 |
5,601 |
483 |
476 |
7,826 |
|
Affected |
3,694 |
48,825 |
41,630 |
7,870 |
610 |
102,629 |
|
Homeless |
2,384 |
1,722 |
6,275 |
7,664 |
24 |
18,069 |
Source: Walker 1995.
Drought, famine and floods continue to affect far more people than any other type of disaster. High winds (cyclones, hurricanes and typhoons) cause proportionally more deaths than famines and floods, in relation to the affected population as a whole; and earthquakes, the most sudden-onset disaster of all, continue to have the greatest ratio of deaths to affected population (table 4). Technological accidents affected more people than fires (table 5).
Table 4. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by type
|
Earthquake |
Drought |
Flood |
High wind |
Landslide |
Volcano |
Total |
|
|
Killed |
21,668 |
73,606 |
12,097 |
28,555 |
1,550 |
1,009 |
138,486 |
|
Injured |
30,452 |
0 |
7,704 |
7,891 |
245 |
279 |
46,571 |
|
Affected |
1,764,724 |
57,905,676 |
47,849,065 |
9,417,442 |
131,807 |
94,665 |
117,163,379 |
|
Homeless |
224,186 |
22,720 |
3,178,267 |
1,065,928 |
106,889 |
12,513 |
4,610,504 |
Source: Walker 1995.
Table 5. Disasters and Major Accidents
|
Accident |
Technological accident |
Fire |
Total |
|
|
Killed |
3,419 |
603 |
3,300 |
7,321 |
|
Injured |
1,596 |
5,564 |
699 |
7,859 |
|
Affected |
17,153 |
52,704 |
32,771 |
102,629 |
|
Homeless |
868 |
8,372 |
8,829 |
18,069 |
Source: Walker 1995.
Table 6 and table 7 show the number of grouped disaster types over 25 years, by continent. High winds, accidents (mostly transport accidents) and floods account for the largest number of disaster events, with the largest proportion of events being in Asia. Africa accounts for the vast majority of the world’s drought events. While few people are killed by disasters in Europe, the region suffers from disaster events on a scale comparable to that in Asia or Africa, the lower mortality figures reflecting a much lower human vulnerability to crisis. A clear example is the comparison of the human death tolls after the chemical accidents in Seveso (Italy) and in Bhopal (India) (Bertazzi 1989).
Table 6. Disasters with a natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
40 |
125 |
225 |
167 |
83 |
640 |
|
Drought and famine |
277 |
49 |
83 |
15 |
14 |
438 |
|
Flood |
149 |
357 |
599 |
123 |
138 |
1,366 |
|
Landslide |
11 |
85 |
93 |
19 |
10 |
218 |
|
High wind |
75 |
426 |
637 |
210 |
203 |
1,551 |
|
Volcano |
8 |
27 |
43 |
16 |
4 |
98 |
|
Other* |
219 |
93 |
186 |
91 |
4 |
593 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 7. Disasters with a non-natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
213 |
321 |
676 |
274 |
18 |
1,502 |
|
Technological accident |
24 |
97 |
97 |
88 |
4 |
310 |
|
Fire |
37 |
115 |
236 |
166 |
29 |
583 |
Source: Walker 1995.
Figures for 1994 (table 8 and table 9) show that Asia continues to be the most disaster-prone region, with major accidents, floods and high wind disasters being the most common event types. Earthquakes, while causing high death rates per event, are in fact no more common than major technological disasters. The one-year average number of non-natural events, apart from fire, is slightly diminished in comparison with the preceding 25-year period. The average numbers of natural disasters, instead, were higher, with the exception of floods and volcanoes. In 1994, Europe had more human-made disasters than Asia (39 versus 37).
Table 8. Disasters with a natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
3 |
3 |
12 |
1 |
1 |
20 |
|
Drought and famine |
0 |
2 |
1 |
0 |
1 |
4 |
|
Flood |
15 |
13 |
27 |
13 |
0 |
68 |
|
Landslide |
0 |
1 |
3 |
1 |
0 |
5 |
|
High wind |
6 |
14 |
24 |
5 |
2 |
51 |
|
Volcano |
0 |
2 |
5 |
0 |
1 |
8 |
|
Other* |
2 |
3 |
1 |
2 |
0 |
8 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 9. Disasters with a non-natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
8 |
12 |
25 |
23 |
2 |
70 |
|
Technological accident |
1 |
5 |
7 |
7 |
0 |
20 |
|
Fire |
0 |
5 |
5 |
9 |
2 |
21 |
Source: Walker 1995.
Major Chemical Accidents
In this century, the worst non-natural disasters resulting in human suffering and death have been caused by wars, transport and industrial activities. At first, industrial disasters mainly affected people engaged in specific occupations, but later, particularly after the Second World War with the rapid growth and expansion of the chemical industry and the use of nuclear power, these occurrences led to serious danger even to people outside work areas, and to the general environment. We focus here on major accidents involving chemicals.
The first documented chemical disaster with industrial origins goes back to the 1600s. It was described by Bernardino Ramazzini (Bertazzi 1989). Today’s chemical disasters differ in the way they happen and in the type of chemicals involved (ILO 1988). Their potential hazard is a function both of the inherent nature of the chemical and the quantity that is present on site. A common feature is that they usually are uncontrolled events involving fires, explosions or releases of toxic substances that result either in the death and injury of a large number of people inside or outside the plant, extensive property and environmental damage, or both.
Table 10 gives some examples of typical major chemical accidents due to explosions. Table 11 lists some major fire disasters. Fires occur in industry more frequently than explosions and toxic releases, although the consequences in terms of loss of life are generally less. Better prevention and preparedness might be the explanation. Table 12 lists some major industrial accidents involving toxic releases of different chemicals. Chlorine and ammonia are the toxic chemicals most commonly used in major hazard quantities, and both have a history of major accidents. The release of flammable or toxic materials in the atmosphere may also lead to fires.
Table 10. Examples of industrial explosions
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Dimethyl ether |
245 |
3,800 |
Ludwigshafen, Federal Republic of Germany, 1948 |
|
Kerosene |
32 |
16 |
Bitburg, Federal Republic of Germany, 1948 |
|
Isobutane |
7 |
13 |
Lake Charles, Louisiana, United States, 1967 |
|
Oil slops |
2 |
85 |
Pernis, Netherlands, 1968 |
|
Propylene |
– |
230 |
East Saint Louis, Illinois, United States, 1972 |
|
Propane |
7 |
152 |
Decatur, Illinois, United States, 1974 |
|
Cyclohexane |
28 |
89 |
Flixborough, United Kingdom, 1974 |
|
Propylene |
14 |
107 |
Beek, Netherlands, 1975 |
Adapted from ILO 1988.
Table 11. Examples of major fires
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Methane |
136 |
77 |
Cleveland, Ohio, United States, 1944 |
|
Liquefied petroleum gas |
18 |
90 |
Ferzyn, France, 1966 |
|
Liquefied natural gas |
40 |
– |
Staten Island, New York, United States, 1973 |
|
Methane |
52 |
– |
Santa Cruz, Mexico, 1978 |
|
Liquefied petroleum gas |
650 |
2,500 |
Mexico City, Mexico, 1985 |
Adapted from ILO 1988.
Table 12. Examples of major toxic releases
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Phosgene |
10 |
– |
Poza Rica, Mexico, 1950 |
|
Chlorine |
7 |
– |
Wilsum, Federal Republic of Germany, 1952 |
|
Dioxin/TCDD |
– |
193 |
Seveso, Italy, 1976 |
|
Ammonia |
30 |
25 |
Cartagena, Colombia, 1977 |
|
Sulphur dioxide |
– |
100 |
Baltimore, Maryland, United States, 1978 |
|
Hydrogen sulphide |
8 |
29 |
Chicago, Illinois, United States, 1978 |
|
Methyl isocyanate |
2,500 |
200,000 |
Bhopal, India, 1984 |
Adapted from ILO 1988.
A review of the literature concerning major chemical disasters enables us to identify several other common characteristics of today’s industrial disasters. We will review them briefly, to provide not only a classification of general value, but also an appreciation of the nature of the problem and the challenges that face us.
Overt Disasters
Overt disasters are environmental releases which leave no ambiguity about their sources and their potential harm. Examples are Seveso, Bhopal and Chernobyl.
Seveso plays the role of prototype for chemical industrial disasters (Homberger et al. 1979; Pocchiari et al. 1983, 1986). The accident took place on 10 July 1976 in the Seveso area, close to Milan, Italy, in a plant where trichlorophenol was produced, and it caused the contamination of several square kilometres of populated countryside by the powerfully toxic 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD). More than 700 people were evacuated, and restrictions were applied to another 30,000 inhabitants. The most clearly established health effect was chloracne, but the picture of health consequences possibly linked to this incident has not yet been completed (Bruzzi 1983; Pesatori 1995).
Bhopal represents, probably, the worst chemical industrial disaster ever (Das 1985a, 1985b; Friedrich Naumann Foundation 1987; Tachakra 1987). On the night of 2 December 1984, a gas leak caused a deadly cloud to spread over the city of Bhopal, in central India, leaving thousands dead and hundreds of thousands injured in the space of a few hours. The accident occurred because of a runaway reaction in one of the tanks in which methyl isocyanate (MIC) was stored. The concrete storage tank, containing some 42 tons of this compound, which was used to manufacture pesticides, burst open and vented MIC and other breakdown chemicals into the air. Above and beyond the obvious catastrophic impact of the accident, questions still exist as to the possible long-term consequences for the health of those affected and/or exposed (Andersson et al. 1986; Sainani et al. 1985).
Slow-Onset Disasters
Slow-onset disasters may become apparent only because human targets happen to be on the release path, or because, as time passes, some environmental evidence of a threat from noxious materials crops up.
One of the most impressive and instructive examples of the first type is “Minamata disease”. In 1953 unusual neurological disorders began to strike people living in fishing villages along Minamata Bay, Japan. The disease was named kibyo, the “mystery illness”. After numerous investigations, poisoned fish emerged as the probable culprit, and in 1957 the disease was produced experimentally by feeding cats with fish caught in the bay. The following year, the suggestion was put forward that the clinical picture of kibyo, which included polyneuritis, cerebellar ataxia and cortical blindness, was similar to that due to poisoning by alkyl mercury compounds. A source of organic mercury had to be sought, and it was eventually found in a factory discharging its effluent into Minamata Bay. By July 1961, the disease had occurred in 88 persons, of whom 35 (40%) had died (Hunter 1978).
An example of the second type is Love Canal, an excavation site near Niagara Falls in the United States. The area had been used as a chemical and municipal disposal site over a period of about 30 years, until 1953. Homes were later built next to the landfill. In the late 1960s, there were complaints of chemical odours in home basements, and chemical leaching in areas surrounding the site began to be reported with increasing frequency over time. In the 1970s, residents began to fear that a serious threat to their health could arise, and this shared perception prompted environmental and health investigations to be carried out. None of the published studies could conclusively support a causal link between exposure to chemicals at the disposal site and adverse health effects among the residents. Yet, there is no doubt that serious social and psychological consequences have resulted among the population in the area, particularly those who were evacuated (Holden 1980).
Mass Food Poisonings
Outbreaks of food poisoning can be caused by toxic chemicals released into the environment through the use of chemicals in the handling and processing of food. One of the most serious episodes of this type occurred in Spain (Spurzem and Lockey 1984; WHO 1984; Lancet 1983). In May 1981, an outbreak of a previously unknown syndrome began to appear in the working-class suburbs of Madrid. Over 20,000 persons were ultimately involved.
By June 1982, 315 patients had died (around 16 deaths per 1,000 cases). Initially, the clinical features included interstitial pneumonitis, diverse skin rashes, lymphadenopathies, intense eosinophilia, and gastro-intestinal symptoms. Nearly one-fourth of those who survived the acute phase required later hospitalization for neuromuscular alterations. Schleroderma-like changes of the skin also were observed in this late stage along with pulmonary hypertension and Raynaud’s phenomenon.
One month after the occurrence of the first cases, the illness was found to be associated with the consumption of inexpensive denatured rapeseed oil, sold in unlabelled plastic containers and usually acquired from itinerant salesmen. The warning issued by the Spanish government against the consumption of the suspected oil caused a dramatic fall in the number of hospitalizations from toxic pneumonitis (Gilsanz et al. 1984; Kilbourne et al. 1983).
Polychlorinated biphenyls (PCBs) were involved in other widely reported accidental mass food poisonings in Japan (Masuda and Yoshimura 1984) and in Taiwan (Chen et al. 1984).
Transnational Disasters
Today’s human-made disasters do not necessarily respect national political boundaries. An obvious example is Chernobyl, whose contamination reached from the Atlantic Ocean to the Ural Mountains (Nuclear Energy Agency, 1987). Another example comes from Switzerland (Friedrich Naumann Foundation 1987; Salzman 1987). On 1 November 1986, shortly after midnight, a fire developed in a warehouse operated by the multinational pharmaceutical company Sandoz in Schweizerhalle, 10 km southeast of Basel, and some 30 tons of the chemicals stored in the warehouse were drained along with water from the fire-fighting into the nearby River Rhine. Severe ecological damage occurred over a length of about 250 km. Apart from symptoms of irritation reported in the parts of the Basel area reached by gases and vapours produced by the fire, no cases of serious illness were reported. Nonetheless, this accident triggered serious concern in at least four European countries (Switzerland, France, Germany, The Netherlands).
Transnationality applies not only to consequences and harm caused by disasters, but also to their remote causes. Bhopal might serve as an example. In analysing the causes of that disaster, some persons reached the conclusion that “The Bhopal disaster occurred because of specific acts and decisions which were taken in Danbury, Connecticut or elsewhere in the corporate superstructure, but not in Bhopal.” (Friedrich Naumann Foundation 1987.)
“Developing” Disasters
The emerging pattern of industrialization as well as modernization of agriculture in developing countries involves the application and use of imported or adopted technology and products, within contexts which are quite different from those in which they were intended to be used. Businesses facing the tightening of regulations in industrial countries may export hazardous industries to world regions where less stringent measures for protection of the environment and public health exist. Industrial activities become concentrated in existing urban settlements and add significantly to the pressure caused by overcrowding and shortages of community services. Such activities are distributed between a small highly organized sector and a large unorganized sector; governmental controls in regard to labour and environmental safety in the latter sector are less stringent (Krishna Murti 1987). An example comes from Pakistan, where among 7,500 field workers in a malaria control programme in 1976, as many as 2,800 experienced some form of toxicity (Baker et al. 1978). It was also estimated that about 500,000 acute pesticide poisonings occur annually, resulting in about 9,000 deaths, and that only about 1% of the deadly cases occur in industrialized countries, although those countries consume about 80% of the total world agrochemical production (Jeyaratnam 1985).
It has also been argued that developing societies might actually find themselves carrying a double burden instead of being cleared from the one of underdevelopment. It could be, in fact, that the consequences of improper industrialization are simply being added to those of the countries’ underdeveloped states (Krishna Murti 1987). It is clear, thus, that international cooperation ought to be urgently strengthened in three domains: scientific work, public health and industrial siting and safety policies.
Lessons for the Future
Despite the variety of the reviewed industrial disasters, some common lessons have been learned on how to prevent their occurrence, and also on how to mitigate the impact of major chemical disasters on the population. In particular:
- Different experts should be on the scene working in close coordination; they should usually cover the fields related to the environmental fate of the agent, its toxic properties to humans and biota, analytical methods, clinical medicine and pathology, biostatistics and epidemiology.
- Based on pre-existing and/or early available evidence, a comprehensive study plan should be developed as early as possible to identify goals, problems and resource requirements.
- Early phase activities affect the course of any subsequent action. Since long-term effects should be expected after virtually every type of industrial disaster, great care should be devoted to insure availability of requisite information for later studies (e.g., proper identifiers of the exposed for follow-up).
- In planning long-term investigations, feasibility should be given high consideration to facilitate scientific and public health achievements and clarity of communication.
- Overall, for reasons of validity and cost effectiveness, it is advisable to rely on “hard” information, whenever available, either in identifying and enumerating the study population (e.g., residence) or in estimating exposure (e.g., environmental and biological measurements) and choosing the endpoints (e.g., mortality).
Control of Major Hazard Installations for the Prevention of Major Accidents
The objective of this article is to provide guidance for establishing a system to control major hazard installations. Two ILO documents and the more recent ILO Convention (see "ILO Convention") form the basis of the first part of this article. The European Directive forms the basis for the second part of this article.
The ILO Perspective
Much of what follows has been extracted from two documents Prevention of Major Industrial Accidents (ILO 1991) and Major Hazard Control: A Practical Manual (ILO 1988). The document “Convention concerning the Prevention of Major Industrial Accidents” (ILO 1993) (see "ILO Convention") serves to complement and update material from the earlier two documents. Each of these documents proposes ways to protect workers, the public and the environment against the risk of major accidents by (1) preventing major accidents from occurring at these installations and (2) minimizing the consequences of a major accident onsite and offsite, for example by (a) arranging appropriate separation between major hazard installations and housing and other centres of population nearby, such as hospitals, schools and shops, and (b) appropriate emergency planning.
The 1993 ILO Convention should be referred to for specifics; what follows is more of a narrative overview of the document.
Major hazard installations possess the potential, by virtue of the nature and quantity of hazardous substances present, to cause a major accident in one of the following general categories:
- the release of toxic substances in tonnage quantities which are lethal or harmful even at considerable distances from the point of release through contamination of air, water and/or soil
- the release of extremely toxic substances in kilogram quantities, which are lethal or harmful even at considerable distance from the point of release
- the release of flammable liquids or gases in tonnage quantities, which may either burn to produce high levels of thermal radiation or form an explosive vapour cloud
- the explosion of unstable or reactive materials.
Member country obligations
The 1993 Convention expects member countries who are not immediately able to implement all of the preventive and protective measures provided for in the Convention:
- to draw up plans, in consultation with the most representative organizations of employers and workers, and with other interested parties who may be affected, for the progressive implementation of said measures within a fixed time-frame
- to implement and periodically review a coherent national policy concerning the protection of workers, the public and the environment against the risk of major accidents
- to implement the policy through preventive and protective measures for major hazard installations and, where, practicable, promote the use of the best available safety technologies and
- to apply the Convention in accordance with national law and practice.
Components of a major hazard control system
The variety of major accidents leads to the concept of major hazard as an industrial activity requiring controls over and above those applied in normal factory operations, in order to protect both workers and people living and working outside. These controls aim not only at preventing accidents but also at mitigating the consequences of any accidents which could occur.
Controls need to be based on a systematic approach. Basic components of this system are:
- identification of major hazard installations together with their respective threshold quantities and inventory. Governmental authorities and employers should require the identification of major hazard installations on a priority basis; these should be regularly reviewed and updated.
- information about the installation. Once the major hazard installations have been identified, additional information needs to be collected about their design and operation. The information should be gathered and arranged systematically, and should be accessible to all parties concerned within the industry and outside the industry. In order to achieve a complete description of the hazards, it may be necessary to carry out safety studies and hazard assessments to discover possible process failures and to set priorities during the process of hazard assessment.
- special provision to protect confidential information
- action inside the industrial activity. Employers have the primary responsibility for operating and maintaining a safe facility. A sound safety policy is required. Technical inspection, maintenance, facility modification, training and selecting of suitable personnel must be carried out according to standard quality control procedures for major hazard installations. In addition to the preparation of the safety report, accidents of any type should be investigated and copies of reports submitted to the competent authority.
- actions by the government or other competent authorities. Assessment of the hazards for the purposes of licensing (where appropriate), inspection and enforcement of legislation. Land-use planning can appreciably reduce the potential for a disaster. The training of factory inspectors also is an important role of the government or other competent authority.
- emergency planning. This aims at the reduction of the consequences of major accidents. In setting up emergency planning, a distinction is made between onsite and offsite planning.
The responsibilities of employers
Major hazard installations have to be operated at a very high standard of safety. In addition, employers play a key role in the organization and implementation of a major hazard control system. In particular, as outlined in table 13, employers have the responsibility to:
- Provide the information required to identify major hazard installations within a fixed time-frame.
- Carry out the hazard assessment.
- Report to the competent authority on the results of the hazard assessment.
- Introduce technical measures, including design, safety systems construction, choice of chemicals, operation, maintenance and systematic inspection of the installation.
- Introduce organizational measures, including, among others, training and instruction of personnel and staffing levels.
- Set up an emergency plan.
- Take measures to improve plant safety and limit the consequences of an accident.
- Consult with workers and their representatives.
- Improve the system by learning from near misses and related information.
- Ensure that quality control procedures are in effect and audit these periodically.
- Notify the competent authority before any permanent closure of a major hazard installation.
Table 13. The role of major hazard installations management in hazard control
|
Actions (depending on local legislation) |
Action in the event of a major |
|||
|
Provide notification to authorities |
Provide information on |
Prepare an onsite emergency plan |
Inform the public about the major hazard |
Notify authority about major accident |
|
Prepare and submit safety report |
Provide further information on request |
Provide information to local authority to enable it to draw |
Provide information on major accident |
|
First and foremost, employers of installations which can cause a major accident have a duty to control this major hazard. To do this, they must be aware of the nature of the hazard, of the events that cause accidents, and of the potential consequences of such accidents. This means that, in order to control a major hazard successfully, employers must have answers to the following questions:
- Do toxic, explosive or flammable substances in the facility constitute a major hazard?
- Do chemicals or agents exist which, if combined, could become a toxic hazard?
- Which failures or errors can cause abnormal conditions leading to a major accident?
- If a major accident occurs, what are the consequences of a fire, an explosion or a toxic release for the employees, people living outside the facility, the plant or the environment?
- What can management do to prevent these accidents from happening?
- What can be done to mitigate the consequences of an accident?
Hazard assessment
The most appropriate way to answer the above questions is to carry out a hazard assessment, the purpose of which is to understand why accidents occur and how they can be avoided or at least mitigated. Methods which can be used for an assessment are summarized in table 14.
Table 14. Working methods for hazard assessment
|
Method |
Purpose |
Aim |
Working principle |
|
1. Preliminary hazard analysis |
1. Identification of hazards |
1. Completeness of safety concept |
1. Use of “thinking aids” |
|
2. Matrix diagrams of |
|||
|
3. Use of check-lists |
|||
|
4. Failure effect |
2. Use of “searching |
||
|
5. Hazard and |
|||
|
6. Accident sequence |
2. Assessment of hazard according to |
2. Optimization of |
3. Graphic description |
|
7. Fault tree analysis |
|||
|
8. Accident consequence analysis |
3. Assessment of accident consequences |
3. Mitigation of |
4. Mathematical |
Source: ILO 1988.
Safe operation
A general outline of how the hazards should be controlled will be given.
Plant component design
A component has to withstand the following: static loads, dynamic loads, internal and external pressure, corrosion, loads arising from large differences in temperature, loads arising from external impacts (wind, snow, earthquakes, settling). Design standards are therefore a minimum requirement as far as major hazard installations are concerned.
Operation and control
When an installation is designed to withstand all loads that can occur during normal or foreseen abnormal operating conditions, it is the task of a process control system to keep the plant safely within these limits.
In order to operate such control systems, it is necessary to monitor the process variables and active parts of the plant. Operating personnel should be well trained to be aware of the mode of operation and the importance of the control system. To ensure that the operating personnel do not have to rely solely on the functioning of automatic systems, these systems should be combined with acoustic or optical alarms.
It is most important to realize that any control system will have problems in rare operating conditions such as start-up and shut-down phases. Special attention must be paid to these phases of operation. Quality control procedures will be audited by management periodically.
Safety systems
Any major hazard installation will require some form of safety system. The form and design of the system depend on the hazards present in the plant. The following gives a survey of available safety systems:
- systems preventing deviation from permissible operating conditions
- systems preventing failure of safety-related components
- safety-related utility supplies
- alarm systems
- technical protective measures
- prevention of human and organizational errors.
Maintenance and monitoring
The safety of a plant and the function of a safety-related system can only be as good as the maintenance and monitoring of these systems.
Inspection and repair
It is necessary to establish a plan for onsite inspections, for the operating personnel to follow, which should include a schedule and the operating conditions to be adhered to during inspection work. Strict procedures must be specified for carrying out repair work.
Training
As people can have a negative as well as a positive influence on plant safety, it is important to reduce the negative influences and support the positive ones. Both goals can be achieved by proper selection, training and periodic evaluation/assessment of the personnel.
Mitigation of consequences
Even if a hazard assessment has been carried out and the hazards have been detected and appropriate measures to prevent accidents have been taken, the possibility of an accident cannot be completely ruled out. For this reason, it must be part of the safety concept to plan and provide measures which can mitigate the consequences of an accident.
These measures have to be consistent with the hazards identified in the assessment. Furthermore, they must be accompanied by proper training of plant personnel, the emergency forces and responsible representatives from public services. Only training and rehearsals of accident situations can make emergency plans realistic enough to work in a real emergency.
Safety reporting to the competent authority
Depending on local arrangements in different countries, employers of a major hazard installation shall report to the appropriate competent authority. Reporting may be carried out in three steps. These are:
- identification/notification of major hazard installation (including any future changes that are to be made to the installation)
- the preparation of periodic safety reports (which shall be revised in the light of any modifications made to a facility)
- immediate reporting of any type of accident, followed by a detailed report.
Rights and duties of workers and their representatives
Workers and their representatives shall be consulted through appropriate cooperative mechanisms in order to ensure a safe system of work. They shall be consulted in the preparation of, and have access to, safety reports, emergency plans and procedures, and accident reports. They shall receive training for preventing major accidents and in emergency procedures to be followed in the event of a major accident. Finally, workers and their representatives should be able to take corrective action where needed within the scope of their duties, if they believe that there is any imminent danger of a major accident. They also have the right to notify the competent authority of any hazard.
Workers shall comply with all practices and procedures for preventing major accidents and for the control of developments likely to lead to a major accident. They shall comply with all emergency procedures should a major accident occur.
Implementation of a major hazard control system
Although the storage and use of large quantities of hazardous materials is widespread across most countries of the world, the present systems for their control will differ substantially from one country to another. This means that the speed of implementation of a major hazard control system will depend on the facilities already existing in each country, particularly with regard to trained and experienced facility inspectors, together with the resources available locally and nationally for the different components of the control system. For all countries, however, implementation will require the setting of priorities for a stage-by-stage programme.
Identification of major hazards
This is the essential starting point for any major hazard control system—the definition of what actually constitutes a major hazard. Although definitions exist in some countries and particularly in the EU, a particular country’s definition of a major hazard should reflect local priorities and practices and, in particular, the industrial pattern in that country.
Any definition for identifying major hazards is likely to involve a list of hazardous materials, together with an inventory for each, such that any major hazard installation storing or using any of these in excess quantities is by definition a major hazard installation. The next stage is to identify where the major hazard installation exists for any particular region or country. Where a country wishes to identify major hazard installations before the necessary legislation is in place, considerable progress can be achieved informally, particularly where the cooperation of industry is available. Existing sources such as factory inspectorate records, information from industrial bodies and so on, may enable a provisional list to be obtained which, apart from allowing early inspection priorities to be allocated, will enable an assessment to be made of the resources required for different parts of the control system.
Establishment of a group of experts
For countries considering establishing a major hazard control system for the first time, an important first stage is likely to be setting up a group of experts as a special unit at government level. The group will have to set priorities in deciding on its initial programme of activity. The group may be required to train factory inspectors in the techniques of major hazard inspection, including operational standards for such major hazard installations. They should also be able to provide advice about the siting of new major hazards and the use of land nearby. They will need to establish contacts in other countries in order to keep up to date with major hazard developments.
Onsite emergency preparedness
Emergency plans require that the major hazard installation be assessed for the range of accidents that could take place, together with how they would be tackled in practice. The handling of these potential accidents will require both staff and equipment, and a check should be made to ensure that both are available in sufficient numbers. The plans should include the following elements:
- assessment of the size and nature of the events foreseen and the probability of their occurrence
- formulation of the plan and liaison with outside authorities, including emergency services
- procedures: (a) raising the alarm; (b) communications within the plant and outside the plant
- appointment of key personnel and their duties and responsibilities
- emergency control centre
- action onsite and offsite.
Offsite emergency preparedness
This is an area which has received less attention than onsite emergency planning, and many countries will be faced with considering this for the first time. The offsite emergency plan will have to link the possible accidents identified by the major hazard installation, their expected likelihood of occurrence and the proximity of people living and working nearby. It must have addressed the need for the expeditious warning and evacuation of the public, and how these might be achieved. It should be remembered that conventional housing of solid construction offers substantial protection from toxic gas clouds, whereas a shanty-type house is vulnerable to such accidents.
The emergency plan must identify organizations whose help will be required in the event of an emergency and must ensure that they know what role is expected of them: hospitals and medical staff should, for example, have decided how they would handle large numbers of casualties and in particular what treatment they would provide. The offsite emergency plan will need to be rehearsed with public involvement from time to time.
Where a major accident could have transboundary effects, full information is to be provided to the jurisdictions concerned, as well as assistance in cooperation and coordination arrangements.
Siting
The basis for needing a siting policy for major hazard installations is straightforward: since absolute safety cannot be guaranteed, major hazard installations should be separated from people living and working outside the facility. As a first priority, it may be appropriate to concentrate efforts on proposed new major hazards and to try to prevent the encroachment of housing, particularly shanty houses, which are a common feature in many countries.
Training and facility inspectors
The role of the facility inspectors is likely to be central in many countries in implementing a major hazard control system. Facility inspectors will have the knowledge that will enable early identification of major hazards to take place. Where they have specialist inspectors to call upon, factory inspectors will be assisted in the often highly technical aspects of major hazard inspection.
Inspectors will need appropriate training and qualifications to aid them in this work. Industry itself is likely to be the largest source of technical expertise within many countries, and may be able to provide assistance in facility inspectorate training.
The competent authority shall have the right to suspend any operation which poses an imminent threat of a major accident.
Evaluation of major hazards
This should be carried out by specialists, if possible according to guidelines drawn up, for example, by the group of experts or by specialist inspectors, possibly with assistance from the major hazard installation employer management group. Evaluation involves a systematic study for major accident hazard potential. It will be a similar exercise, although in much less detail, to that carried out by the major hazard installation management in producing its safety report for the facility inspectorate and in establishing an onsite emergency plan.
Evaluation will include a study of all handling operations of hazardous materials, including transport.
An examination of the consequences of process instability or major changes in the process variables will be included.
The evaluation also should consider the positioning of one hazardous material in relation to another.
The consequences of common mode failure will also need to be assessed.
The evaluation will consider the consequences of the identified major accidents in relation to offsite populations; this may determine whether the process or plant can be put into operation.
Information to the public
Experience of major accidents, particularly those involving toxic gas releases, has shown the importance of the public nearby having prior warning of: (a) how to recognize that an emergency is occurring; (b) what action they should take; and (c) what remedial medical treatment would be appropriate for anyone being affected by the gas.
For inhabitants of conventional housing of solid construction, the advice in the event of an emergency usually is to go indoors, close all doors and windows, switch off all ventilation or air conditioning, and switch on the local radio for further instructions.
Where large numbers of shanty-dwellers live close to a major hazard installation, this advice would be inappropriate, and large-scale evacuation might be necessary.
Prerequisites for a major hazard control system
Personnel
A fully developed major hazard control system requires a wide variety of specialized personnel. Apart from industrial staff concerned either directly or indirectly with the safe operation of the major hazard installation, required resources include general factory inspectors, specialist inspectors, risk assessors, emergency planners, quality control officers, local authority land planners, police, medical facilities, river authorities and so on, plus legislators to promulgate new legislation and regulations for major hazard control.
In most countries, human resources for these tasks are likely to be limited, and the setting of realistic priorities is essential.
Equipment
A feature of establishing a major hazard control system is that much can be achieved with very little equipment. Factory inspectors will not need much in addition to their existing safety equipment. What will be required is the acquisition of technical experience and knowledge and the means to relay this from the group of experts to, say, the regional labour institute, the facility inspectorate and the industry. Additional training aids and facilities may be necessary.
Information
A key element in establishing a major hazard control system is obtaining state-of-the-art information and quickly passing this information on to all those who will need it for their safety work.
The volume of literature covering the various aspects of major hazards work is now considerable, and, used selectively, this could provide an important source of information to a group of experts.
Responsibility of exporting countries
When, in an exporting member country, the use of hazardous substances, technologies or processes is prohibited as a potential source of a major accident, the information on this prohibition and the reasons for it shall be made available by the exporting member country to any importing country.
Certain non-binding recommendations flowed from the Convention. In particular, one had a transnational focus. It recommends that a national or a multinational enterprise with more than one establishment or facility should provide safety measures relating to the prevention of major accidents and the control of developments likely to lead to a major accident, without discrimination, to the workers in all its establishments, regardless of the place or country in which they are situated. (The reader should also refer to the section “Transnational disasters” in this article.)
The European Directive on Major Accident Hazards of Certain Industrial Activities
Following serious incidents in the chemical industry in Europe in the last two decades, specific legislation covering major hazard activities was developed in various countries in Western Europe. A key feature in the legislation was the obligation of the employer of a major hazard industrial activity to submit information about the activity and its hazards based on the results of systematic safety studies. After the accident in Seveso (Italy) in 1976, the major hazard regulations in the various countries were put together and integrated in an EC Directive. This Directive, on the major accident hazards of certain industrial activities, has been in force since 1984 and is often referred to as the Seveso Directive (Council of the European Communities 1982, 1987).
For the purpose of identifying major hazard installations, the EC Directive uses criteria based on the toxic, flammable and explosive properties of the chemicals (see table 15).
Table 15. EC Directive criteria for major hazard installations
|
Toxic substances (very toxic and toxic): |
|||
|
Substances showing the following values of acute toxicity and having physical and chemical properties capable of entailing major accident hazards: |
|||
|
LD50 oral. rat mg/kg |
LD50 cut. rat/rab mg/kg |
LC50 ihl. 4hr. rat mg/1 |
|
|
1. |
LD50 <5 |
LD <1 |
LD50 <0.10 |
|
2. |
5<LD50 <25 |
10 <LD50 <50 |
0.1<LC50 <0.5 |
|
3. |
25 <LD50 <200 |
50 <LD50 <400 |
0.5 <LC50 <2 |
|
Flammable substances: |
|||
|
1. |
Flammable gases: substances which in the gaseous state at normal pressure and mixed with air become flammable and the boiling-point of which at normal pressure is 20 ºC or below. |
||
|
2. |
Highly flammable liquids: substances which have a flashpoint lower than 21 °C and the boiling point of which at normal pressure is above 20 °C. |
||
|
3. |
Flammable liquids: substances which have a flashpoint lower than 55 °C and which remain liquid under pressure, where particular processing conditions, such as high pressure and high temperature, may create major accident hazards. |
||
|
Explosive substances: |
|||
|
Substances which may explode under the effect of flame or which are more sensitive to shocks or friction than dinitrobenzene. |
|||
For the selection of specific major hazard industrial activities, a list of substances and threshold limits is provided in annexes to the Directive. An industrial activity is defined by the Directive as the aggregate of all installations within a distance of 500 metres of each other and belonging to the same factory or plant. When the quantity of the substances present exceeds the given threshold limit appearing in the list, the activity is referred to as a major hazard installation. The list of substances consists of 180 chemicals, whereas the threshold limits vary between 1 kg for extremely toxic substances to 50,000 tonnes for highly flammable liquids. For isolated storage of substances, a separate list of a few substances is given.
In addition to flammable gases, liquids and explosives, the list contains chemicals such as ammonia, chlorine, sulphur dioxide and acrylonitrile.
In order to facilitate the application of a major hazard control system and to encourage the authorities and management to apply it, it must be priority oriented, with attention being focused on the more hazardous installations. A suggested list of priorities is given in table 16.
Table 16. Priority chemicals used in identifying major hazard installations
|
Names of substances |
Quantity (>) |
EC list serial number |
|
General flammable substances: |
||
|
Flammable gases |
200 t |
124 |
|
Highly flammable liquids |
50,000 t |
125 |
|
Specific flammable substances: |
||
|
Hydrogen |
50 t |
24 |
|
Ethylene oxide |
50 t |
25 |
|
Specific explosives: |
||
|
Ammonium nitrate |
2,500 t |
146 b |
|
Nitroglycerine |
10 t |
132 |
|
Trinitrotoluene |
50 t |
145 |
|
Specific toxic substances: |
||
|
Acrylonitrile |
200 t |
18 |
|
Ammonia |
500 t |
22 |
|
Chlorine |
25 t |
16 |
|
Sulphur dioxide |
250 t |
148 |
|
Hydrogen sulphide |
50 t |
17 |
|
Hydrogen cyanide |
20 t |
19 |
|
Carbon disulphide |
200 t |
20 |
|
Hydrogen fluoride |
50 t |
94 |
|
Hydrogen chloride |
250 t |
149 |
|
Sulphur trioxide |
75 t |
180 |
|
Specific very toxic substances: |
||
|
Methyl isocyanate |
150 kg |
36 |
|
Phosgene |
750 kg |
15 |
With the chemicals shown in the table acting as a guide, a list of installations can be identified. If the list is still too big to be coped with by the authorities, new priorities can be set by means of setting new quantity thresholds. Priority setting also can be used inside the factory to identify the more hazardous parts. In view of the diversity and complexity of industry in general, it is not possible to restrict major hazard installations to certain sectors of industrial activity. Experience, however, indicates that major hazard installations are most commonly associated with the following activities:
- petrochemical works and refineries
- chemical works and chemical production plants
- LPG storage and terminals
- stores and distribution centres for chemicals
- large fertilizer stores
- explosives factories
- works in which chlorine is used in bulk quantities.