- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Major Sectors and Their Hazards

Health, Prevention and Management
Health and Safety Hazards in the Construction Industry
Construction workers build, repair, maintain, renovate, modify and demolish houses, office buildings, temples, factories, hospitals, roads, bridges, tunnels, stadiums, docks, airports and more. The International Labour Organization (ILO) classifies the construction industry as government and private-sector firms erecting buildings for habitation or for commercial purposes and public works such as roads, bridges, tunnels, dams or airports. In the United States and some other countries, construction workers also clean hazardous waste sites.
Construction as a proportion of gross domestic product varies widely in industrialized countries. It is about 4% of GDP in the United States, 6.5% in Germany and 17% in Japan. In most countries, employers have relatively few full-time employees. Many companies specialize in skilled trades—electricity, plumbing or tile setting, for instance—and work as subcontractors.
The Construction Labour Force
A large portion of construction workers are unskilled labourers; others are classified in any of several skilled trades (see table 1). Construction workers include about 5 to 10% of the workforce in industrialized countries. Throughout the world, over 90% of construction workers are male. In some developing countries, the proportion of women is higher and they tend to be concentrated in unskilled occupations. In some countries, the work is left to migrant workers, and in others, the industry provides relatively well-paid employment and an avenue to financial security. For many, unskilled construction work is the entry into the paid labour force in construction or other industries.
Work Organization and Labour Instability
Construction projects, especially large ones, are complex and dynamic. Several employers may work on one site simultaneously, with the mix of contractors changing with the phases of the project; for example, the general contractor is present at all times, excavating contractors early, then carpenters, electricians and plumbers, followed by floor finishers, painters and landscapers. And as the work develops—for instance, as a building’s walls are erected, as the weather changes or as a tunnel advances—the ambient conditions such as ventilation and temperature change too.
Construction workers typically are hired from project to project and may spend only a few weeks or months at any one project. There are consequences for both workers and work projects. Workers must make and remake productive and safe working relationships with other workers whom they may not know, and this may affect safety at the work site. And in the course of the year, construction workers may have several employers and less than full employment. They might work an average of only 1,500 hours in a year while workers in manufacturing, for example, are more likely to work regular 40 hour weeks and 2,000 hours per year. In order to make up for slack time, many construction workers have other jobs—and exposure to other health or safety hazards—outside of construction.
For a particular project, there is frequent change in the number of workers and the composition of the labour force at any one site. This change results both from the need for different skilled trades at different phases of a work project and from the high turnover of construction workers, particularly unskilled workers. At any one time, a project may include a large proportion of inexperienced, temporary and transient workers who may not be fluent in the common language. Although construction work often must be done in teams, it is difficult to develop effective, safe teamwork under such conditions.
Like the workforce, the universe of construction contractors is marked by high turnover and consists mainly of small operations. Of the 1.9 million construction contractors in the United States identified by the 1990 Census, only 28% had any full-time employees. Just 136,000 (7%) had 10 or more employees. The degree of contractor participation in trade organizations varies by country. In the United States, only about 10 to 15% of contractors participate; in some European countries, this proportion is higher but still involves less than half of contractors. This makes it difficult to identify contractors and inform them of their rights and responsibilities under pertinent health and safety or any other legislation or regulations.
As in some other industries, an increasing proportion of contractors in the United States and Europe consists of individual workers hired as independent contractors by prime- or sub-contractors who employ workers. Ordinarily, an employing contractor does not provide subcontractors with health benefits, workers’ compensation coverage, unemployment insurance, pension benefits or other benefits. Nor do prime contractors have any obligation to subcontractors under health and safety regulations; these regulations govern rights and responsibilities as they apply to their own employees. This arrangement gives some independence to individuals who contract for their services, but at the cost of removing a wide range of benefits. It also relieves employing contractors of the obligation to provide mandated benefits to individuals who are contractors. This private arrangement subverts public policy and has been successfully challenged in court, yet it persists and may become more of a problem for the health and safety of workers on the job, regardless of their employment relationship. The US Bureau of Labor Statistics (BLS) estimates that 9% of the US workforce is self-employed, but in construction as many as 25% of workers are self-employed independent contractors.
Health Hazards on Construction Sites
Construction workers are exposed to a wide variety of health hazards on the job. Exposure differs from trade to trade, from job to job, by the day, even by the hour. Exposure to any one hazard is typically intermittent and of short duration, but is likely to reoccur. A worker may not only encounter the primary hazards of his or her own job, but may also be exposed as a bystander to hazards produced by those who work nearby or upwind. This pattern of exposure is a consequence of having many employers with jobs of relatively short duration and working alongside workers in other trades that generate other hazards. The severity of each hazard depends on the concentration and duration of exposure for that particular job. Bystander exposures can be approximated if one knows the trade of workers nearby. Hazards present for workers in particular trades are listed in table 2.
Table 2. Primary hazards encountered in skilled construction trades.
Each trade is listed below with an indication of the primary hazards to which a worker in that trade might be exposed. Exposure may occur to either supervisors or to wage earners. Hazards that are common to nearly all construction-heat, risk factors for musculoskeletal disorders and stress-are not listed.
The classifications of construction trades used here are those used in the United States. It includes the construction trades as classified in the Standard Occupational Classification system developed by the US Department of Commerce. This system classifies the trades by the principal skills inherent in the trade.
|
Occupations |
Hazards |
|
Brickmasons |
Cement dermatitis, awkward postures, heavy loads |
|
Stonemasons |
Cement dermatitis, awkward postures, heavy loads |
|
Hard tile setters |
Vapour from bonding agents, dermatitis, awkward postures |
|
Carpenters |
Wood dust, heavy loads, repetitive motion |
|
Drywall installers |
Plaster dust, walking on stilts, heavy loads, awkward postures |
|
Electricians |
Heavy metals in solder fumes, awkward posture, heavy loads, asbestos dust |
|
Electrical power installers and repairers |
Heavy metals in solder fumes, heavy loads, asbestos dust |
|
Painters |
Solvent vapours, toxic metals in pigments, paint additives |
|
Paperhangers |
Vapours from glue, awkward postures |
|
Plasterers |
Dermatitis, awkward postures |
|
Plumbers |
Lead fumes and particles, welding fumes |
|
Pipefitters |
Lead fumes and particles, welding fumes, asbestos dust |
|
Steamfitters |
Welding fumes, asbestos dust |
|
Carpet layers |
Knee trauma, awkward postures, glue and glue vapour |
|
Soft tile installers |
Bonding agents |
|
Concrete and terrazzo finishers |
Awkward postures |
|
Glaziers |
Awkward postures |
|
Insulation workers |
Asbestos, synthetic fibres, awkward postures |
|
Paving, surfacing and tamping equipment operators |
Asphalt emissions, gasoline and diesel engine exhaust, heat |
|
Rail- and track-laying equipment operators |
Silica dust, heat |
|
Roofers |
Roofing tar, heat, working at heights |
|
Sheetmetal duct installers |
Awkward postures, heavy loads, noise |
|
Structural metal installers |
Awkward postures, heavy loads, working at heights |
|
Welders |
Welding emissions |
|
Solderers |
Metal fumes, lead, cadmium |
|
Drillers, earth, rock |
Silica dust, whole-body vibration, noise |
|
Air hammer operators |
Noise, whole-body vibration, silica dust |
|
Pile driving operators |
Noise, whole-body vibration |
|
Hoist and winch operators |
Noise, lubricating oil |
|
Crane and tower operators |
Stress, isolation |
|
Excavating and loading machine operators |
Silica dust, histoplasmosis, whole-body vibration, heat stress, noise |
|
Grader, dozer and scraper operators |
Silica dust, whole-body vibration, heat noise |
|
Highway and street construction workers |
Asphalt emissions, heat, diesel engine exhaust |
|
Truck and tractor equipment operators |
Whole-body vibration, diesel engine exhaust |
|
Demolition workers |
Asbestos, lead, dust, noise |
|
Hazardous waste workers |
Heat, stress |
Construction Hazards
As in other jobs, hazards for construction workers are typically of four classes: chemical, physical, biological and social.
Chemical hazards
Chemical hazards are often airborne and can appear as dusts, fumes, mists, vapours or gases; thus, exposure usually occurs by inhalation, although some airborne hazards may settle on and be absorbed through the intact skin (e.g., pesticides and some organic solvents). Chemical hazards also occur in liquid or semi-liquid state (e.g., glues or adhesives, tar) or as powders (e.g., dry cement). Skin contact with chemicals in this state can occur in addition to possible inhalation of the vapour resulting in systemic poisoning or contact dermatitis. Chemicals might also be ingested with food or water, or might be inhaled by smoking.
Several illnesses have been linked to the construction trades, among them:
- silicosis among sand blasters, tunnel builders and rock drill operators
- asbestosis (and other diseases caused by asbestos) among asbestos insulation workers, steam pipe fitters, building demolition workers and others
- bronchitis among welders
- skin allergies among masons and others who work with cement
- neurologic disorders among painters and others exposed to organic solvents and lead.
Elevated death rates from cancer of the lung and respiratory tree have been found among asbestos insulation workers, roofers, welders and some woodworkers. Lead poisoning occurs among bridge rehabilitation workers and painters, and heat stress (from wearing full-body protective suits) among hazardous-waste clean-up workers and roofers. White finger (Raynaud’s syndrome) appears among some jackhammer operators and other workers who use vibrating drills (e.g., stoper drills among tunnellers).
Alcoholism and other alcohol-related disease is more frequent than expected among construction workers. Specific occupational causes have not been identified, but it is possible that it is related to stress resulting from lack of control over employment prospects, heavy work demands or social isolation due to unstable working relationships.
Physical hazards
Physical hazards are present in every construction project. These hazards include noise, heat and cold, radiation, vibration and barometric pressure. Construction work often must be done in extreme heat or cold, in windy, rainy, snowy, or foggy weather or at night. Ionizing and non-ionizing radiation is encountered, as are extremes of barometric pressure.
The machines that have transformed construction into an increasingly mechanized activity have also made it increasingly noisy. The sources of noise are engines of all kinds (e.g., on vehicles, air compressors and cranes), winches, rivet guns, nail guns, paint guns, pneumatic hammers, power saws, sanders, routers, planers, explosives and many more. Noise is present on demolition projects by the very activity of demolition. It affects not only the person operating a noise-making machine, but all those close-by and not only causes noise-induced hearing loss, but also masks other sounds that are important for communication and for safety.
Pneumatic hammers, many hand tools and earth-moving and other large mobile machines also subject workers to segmental and whole-body vibration.
Heat and cold hazards arise primarily because a large portion of construction work is conducted while exposed to the weather, the principal source of heat and cold hazards. Roofers are exposed to the sun, often with no protection, and often must heat pots of tar, thus receiving both heavy radiant and convective heat loads in addition to metabolic heat from physical labour. Heavy equipment operators may sit beside a hot engine and work in an enclosed cab with windows and without ventilation. Those that work in an open cab with no roof have no protection from the sun. Workers in protective gear, such as that needed for removal of hazardous waste, may generate metabolic heat from hard physical labour and get little relief since they may be in an air-tight suit. A shortage of potable water or shade contributes to heat stress as well. Construction workers also work in especially cold conditions during the winter, with danger of frostbite and hypothermia and risk of slipping on ice.
The principal sources of non-ionizing ultraviolet (UV) radiation are the sun and electric arc welding. Exposure to ionizing radiation is less common, but can occur with x-ray inspection of welds, for example, or it may occur with instruments such as flow meters that use radioactive isotopes. Lasers are becoming more common and may cause injury, especially to the eyes, if the beam is intercepted.
Those who work under water or in pressurized tunnels, in caissons or as divers are exposed to high barometric pressure. Such workers are at risk of developing a variety of conditions associated with high pressure: decompression sickness, inert gas narcosis, aseptic bone necrosis and other disorders.
Strains and sprains are among the most common injuries among construction workers. These, and many chronically disabling musculoskeletal disorders (such as tendinitis, carpal tunnel syndrome and low-back pain) occur as a result of either traumatic injury, repetitive forceful movements, awkward postures or overexertion (see figure 1). Falls due to unstable footing, unguarded holes and slips off scaffolding (see figure 2) and ladders are very common.
Figure 1. Carrying without appropriate work clothing and protective equipment.
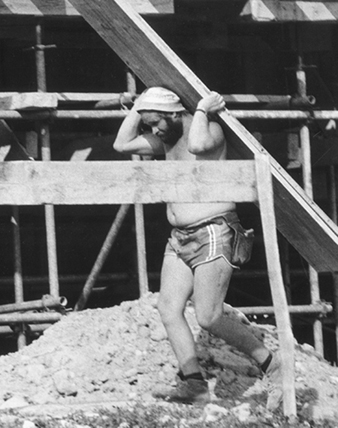
Figure 2. Unsafe scaffolding in Kathmandu, Nepal, 1974

Jane Seegal
Biological hazards
Biological hazards are presented by exposure to infectious micro-organisms, to toxic substances of biological origin or animal attacks. Excavation workers, for example, can develop histoplasmosis, an infection of the lung caused by a common soil fungus. Since there is constant change in the composition of the labour force on any one project, individual workers come in contact with other workers and, as a consequence, may become infected with contagious diseases—influenza or tuberculosis, for example. Workers may also be at risk of malaria, yellow fever or Lyme disease if work is conducted in areas where these organisms and their insect vectors are prevalent.
Toxic substances of plant origin come from poison ivy, poison oak, poison sumac and nettles, all of which can cause skin eruptions. Some wood dusts are carcinogenic, and some (e.g., western red cedar) are allergenic.
Attacks by animals are rare but may occur whenever a construction project disturbs them or encroaches on their habitat. This could include wasps, hornets, fire ants, snakes and many others. Underwater workers may be at risk from attack by sharks or other fish.
Social hazards
Social hazards stem from the social organization of the industry. Employment is intermittent and constantly changing, and control over many aspects of employment is limited because construction activity is dependent on many factors over which construction workers have no control, such as the state of an economy or the weather. Because of the same factors, there can be intense pressure to become more productive. Since the workforce is constantly changing, and with it the hours and location of work, and many projects require living in work camps away from home and family, construction workers may lack stable and dependable networks of social support. Features of construction work such as heavy workload, limited control and limited social support are the very factors associated with increased stress in other industries. These hazards are not unique to any trade, but are common to all construction workers in one way or another.
Evaluating Exposure
Evaluating either primary or bystander exposure requires knowing the tasks being done and the composition of ingredients and by-products associated with each job or task. This knowledge usually exists somewhere (e.g., material safety data sheets, MSDSs) but may not be available at the job site. With continually evolving computer and communications technology, it is relatively easy to obtain such information and make it available.
Controlling Occupational Hazards
Measuring and evaluating exposure to occupational hazards requires consideration of the novel manner in which construction workers are exposed. Conventional industrial hygiene measurements and exposure limits are based on 8-hour time-weighted averages. But since exposures in construction are usually brief, intermittent, varied but likely to be repeated, such measures and exposure limits are not as useful as in other jobs. Exposure measurement can be based on tasks rather than shifts. With this approach, separate tasks can be identified and hazards characterized for each. A task is a limited activity such as welding, soldering, sanding drywall, painting, installing plumbing and so on. As exposures are characterized for tasks, it should be possible to develop an exposure profile for an individual worker with knowledge of the tasks he or she performed or was near enough to be exposed to. As knowledge of task-based exposure increases, one may develop task-based controls.
Exposure varies with the concentration of the hazard and the frequency and duration of the task. As a general approach to hazard control, it is possible to reduce exposure by reducing the concentration or the duration or frequency of the task. Since exposure in construction is already intermittent, administrative controls that rely on reducing the frequency or duration of exposure are less practical than in other industries. Consequently, the most effective way to reduce exposure is to reduce the concentration of hazards. Other important aspects of controlling exposure include provisions for eating and sanitary facilities and education and training.
Decreasing exposure concentration
For reducing exposure concentration, it is useful to consider the source, the environment in which a hazard occurs and the workers who are exposed. As a general rule, the closer controls are to a source, the more efficient and effective they are. Three general types of controls can be used to reduce the concentration of occupational hazards. These are, from most to least effective:
- engineering controls at the source
- environmental controls that remove the hazard from the environment
- personal protection provided to the worker.
Engineering controls
Hazards originate at a source. The most efficient way to protect workers from hazards is to change the primary source with some sort of engineering change. For example, a less hazardous substance can be substituted for one that is more hazardous. Non-respirable synthetic vitreous fibres can be substituted for asbestos, and water can be substituted for organic solvents in paints. Similarly, non-silica abrasives can replace sand in abrasive blasting (also known as sand blasting). Or a process can be fundamentally changed, such as by replacing pneumatic hammers with impact hammers that generate less noise and vibration. If sawing or drilling generates harmful dusts, particulate matter or noise, these processes could be done by shear cutting or punching. Technological improvements are reducing the risks of some musculoskeletal and other health problems. Many of the changes are straightforward—for example, a two-handed screwdriver with a longer handle increases torque on the object and reduces stress on the wrists.
Environmental controls
Environmental controls are used to remove a hazardous substance from the environment, if the substance is airborne, or to shield the source, if it is a physical hazard. Local exhaust ventilation (LEV) can be used at a particular job with a ventilation duct and a hood to capture the fumes, vapours or dust. However, since the location of tasks that emit toxic materials changes, and because the structure itself changes, any LEV would have to be mobile and flexible in order to accommodate these changes. Mobile truck-mounted dust collectors with fans and filters, independent power sources, flexible ducts and mobile water supplies have been used on many job sites to provide LEV for a variety of hazard-producing processes.
The simple and effective method for controlling exposure to radiant physical hazards (noise, ultraviolet (UV) radiation from arc welding, infrared radiant (IR) heat from hot objects) is to shield them with some appropriate material. Plywood sheets shield IR and UV radiation, and material that absorbs and reflects sound will provide some protection from noise sources.
Major sources of heat stress are weather and hard physical labour. Adverse effects from heat stress can be avoided through reductions in the workload, provision of water and adequate breaks in the shade and, possibly, night work.
Personal protection
When engineering controls or changes in work practices do not adequately protect workers, workers may need to use personal protective equipment (PPE) (see figure 3). In order for such equipment to be effective, workers must be trained in its use, and the equipment must fit properly and be inspected and maintained. Furthermore, if others who are in the vicinity may be exposed to the hazard, they should either be protected or prevented from entering the area.
Figure 3. Construction worker in Nairobi, Kenya, without foot protection or hard hat

The use of some personal controls can create problems. For instance, construction workers often perform as teams and thus have to communicate with each other, but respirators interfere with communication. And full-body protective gear can contribute to heat stress because it is heavy and because body heat is not allowed to dissipate.
Having protective gear without knowing its limitations can also give workers or employers the illusion that the workers are protected when, with certain exposure conditions, they are not protected. For instance, there are no gloves currently available that protect for more than 2 hours against methylene chloride, a common ingredient in paint strippers. And there are few data on whether gloves protect against solvent mixtures such as those containing both acetone and toluene or both methanol and xylene. The level of protection depends on how a glove is used. In addition, gloves are generally tested on one chemical at a time and rarely for more than 8 hours.
Eating and sanitary facilities
A lack of eating and sanitary facilities may also lead to increased exposures. Often, workers cannot wash before meals and must eat in the work zone, which means they may inadvertently swallow toxic substances transferred from their hands to food or cigarettes. A lack of changing facilities at a worksite may result in transport of contaminants from the workplace to a worker’s home.
Injuries and Illnesses in Construction
Fatal injuries
Because construction involves a large proportion of the workforce, construction fatalities also affect a large population. For instance, in the United States, construction represents 5 to 6% of the workforce but accounts for 15% of work-related fatalities—more than any other sector. The construction sector in Japan is 10% of the workforce but has 42% of the work-related deaths; in Sweden, the numbers are 6% and 13%, respectively.
The most common fatal injuries among construction workers in the United States are falls (30%), transportation accidents (26%), contact with objects or equipment (e.g., struck by an object or caught in machinery or materials) (19%) and exposure to harmful substances (18%), most of which (75%) are electrocutions from contact with electrical wiring, overhead power lines or electrically powered machinery or hand tools. These four types of events account for nearly all (93%) fatal injuries among construction workers in the United States (Pollack et al. 1996).
Among trades in the US, the rate of fatal injuries is highest among structural steel workers (118 fatalities per 100,000 full-time equivalent workers for 1992–1993 compared to a rate of 17 per 100,000 for other trades combined) and 70% of structural steel worker fatalities were from falls. Labourers experienced the greatest number of fatalities, with an annual average number of about 200. Overall, the rate of fatalities was highest for workers 55 years and older.
The proportion of fatalities by event differed for each trade. For supervisors, falls and transportation accidents accounted for about 60% of all fatalities. For carpenters, painters, roofers and structural steel workers, falls were most common, accounting for 50, 55, 70 and 69% of all fatalities for those trades, respectively. For operating engineers and excavating machine operators, transportation accidents were the most common causes, accounting for 48 and 65% of fatalities for those trades, respectively. Most of these were associated with dump trucks. Fatalities from improperly sloped or shored trenches continue to be a major cause of fatalities (McVittie 1995). The primary hazards in the skilled trades are listed in table 2.
A study of Swedish construction workers did not find a high overall work-related mortality rate, but did find high death rates for particular conditions (see table 3).
Table 3. Construction occupations with excess standardized mortality rates (SMRs)and standardized incidence rates (SIRs) for selected causes.
|
Occupation |
Significantly higher SMRs |
Significantly higher SIRs |
|
Bricklayers |
- |
Peritoneal tumour |
|
Concrete workers |
All causes,* all cancers,* stomach cancer, violent death,* accidental falls |
Lip cancer, stomach and larynx cancer,*a lung cancerb |
|
Crane drivers |
Violent death* |
- |
|
Drivers |
All causes,* cardiovascular* |
Lip cancer |
|
Insulators |
All causes,* lung cancer, pneumoconiosis, violent death* |
Peritoneal tumour, lung cancer |
|
Machine operators |
Cardiovascular,* other accidents |
- |
|
Plumbers |
All cancers,* lung cancer, pneumoconiosis |
All cancers, pleural tumour, lung cancer |
|
Rock workers |
All causes,* cardiovascular,* |
- |
|
Sheet metal workers |
All cancers,* lung cancer, accidental falls |
All cancers, lung cancer |
|
Woodworkers/carpenters |
- |
Nose and nasal sinus cancer |
* Cancers or causes of death are significantly higher in comparison to all other occupational groups combined. “Other accidents” includes typical work-related injuries.
a The relative risk for larynx cancer among concrete workers, compared to carpenters, is 3 times higher.
b The relative risk for lung cancer among concrete workers, compared to carpenters, is almost double.
Source: Engholm and Englund 1995.
Disabling or lost time injuries
In the United States and Canada, the most common causes of lost time injuries are overexertion; being struck by an object; falls to a lower level; and slips, trips and falls on the same level. The most common category of injury is strains and sprains, some of which become sources of chronic pain and impairment. The activities most often associated with lost time injuries are manual materials handling and installation (e.g., installing dry-wall, piping or ventilation duct-work). Injuries occurring in transit (e.g., walking, climbing, descending) are also common. Underlying many of these injuries is the problem of housekeeping. Many slips, trips and falls are caused by walking through construction debris.
Costs of Injuries and Illness
Occupational injuries and illnesses in construction are very costly. Estimates for the cost of injuries in construction in the US range from $10 billion to $40 billion annually (Meridian Research 1994); at $20 billion, the cost per construction worker would be US$3,500 yearly. Workers’ compensation premiums for three trades—carpenters, masons and structural iron workers— averaged 28.6% of payroll nationally in mid-1994 (Powers 1994). Premium rates vary enormously, depending on trade and jurisdiction. The average premium cost is several times higher than in most industrialized countries, where workers’ compensation insurance premiums range from 3 to 6% of payroll. In addition to workers’ compensation, there are liability insurance premiums and other indirect costs, including reduced work crew efficiency, clean-up (from a cave-in or collapse, for instance) or overtime necessitated by an injury. Such indirect costs can be several times the workers’ compensation award.
Management for Safe Construction Work
Effective safety programmes have several features in common. They are manifest throughout organizations, from the highest offices of a general contractor to project managers, supervisors, union officials and workers on the job. Codes of practice are conscientiously implemented and evaluated. Costs of injury and illness are calculated and performance is measured; those that do well are rewarded, those that do not are penalized. Safety is an integral part of contracts and subcontracts. Everybody—managers, supervisors and workers—receives general, site-specific and site-relevant training and re-training. Inexperienced workers receive on-the-job training from experienced workers. In projects where such measures are implemented, injury rates are significantly lower than on otherwise comparable sites.
Preventing Accidents and Injuries
Entities in the industry with lower injury rates share several common characteristics: they have a clearly defined policy statement that applies throughout the organization, from top management to the project site. This policy statement refers to a specific code of practice that describes, in detail, the hazards and their control for the pertinent occupations and tasks at a site. Responsibilities are clearly assigned and standards of performance are stated. Failures to meet these standards are investigated and penalties imposed as appropriate. Meeting or exceeding standards is rewarded. An accounting system is used that shows the costs of each injury or accident and the benefits of injury prevention. Employees or their representatives are involved in establishing and administering a programme of injury prevention. Involvement often occurs in the formation of a joint labour or worker management committee. Physical examinations are performed to determine workers’ fitness for duty and job assignment. These exams are provided when first employed and when returning from a disability or other layoff.
Hazards are identified, analysed and controlled following the classes of hazards discussed in other articles in this chapter. The entire work site is inspected on a regular basis and results are recorded. Equipment is inspected to ensure its safe operation (e.g., brakes on vehicles, alarms, guards and so on). Injury hazards include those associated with the most common types of lost-time injuries: falls from heights or at the same level, lifting or other forms of manual materials handling, risk of electrocution, risk of injury associated with either highway or off-road vehicles, trench cave-ins and others. Health hazards would include airborne particles (such as silica, asbestos, synthetic vitreous fibres, diesel particulates), gases and vapours (such as carbon monoxide, solvent vapour, engine exhaust), physical hazards (such as noise, heat, hyperbaric pressure) and others, such as stress.
Preparations are made for emergency situations and emergency drills are conducted as needed. Preparations would include assignment of responsibilities, provision of first aid and immediate medical attention at the site, communication at the site and with others off the site (such as ambulances, family members, home offices and labour unions), transportation, designation of health care facilities, securing and stabilizing the environment where the emergency occurred, identifying witnesses and documenting events. As needed, emergency preparedness would also cover means of escape from an uncontrolled hazard such as fire or flood.
Accidents and injuries are investigated and recorded. The purpose of reports is to identify causes that could have been controlled so that, in the future, similar occurrences can be prevented. Reports should be organized with a standardized record-keeping system to better facilitate analysis and prevention. To facilitate comparison of injury rates from one situation to another, it is useful to identify the pertinent population of workers within which an injury occurred, and their hours worked, in order to calculate an injury rate (i.e., the number of injuries per hour worked or the number of hours worked between injuries).
Workers and supervisors receive training and education in safety. This education consists of teaching general principles of safety and health, is integrated into task training, is specific for each work site and covers procedures to follow in the event of an accident or injury. Education and training for workers and supervisors is an essential part of any effort to prevent injuries and disease. Training about safe work practices and procedures have been provided in many countries by some companies and trade unions. These procedures, include lockout and tagout of electrical power sources during maintenance procedures, use of lanyards while working at heights, shoring trenches, providing safe walking surfaces and so on. It is also important to provide site-specific training, covering unique features about the job site such as means of entry and exit. Training should include instruction about dangerous substances. Performance or hands-on training, demonstrating that one knows safe practices, is much better for instilling safe behaviour than classroom instruction and written examination.
In the United States, training about certain hazardous substances is mandated by federal law. The same concern in Germany led to development of the Gefahrstoff-Informationssystem der Berufsgenossenschaften der Bauwirtschaft, or GISBAU, programme. GISBAU works with manufacturers to determine the content of all substances used on construction sites. Equally important, the programme provides the information in a form to suit the differing needs of health staff, managers and workers. The information is available through training programmes, in print and on computer terminals at work sites. GISBAU gives advice about how to substitute for some hazardous substances and tells how to safely handle others. (See the chapter Using, storing and transporting chemicals.)
Information about chemical, physical and other health hazards is available at the work site in the languages that workers use. If workers are to work intelligently on the job, they should have the information necessary to decide what to do in specific situations.
And finally, contracts between contractors and subcontractors should include safety features. Provisions could include establishing a unified safety organization at multi-employer work sites, performance requirements and rewards and penalties.
Health Risks of Underground Construction Work
Hazards
Underground construction work includes tunnelling for roads, highways and railroads and laying pipelines for sewers, hot water, steam, electrical conduits, telephone lines. Hazards in this work include hard physical labour, crystalline silica dust, cement dust, noise, vibration, diesel engine exhaust, chemical vapours, radon and oxygen-deficient atmospheres. Occasionally this work must be done in a pressurized environment. Underground workers are at risk for serious and often fatal injuries. Some hazards are the same as those of construction on the surface, but they are amplified by working in a confined environment. Other hazards are unique to underground work. These include being struck by specialized machinery or being electrocuted, being buried by roof falls or cave-ins and being asphyxiated or injured by fires or explosions. Tunnelling operations may encounter unexpected impoundments of water, resulting in floods and drowning.
The construction of tunnels requires a great deal of physical effort. Energy expenditure during manual work is usually from 200 to 350 W, with a great part of static load of the muscles. Heart rate during work with compressed-air drills and pneumatic hammers reaches 150 to 160 per minute. Work is often done in unfavourable cold and humid microclimatic conditions, sometimes in cumbersome work postures. It is usually combined with exposure to other risk factors which depend on the local geological conditions and on the type of technology used. This heavy workload can be an important contribution to heat stress.
The need for heavy manual labour can be reduced by mechanization. But mechanization brings its own hazards. Large and powerful mobile machines in a confined environment introduce risks of serious injury to persons working nearby, who may be struck or crushed. Underground machinery also may generate dust, noise, vibration and diesel exhaust. Mechanization also results in fewer jobs, which reduces the number of persons exposed but at the expense of unemployment and all of its attendant problems.
Crystalline silica (also known as free silica and quartz) occurs naturally in many different types of rock. Sandstone is practically pure silica; granite may contain 75%; shale, 30%; and slate, 10%. Limestone, marble and salt are, for practical purposes, completely free of silica. Considering that silica is ubiquitous in the earth’s crust, dust samples should be taken and analysed at least at the start of an underground job and whenever the type of rock changes as work progresses through it.
Respirable silica dust is generated whenever silica-bearing rock is crushed, drilled, ground or otherwise pulverized. The main sources of airborne silica dust are compressed-air drills and pneumatic hammers. Work with these tools most often occurs in the fore part of the tunnel and, therefore, workers in these areas are the most heavily exposed. Dust suppression technology should be applied in all instances.
Blasting generates not only flying debris, but also dust and nitrogen oxides. To prevent excessive exposure, the customary procedure is to prevent re-entry to the affected area until the dust and gases have cleared. A common procedure is to blast at the end of the last work shift of the day and to clear out debris during the next shift.
Cement dust is generated when cement is mixed. This dust is a respiratory and mucous membrane irritant in high concentrations, but chronic effects have not been observed. When it settles on skin and mixes with sweat, however, cement dust can cause dermatoses. When wet concrete is sprayed in place, it too can cause dermatoses.
Noise can be significant in underground construction work. Principal sources include pneumatic drills and hammers, diesel engines and fans. Since the underground work environment is confined, there is also considerable reverberant noise. Peak noise levels can exceed 115 dBA, with time-weighted average noise exposure equivalent to 105 dBA. Noise-reducing technology is available for most equipment and should be applied.
Underground construction workers can also be exposed to whole-body vibration from mobile machinery and to hand-arm vibration from pneumatic drills and hammers. The levels of acceleration transmitted to the hands from pneumatic tools can reach about 150 dB (comparable to 10 m/s2). Harmful effects of hand-arm vibration can be aggravated by a cold and damp working environment.
If soil is highly saturated with water or if construction is conducted under water, the work environment may have to be pressurized to keep water out. For underwater work, caissons are used. When workers in such a hyperbaric environment make too rapid a transition to normal air pressure, they risk decompression sickness and related disorders. Since the absorption of most toxic gases and vapours depends on their partial pressure, more may be absorbed at higher pressure. Ten ppm of carbon monoxide (CO) at 2 atmospheres of pressure, for example, will have the effect of 20 ppm CO at 1 atmosphere.
Chemicals are used in underground construction in a variety of ways. For example, insufficiently coherent layers of rock may be stabilized with an infusion of urea formaldehyde resin, polyurethane foam or mixtures of sodium water glass with formamide or with ethyl and butyl acetate. Consequently, vapours of formaldehyde, ammonia, ethyl or butyl alcohol or di-isocyanates may be found in the tunnel atmosphere during application. Following application, these contaminants may escape into the tunnel from the surrounding walls, and it may therefore be difficult to fully control their concentrations, even with intensive mechanical ventilation.
Radon occurs naturally in some rock and may leak into the work environment, where it will decay into other radioactive isotopes. Some of these are alpha emitters that may be inhaled and increase the risk of lung cancer.
Tunnels constructed in inhabited areas can also be contaminated with substances from surrounding pipes. Water, heating and cooking gas, fuel oil, petrol and so on may leak into a tunnel or, if pipes carrying these substances are broken during excavation, they may escape into the work environment.
The construction of vertical shafts using mining technology poses similar health problems to those of tunnelling. In terrain where organic substances are present, products of microbiological decomposition may be expected.
Maintenance work in tunnels used for traffic differs from similar work on the surface mainly in the difficulty of installing safety and control equipment, for example, ventilation for electric arc welding; this may influence the quality of safety measures. Work in tunnels in which pipelines for hot water or steam are present is associated with great heat load, demanding a special regime of work and breaks.
Oxygen deficiency may occur in tunnels either because oxygen is displaced by other gases or because it is consumed by microbes or by the oxidation of pyrites. Microbes may also release methane or ethane, which not only displace oxygen but, in sufficient concentration, may create the risk of explosion. Carbon dioxide (commonly called blackdamp in Europe) is also generated by microbial contamination. The atmospheres in spaces which have been closed for a long time may contain mostly nitrogen, practically no oxygen and 5 to 15% carbon dioxide.
Blackdamp penetrates into the shaft from the surrounding terrain due to changes in the atmospheric pressure. The composition of the air in the shaft may change very quickly—it may be normal in the morning, but be deficient in oxygen by the afternoon.
Prevention
Prevention of exposure to dust should in the first place be implemented by technical means, such as wet drilling (and/or drilling with LEV), wetting of the material before it is pulled down and loaded to the transport, LEV of mining machines and mechanical ventilation of tunnels. Technical control measures may not be sufficient to lower the concentration of respirable dust to an acceptable level in some technological operations (e.g., during drilling and sometimes also in the case of wet drilling), and therefore it may be necessary to supplement the protection of the workers engaged in such operations by the use of respirators.
The efficiency of technical control measures must be checked by monitoring the concentration of airborne dust. In the case of fibrogenic dust, it is necessary to arrange the programme of monitoring in such a way that it allows the registration of the exposure of individual workers. The individual exposure data, in connection with data about each worker’s health, are necessary for the assessment of the risk of pneumoconiosis in particular work conditions, as well as for the assessment of the efficiency of control measures in the long-run. Last but not least, the individual registration of exposure is necessary for evaluating the ability of individual workers to continue in their jobs.
Due to the nature of underground work, protection against noise depends mostly on the personal protection of hearing. Effective protection against vibrations, on the other hand, can be achieved only by eliminating or decreasing the vibration by mechanization of risky operations. PPE is not effective. Similarly, the risk of diseases due to physical overload of the upper extremities can be lowered only by mechanization.
Exposure to chemical substances can be influenced by the selection of appropriate technology (e.g., the use of formaldehyde resins and formamide should be eliminated), by good maintenance (e.g., of diesel engines) and by adequate ventilation. Organization and work regime precautions are sometimes very effective, especially in the case of the prevention of dermatoses.
Work in underground spaces in which the composition of the air is not known demands strict adherence to safety rules. Entering such spaces without isolating breathing apparatuses must not be allowed. The work should be done only by a group of at least three people—one worker in the underground space, with breathing apparatus and safety harness, the others outside with a rope to secure the inside worker. In case of accident it is necessary to act quickly. Many lives have been lost in efforts to save the victim of an accident when the safety of the rescuer was disregarded.
Pre-placement, periodic and post-employment preventive medical examinations are a necessary part of the health and safety precautions for workers in tunnels. The frequency of periodic examinations and the type and scope of special examinations (x ray, lung functions, audiometry and so on) should be individually determined for each workplace and for each job according to the working conditions.
Prior to groundbreaking for underground work, the site should be inspected and soil samples should be taken in order to plan the excavation. Once work is underway, the work site should be inspected daily to prevent roof falls or cave-ins. The workplace of solitary workers should be inspected at least twice each shift. Fire suppression equipment should be strategically placed throughout the underground work site.
Preventive Health Services in Construction
The construction industry forms 5 to 15% of the national economy of most countries and is usually one of the three industries having the highest rate of work-related injury risks. The following chronic occupational health risks are pervasive (Commission of the European Communities 1993):
- Musculoskeletal disorders, occupational hearing loss, dermatitis and lung disorders are the most common occupational diseases.
- An increased risk of respiratory tract carcinomas and mesothelioma caused by asbestos exposure has been observed in all countries where occupational mortality and morbidity statistics are available.
- Disorders resulting from improper nutrition, smoking or use of alcohol and drugs are associated especially with migrant workers, a substantial portion of construction employment in many countries.
Preventive health services for construction workers should be planned with these risks as priorities.
Types of Occupational Health Services
Occupational health services for construction workers consist of three main models:
- specialized services for construction workers
- occupational health care for construction workers rendered by providers of broad-based occupational health services
- health services provided voluntarily by the employer.
Specialized services are the most effective but also the most expensive in terms of direct costs. Experiences from Sweden indicate that the lowest injury rates on construction sites worldwide and a very low risk for occupational diseases among construction workers are associated with extensive preventive work through specialized service systems. In the Swedish model, called Bygghälsan, technical and medical prevention have been combined. Bygghälsan operates through regional centres and mobile units. During the severe economic recession of the late 1980s, however, Bygghälsan severely cut back its health service activities.
In countries that have occupational health legislation, construction companies usually buy the needed health services from companies serving general industries. In such cases, the training of occupational health personnel is important. Without special knowledge of the circumstances surrounding construction, medical personnel cannot provide effective preventive occupational health programmes for construction companies.
Some large multinational companies have well-developed occupational safety and health programmes that are part of the culture of the enterprise. The cost-benefit calculations have proved these activities economically profitable. Nowadays, occupational safety programmes are included in quality management of most international companies.
Mobile health clinics
Because construction sites are often situated far from any established providers of health services, mobile health service units may be necessary. Practically all countries that have specialized occupational health services for construction workers use mobile units for delivering the services. The mobile unit’s advantage is the saving of work time by bringing the services to worksites. Mobile health centres are contained in a specially equipped bus or trailer and are especially suitable for all types of screening procedures, such as periodic health examinations. Mobile services should be careful to arrange in advance for collaboration with local providers of health services in order to secure follow-up evaluation and treatment for workers whose test results suggest a health problem.
Standard equipment for a mobile unit includes a basic laboratory with a spirometer and an audiometer, an interview room and x-ray equipment, when needed. It is best to design module units as multipurpose spaces so they can be used for different types of projects. The Finnish experience indicates that mobile units are also suitable for epidemiological studies, which can be incorporated into occupational health programmes, if properly planned in advance.
Contents of preventive occupational health services
Identification of risk at construction sites should guide medical activity, although this is secondary to prevention through proper design, engineering and work organization. Risk identification requires a multidisciplinary approach; this requires close collaboration between the occupational health personnel and the enterprise. A systematic workplace survey of risks using standardized checklists is one option.
Preplacement and periodic health examinations are usually conducted according to requirements set by legislation or guidance provided by authorities. The examination’s content depends on the exposure history of each worker. Short work contracts and frequent turnover of the construction workforce can result in “missed” or “inappropriate” health examinations, a failure to follow up on findings or unwarranted duplication of health examinations. Therefore, regular standard periodic examinations are recommended for all workers. A standard health examination should contain: an exposure history; symptom and illness histories with special emphasis on musculoskeletal and allergic diseases; a basic physical examination; and audiometry, vision, spirometry and blood pressure tests. The examinations should also provide health education and information on how to avoid occupational risks known to be common.
Surveillance and Prevention of Key Construction-related Problems
Musculoskeletal disorders and their prevention
Musculoskeletal disorders have multiple origins. Lifestyle, hereditary susceptibility and ageing, combined with improper physical strain and minor injuries, are commonly accepted risk factors for musculoskeletal disorders. The types of musculoskeletal problems have different exposure patterns in different construction professions.
There is no reliable test to predict an individual’s risk for acquiring a musculoskeletal disorder. Medical prevention of musculoskeletal disorders is based on guidance in ergonomic matters and lifestyles. Preplacement and periodic examinations can be used for this purpose. Non-specific strength testing and routine x rays of the skeletal system have no specific value for prevention. Instead, early detection of symptoms and a detailed work history of musculoskeletal symptoms can be used as a basis for medical counselling. A programme that performs periodic symptom surveys to identify work factors that can be changed has been shown to be effective.
Often, workers who have been exposed to heavy physical loads or strain think the work keeps them fit. Several studies have proved that this is not the case. Therefore, it is important that, in the context of health examinations, the examinees be informed about proper ways to maintain their physical fitness. Smoking has also been associated with lumbar disk degeneration and low-back pain. Therefore, anti-smoking information and therapy should be included in the periodic health examinations, too (Workplace Hazard and Tobacco Education Project 1993).
Occupational noise-induced hearing loss
The prevalence of noise-induced hearing loss varies among construction occupations, depending on levels and duration of exposure. In 1974, less than 20% of Swedish construction workers at age 41 had normal hearing in both ears. Implementation of a comprehensive hearing conservation programme increased the proportion in that age group having normal hearing to almost 40% by the late 1980s. Statistics from British Columbia, Canada, show that construction workers generally suffer significant loss of hearing after working more than 15 years in the trades (Schneider et al. 1995). Some factors are thought to increase susceptibility to occupational hearing loss (e.g., diabetic neuropathy, hypercholesterolemia and exposure to certain ototoxic solvents). Whole-body vibration and smoking may have an additive effect.
A large-scale programme for hearing conservation is advisable for the construction industry. This type of programme requires not only collaboration at the worksite level, but also supportive legislation. Hearing conservation programmes should be specific in work contracts.
Occupational hearing loss is reversible in the first 3 or 4 years after initial exposure. Early detection of hearing loss will provide opportunities for prevention. Regular testing is recommended to detect the earliest possible changes and to motivate workers to protect themselves. At the time of testing, the exposed workers should be educated in the principles of personal protection, as well as the maintenance and proper use of protection devices.
Occupational dermatitis
Occupational dermatitis is prevented mainly by hygienic measures. The proper handling of wet cement and skin protection are effective in promoting hygiene. During health examinations, it is important to stress the importance of avoiding skin contact with wet cement.
Occupational lung diseases
Asbestosis, silicosis, occupational asthma and occupational bronchitis can be found among construction workers, depending on their past work exposures (Finnish Institute of Occupational Health 1987).
There is no medical method to prevent the development of carcinomas after someone has been sufficiently exposed to asbestos. Regular chest x rays, every third year, are the most common recommendation for medical surveillance; there is some evidence that x-ray screening improves the outcome in lung cancer (Strauss, Gleanson and Sugarbaker 1995). Spirometry and anti-smoking information are usually included in the periodic health examination. Diagnostic tests for the early diagnosis of asbestos-related malignant tumours are not available.
Malignant tumours and other lung diseases related to asbestos exposure are widely underdiagnosed. Therefore, many construction workers eligible for compensation remain without benefits. In the late 1980s and early 1990s, Finland conducted a nationwide screening of workers exposed to asbestos. The screening revealed that only one-third of the workers with asbestos-related diseases and who had access to occupational health services had been diagnosed earlier (Finnish Institute of Occupational Health 1994).
Special needs of migrant workers
Depending on the construction site, the social context, sanitary conditions and climate may present important risks to construction workers. Migrant workers often suffer from psychosocial problems. They have a higher risk of work-related injuries than native workers. Their risk of carrying infectious diseases, such as HIV/AIDS, tuberculosis, and parasitic diseases must be taken into account. Malaria and other tropical diseases are problems for workers in areas where they are endemic.
In many large construction projects, a foreign workforce is used. A preplacement medical examination should be conducted in the home country. Also, the spreading of contagious diseases must be prevented through proper vaccination programmes. In the host countries, proper vocational training, health and safety education, and housing should be organized. Migrant workers should be provided the same access to health care and social security as native workers (El Batawi 1992).
In addition to preventing construction-related ailments, the health practitioner should work to promote positive changes in lifestyle, which can improve a worker’s health overall. Avoiding alcohol and smoking are the most important and fruitful themes for health promotion for construction workers. It has been estimated that a smoker costs the employer 20 to 30% more than a non-smoking worker. Investments in anti-smoking campaigns pay not only in the short term, with lower accident risks and shorter sick leaves, but also in the long term, with lower risks of cardiovascular pulmonary diseases and cancer. In addition, tobacco smoke has harmful multiplier effects with most dusts, especially with asbestos.
Economic benefits
It is difficult to prove any direct economic benefit of occupational health services to an individual construction company, especially if the company is small. Indirect cost-benefit calculations show, however, that accident prevention and health promotion are economically beneficial. Cost-benefit calculations of investments in preventive programmes are available for companies to use internally. (For a model used extensively in Scandinavia, see Oxenburg 1991.)
Health and Safety Regulations: The Netherlands Experience
Implementation of the EC directive Minimum Regulations for Health and Safety on Temporary and Mobile Building Sites typifies the legal regulations emanating from the Netherlands and from the European Union. Their aim is to improve working conditions, to combat disability and to reduce sickness absenteeism. In the Netherlands, these regulations for the construction industry are expressed in the Arbouw Resolution, Chapter 2, Section 5.
As is often the case, the legislation seems to be following the social changes that began in 1986, when organizations of employers and employees joined to establish the Arbouw Foundation to provide services for construction companies in civil engineering and utility construction, earth works, roadbuilding and water construction and the completion sectors of the industry. Thus, the new regulations are scarcely a problem for the responsible companies already committed to implement health and safety considerations. The fact that these principles are often very difficult to put into practice, however, has led to non-observance and unfair competition and, consequently, the need for legal regulations.
Legal Regulations
The legal regulations focus on preventive measures before the construction project is started and while it is in progress. This will yield the greatest long-term benefit.
The Health and Safety Act stipulates that evaluations of risks must address not only those arising from materials, preparations, tools, equipment and so on, but also those involving special groups of workers (e.g., pregnant women, young and elderly workers and those with disabilities).
Employers are obliged to have written risk evaluations and inventories produced by certified experts, who may be employees or external contractors. The document must include recommendations for eliminating or limiting the risks and must also stipulate phases of the work when qualified specialists will be required. Some construction companies have developed their own approach to the evaluation, the General Business Investigation and Risk Inventory and Evaluation (ABRIE), which has become the prototype for the industry.
The Health and Safety Act obliges employers to offer a periodic health examination to their employees. The purpose is to identify health problems that may make certain jobs especially hazardous for some workers unless certain precautions are taken. This requirement echoes the various collective labour agreements in the construction industry which for years have required employers to provide employees with comprehensive occupational health care, including periodic medical examinations. The Arbouw Foundation has contracted with the Federation of Occupational Health and Safety Care Centres for the provision of these services. Over the years, a wealth of valuable information has been accumulated which has contributed to enhancement of the quality of the risk inventories and evaluations.
Absenteeism Policy
The Health and Safety Act also requires employers to have an absenteeism policy which includes a stipulation that experts in this field be retained to monitor and counsel disabled employees.
Joint Responsibility
Many health and safety risks can be traced to inadequacies in the building and organization choices or to poor planning of the work when setting up a project. To obviate this, the employers, employees and the government agreed in 1989 on a working conditions covenant. Among other things, it specified cooperation between clients and contractors and between contractors and subcontractors. This has resulted in a code of conduct which serves as a model for the implementation of the European directive on temporary and mobile building sites.
As part of the covenant, Arbouw formulated limits for exposure to hazardous substances and materials, along with guidelines for the application in various construction operations.
Under the leadership of Arbouw, the FNV Building Workers and Wood Workers Union, the FNV Industry Union and the Mineral Wool Association, Benelux, agreed to a contract that called for the development of glass wool and mineral wool products with less dust emission, development of the safest possible production methods for glass wool and mineral wool, formulation and promotion of working methods for the safest use of these products and performance of the research necessary to establish safe exposure limits to them. The exposure limit for respirable fibres was set at 2/cm3 although a limit of 1/cm3 was regarded as feasible. They also agreed to eliminate the use of raw and secondary materials that are health risks, using as criteria the exposure limits formulated by Arbouw. Performance under this agreement will be monitored until it expires on 1 January 1999.
Construction Process Quality
The implementation of the EC directive does not stand in isolation but is an integral part of company health and safety policies, along with quality and environmental policies. Health and safety policy is critical part of the quality policy of the companies. The laws and regulations will be enforceable only if the employers and employees of the construction industry have played a role in their development. The government has dictated the development of a model health and safety plan that is practicable and can be enforced to prevent unfair competition from companies that ignore or subvert it.
Organizational Factors Affecting Health and Safety
Diversity of Projects and Work Activities
Many people outside the construction industry are unaware of the diversity and degree of specialization of work undertaken by the industry, though they see portions of it every day. In addition to traffic delays caused by encroachments on roads and street excavations, the public is frequently exposed to buildings being erected, subdivisions being constructed and, occasionally, to the demolition of structures. What is hidden away from view, in most cases, is the large amount of specialized work done either as part of a “new” construction project or as part of the ongoing repairs maintenance associated with almost anything constructed in the past.
The list of activities is very diverse, ranging from electrical, plumbing, heating and ventilating, painting, roofing and flooring work to very specialized work such as installing or repairing overhead doors, setting heavy machinery, applying fireproofing, refrigeration work and installing or testing communications systems.
The value of construction can be partially measured by the value of building permits. Table 1 shows the value of construction in Canada in 1993.
Table 1. Value of construction projects in Canada, 1993 (based on value of building permits issued in 1993).
|
Type of project |
Value ($ Cdn) |
% of total |
|
Residential buildings (houses, apartments) |
38,432,467,000 |
40.7 |
|
Industrial buildings (factories, mining plants) |
2,594,152,000 |
2.8 |
|
Commercial buildings (offices, stores, shops etc.) |
11,146,469,000 |
11.8 |
|
Institutional buildings (schools, hospitals) |
6,205,352,000 |
6.6 |
|
Other buildings (airports, bus stations, farm buildings, etc.) |
2,936,757,000 |
3.1 |
|
Marine facilities (wharves,dredging) |
575,865,000 |
0.6 |
|
Roads and highways |
6,799,688,000 |
7.2 |
|
Water and sewage systems |
3,025,810,000 |
3.2 |
|
Dams and irrigation |
333,736,000 |
0.3 |
|
Electric power (thermal/nuclear/hydro) |
7,644,985,000 |
8.1 |
|
Railway, telephone and telegraph |
3,069,782,000 |
3.2 |
|
Gas and oil (refineries, pipelines) |
8,080,664,000 |
8.6 |
|
Other engineering construction (bridges, tunnels, etc.) |
3,565,534,000 |
3.8 |
|
Total |
94,411,261,000 |
100 |
Source: Statistics Canada 1993.
The health and safety aspects of the work depend in large measure on the nature of the project. Each type of project and each work activity presents different hazards and solutions. Often, the severity, scope or size of the problem is related to the size of the project as well.
Client-Contractor Relationships
Clients are the individuals, partnerships, corporations or public authorities for whom construction is carried out. The vast majority of construction is done under contractual arrangements between clients and contractors. A client may select a contractor based on past performance or through an agent such as an architect or engineer. In other cases, it may decide to offer the project through advertising and tendering. The methods used and the client’s own attitude to health and safety can have a profound effect on the project’s health and safety performance.
For example, if a client chooses to “pre-qualify” contractors to ensure that they meet certain criteria, then this process excludes inexperienced contractors, those who may not have had satisfactory performance and those without qualified personnel required for the project. While health and safety performance has not previously been one of the common qualifications sought or considered by clients, it is gaining in usage, primarily with large industrial clients and with government agencies that purchase construction services.
Some clients promote safety much more than others. In some cases, this is due to the risk of damage to their existing facilities when contractors are brought in to perform maintenance or to expand the client’s facilities. Petrochemical companies in particular make it clear that contractor safety performance is a key condition of the contract.
Conversely, those firms who choose to offer their project through an unqualified open bidding process to obtain the lowest price often end up with contractors that may be unqualified to perform the work or who take short cuts to save on time and materials. This can have an adverse effect on health and safety performance.
Contractor-Contractor Relationships
Many people who are not familiar with the nature of the contractual arrangements common in construction presume that one contractor performs all or at least the major part of most building construction. For example, if a new office tower, sports complex or other high-visibility project is being constructed, the general contractor usually erects signs and often company flags to indicate its presence and to create the impression that this is “its project”. Years ago, this impression may have been relatively accurate, since some general contractors actually undertook to perform substantial parts of the project with their own direct-hire forces. However, since the mid-1970s, many, if not most, general contractors have assumed more of a project management role on large projects, with the vast majority of the work contracted out to a network of subcontractors, each of which has special skills in a particular aspect of the project. (See table 2)
Table 2. Contractors/subcontractors on typical industrial/commercial/institutional projects
The influence that this network of contractors may have on health and safety becomes fairly obvious when it is compared with a fixed worksite such as a factory or a mill. At a typical fixed-industry workplace, there is only one management entity, the employer. The employer has sole responsibility for the workplace, the lines of command and communication are simple and direct, and only one corporate philosophy applies. At a construction project, there may be ten or more employer entities (representing the general contractor and the usual subcontractors), and the lines of communication and authority tend to be more complex, indirect and often confused.
The attention given to health and safety by the person or company in charge can influence the health and safety performance of others. If the general contractor has attached a high degree of importance to health and safety, this can have a positive influence on the health and safety performance of the subcontractors on the project. The converse is also true.
Additionally, the overall health and safety performance of the site can be adversely affected by the performance of one subcontractor (e.g., if one subcontractor has poor housekeeping, leaving a mess behind as his or her forces move through the project, it can create problems for all of the other subcontractors onsite).
Regulatory efforts regarding health and safety are generally more difficult to introduce and administer in these multi-employer workplaces. It may be difficult to determine which employer has responsibility for which hazards or solutions, and any administrative controls which appear to be eminently workable in a single-employer workplace may need significant modification to be workable on a multi-employer construction project. For example, information regarding hazardous materials used on a construction project must be communicated to those who work with or near the materials, and workers must be adequately trained. At a fixed workplace with only one employer, all of the material and the information accompanying it is much more readily obtained, controlled and communicated, whereas on a construction project, any of the various subcontractors may be bringing in hazardous materials of which the general contractor has no knowledge. Additionally, workers employed by one subcontractor using a certain material may have been trained, but the crew working for another subcontractor in the same area but doing something entirely different may know nothing about the material and yet could be as much at risk as those using the material directly.
Another factor which emerges regarding contractor-contractor relationships relates to the bidding process. A subcontractor who bids too low may take short-cuts that compromise health and safety. In these cases, the general contractor must ensure that subcontractors adhere to the standards, specifications and statutes pertaining to health and safety. It is not uncommon on projects where everyone has bid very low to observe continuing health and safety problems coupled with excessive passing of responsibility, until regulatory authorities step in to impose a solution.
A further problem relates to the scheduling of work and the impact this can have on health and safety. With several different subcontractors on the site at one time, competing interests may create problems. Each contractor wants to get his or her work done as quickly as possible. When two or more contractors want to occupy the same space, or when one has to perform work overhead of another, problems can occur. This is typically a much more common problem in construction than in fixed industry, where the main competing interests tend to involve only operations versus maintenance.
Employer-Employee Relationships
The several employers on a particular project may have somewhat different relationships with their employees than those common at most fixed industrial workplaces. For example, unionized workers at a manufacturing facility tend to belong to one union. When the employer needs additional workers, it interviews and hires them and the new employees join the union. Where there are former unionized workers on layoff, they are re-hired generally on a seniority basis.
In the unionized part of the construction industry, a completely different system is used. Employers form collective associations which then enter into agreements with building and construction trade unions. The majority of the non-salaried direct-hire employees in the industry work through their union. When, for example, a contractor needs five additional carpenters at a project, he or she would call the local Carpenters’ Union and place a request for five carpenters to show up for work at the project on a certain day. The union would notify the five members at the top of the employment list that they are to report to the project to work for the particular firm. Depending on the provisions of the collective agreement between the employers and the union, the contractor may be able to “name hire” or select some of these workers. If there are no union members available to fill the employment call, the employer may be able to hire temporary workers who would join the union, or the union may bring in skilled workers from other locals to help fill the demand.
In non-unionized situations, employers use different processes to obtain additional staff. Prior employment lists, local employment centres, word of mouth and advertising in local newspapers are the principal methods used.
It is not uncommon for workers to be employed by several different employers in the course of a year. The employment duration varies with the nature of the project and the amount of work to be done. This places a large administrative load on the construction contractors compared with their fixed-industry counterparts (e.g., recordkeeping for income taxes, workers’ compensation, unemployment insurance, union dues, pensions, licensing and other regulatory or contractual issues).
This situation presents some unique challenges compared to the typical fixed-industry workplace. Training and qualifications must not only be standardized but portable from one job or sector to another. These important issues affect the construction industry much more profoundly than fixed industries. Construction employers expect workers to come to the project with certain skills and capabilities. In most trades, this is accomplished by a comprehensive apprenticeship programme. If a contractor places a call for five carpenters, he or she expects to see five qualified carpenters at the project on the day they are needed. If health and safety regulations require special training, the employer needs to be able to access a pool of workers with this training, since the training may not be readily available at the time the work is scheduled to start. An example of this is the Certified Worker Programme required at larger construction projects in Ontario, Canada, which involves having joint health and safety committees. Since this training is not currently part of the apprenticeship programme, alternative training systems had to be put in place to create a pool of trained workers.
With growing emphasis on specialized training or at least confirmation of skill level, training programmes conducted in conjunction with the building and construction trades unions will likely grow in importance, number and variety.
Inter-union Relationships
The structure of organized labour mirrors the way in which contractors have specialized within the industry. On a typical construction project, five or more trades may be represented onsite at any one time. This involves many of the same problems posed by multiple employers. Not only are there competing interests to deal with, but lines of authority and communication are more complex and sometimes blurred when compared with a single-employer, single-union workplace. This influences many aspects of health and safety. For example, which worker from which union will represent all workers on the project if there is a regulatory requirement for a health and safety representative? Who gets trained in what and by whom?
In the case of rehabilitation and reinstatement of injured workers, the options for skilled construction workers are much more limited than those of their fixed-industry counterparts. For example, an injured worker at a factory may be able to return to some other job at that workplace without crossing important jurisdictional boundaries between one union and another, because there is typically only one union in the factory. In construction, each trade has fairly clearly defined jurisdiction over the types of work its members can perform. This greatly limits the options for injured workers who may not be able to perform their normal pre-injury job functions but could none the less perform some other related work at that workplace.
Occasionally, jurisdictional disputes arise over which union should perform certain types of work which have health and safety implications. Examples include scaffold erection, boom truck operation, asbestos removal and rigging. Regulations in these areas need to consider jurisdictional concerns, especially with respect to licensing and training.
The Dynamic Nature of Construction
Construction workplaces are in many respects quite different from fixed industry. Not only are they different, they tend to be constantly changing. Unlike a factory which operates at a given location day after day, with the same equipment, the same workers, the same processes and generally the same conditions, construction projects evolve and change from day to day. Walls are erected, new workers from different trades arrive, materials change, employers change as they complete their portions of the work, and most projects are affected to some degree just by the changes in the weather.
When one project is completed, workers and employers move on to other projects to start all over again. This indicates the dynamic nature of the industry. Some employers work in several different cities, provinces, states or even countries. Similarly, many skilled construction workers move with the work. These factors influence many aspects of health and safety, including workers’ compensation, health and safety regulations, performance measurement and training.
Summary
The construction industry is presented with some very different conditions from those in fixed industry. These conditions must be considered when control strategies are being contemplated and may help to explain why things are done differently in the construction industry. Solutions developed with the input from both construction labour and construction management, who know these conditions and how to deal effectively with them, offer the best chance for improving health and safety performance.
Integrating Prevention and Quality Management
Improving Occupational Health and Safety
Construction companies are increasingly adopting the quality management systems spelled out by the International Organization for Standardization (ISO), such as the ISO 9000 series and the subsequent regulations that have been based on it. Although no recommendations on occupational health and safety are specified in this set of standards, there are cogent reasons for including preventive measures when implementing a management system such as that required by the ISO 9000.
Occupational health and safety regulations are written and implemented and are continuously being adapted to technological progress as well as to new safety techniques and to advances in occupational medicine. All too often, however, they are not followed, either deliberately or out of ignorance. When this occurs, models for safety management, such as the ISO 9000 series, assist in integrating the structure and content of preventive measures into management. The advantages of such a comprehensive approach are obvious.
Integrated management means that occupational health and safety regulations are no longer looked at in isolation, but gain relevance from the corresponding sections of a quality management handbook, as well as in process and work instructions, thus creating a fully integrated system. This integral approach can improve the chances of greater attention to accident prevention measures in daily construction practice and, thereby, reduce the number of workplace accidents and injuries. Dissemination of a handbook that integrates occupational health and safety procedures into the processes it describes is crucial for this process.
New management methods are aimed at putting people closer to the centre of the processes. Co-workers are being more actively involved. Information, communication and cooperation are promoted across hierarchical barriers. The reduction of absences due to illness or workplace accidents enhances the implementation of the principles of quality management in construction.
With the development of new building methods and equipment, safety requirements increase steadily in number. The increasing concern with environmental protection makes the problem even more complex. Coping with the demands of modern prevention is difficult without appropriate regulations and a centrally directed articulation of the process and work instructions. Clear divisions of responsibility and effective coordination for the prevention plan should, therefore, be written into the quality management system.
Improving Competitiveness
Documentation of the existence of an occupational safety management system is increasingly required when contractors submit bids for work, and its effectiveness has become one of the criteria for awarding a contract.
The pressure of international competition could become even greater in the future. It seems prudent, therefore, to integrate preventive measures into the quality management system now, rather than waiting and being forced by increasing competitive pressure to do so later, when the pressure of time and the costs of personnel and financing will be much greater. Furthermore, a not inconsiderable benefit of an integrated prevention/quality management system is that having such a well-documented programme in place is likely to reduce the costs of coverage, not only for workers’ compensation, but also for product liability.
Company Management
Company management must be committed to the integration of occupational health and safety into the management system. Goals specifying the content and time-frame of this effort should be defined and included in the basic statement of company policy. The necessary resources should be made available and appropriate personnel assigned to accomplish the project goals. Specialized safety personnel are generally required in large and mid-sized construction companies. In smaller companies, the employer must take the responsibility for the preventive aspects of the quality management system.
A periodic company management review closes the circle. The collective experiences in utilizing the integrated prevention/ quality management system should be examined and assessed, and plans for revision and for subsequent review should be formulated by company management.
Assessing Results
Assessment of results of the occupational safety management system that has been instituted is the second step in the integration of preventive measures and quality management.
The dates, kinds, frequency, causes and costs of accidents should be compiled, analysed and shared with all those in the company with relevant responsibilities. Such an analysis enables the company to set priorities in formulating or modifying process and work instructions. It also makes clear the extent to which occupational health and safety experience affects all divisions and all processes in the construction company. For this reason, defining the interface between company processes and preventive aspects takes on great importance. During bid preparation, the resources in time and money needed for comprehensive preventive measures, such as those incurred in clearing debris, can be precisely calculated.
When purchasing construction materials, attention should be paid to the availability of substitutes for potentially dangerous materials. From the beginning of a project responsibility for occupational health and safety should be assigned for particular aspects and each phase of the construction project. The need and availability for special training in occupational health and safety as well as the relative risks of injury and disease should be compelling considerations in the adoption of particular construction processes. These conditions must be recognized early on so that appropriately qualified workers can be selected and the courses of instruction can be arranged in a timely manner.
The responsibilities and authorities of the personnel assigned to safety and how they fit into the daily work should be documented in writing and collated with the onsite task descriptions. The construction company’s occupational safety staff should appear shown in its organizational chart, which, along with a clear responsibility matrix and schematic flow-charts of processes, should appear in the quality management handbook.
An Example from Germany
In practice, there are four formal procedures and their combinations for integrating occupational health and safety into a quality management system that have been implemented in Germany:
- A quality management handbook and a separate occupational safety management handbook are developed. Each has its own procedures and work instructions. In extreme cases, this creates ineffective, insular organizational solutions, which require twice the amount of work and in practice do not accomplish the desired results.
- An additional section is inserted into the quality management handbook with the heading “Occupational health and safety”. All statements on occupational health and safety are organized in this section. This path is chosen by some construction companies. Positioning a health and safety problem in a separate section may well highlight the importance of prevention, but it entails the risk being ignored as a “fifth wheel” and serves more as an evidence of intent rather than a command for appropriate action.
- All aspects of occupational health and safety are worked directly into the quality management system. This is the most systematic implementation of the basic idea of integration. The integrated and flexible structuring of the presentation models of the German DIN EN ISO 9001-9003 permits such an inclusion.
- The Underground Construction Trade Organization (Berufs-genossenschaft) favours a modular integration. This concept is explained below.
Integration in Quality Management
Once the assessment is completed, at the latest, those responsible for the construction project should contact the quality management officers and decide on the steps for actually integrating occupational safety into the management system. Comprehensive preparatory work should facilitate setting common priorities during the work that promise the greatest preventive results.
The demands of prevention that come out of the assessment are first divided into those that can be categorized according to the processes specific to the company and those that should be considered separately since they are more widespread, more comprehensive or of such a special character that they demand separate consideration. The following question can be of assistance in this categorization: Where would the interested reader of the handbook (e.g., the “customer” or the worker) most likely look for the relevant preventive policy, the section of a chapter devoted to a process specific to the company, or in a special section on occupational health and safety? Thus, it appears, a specialized procedural instruction on transporting hazardous materials would make the most sense in almost all construction companies if it were included in section on handling, storing, packing, conserving and shipping.
Coordination and Implementation
After this formal categorization should come linguistic coordination to ensure easy readability (this means presentation in the appropriate language(s) and in terms easily understood by individuals with educational levels characteristic of the particular workforce). Finally, the final documents must be formally endorsed by the top management of the company. At this juncture, it would be useful to publicize the significance of the changed or newly-implemented procedures and work instructions in company bulletins, safety circles, memos and any other available media, and to promote their application.
General Audits
To assess the effectiveness of the instructions, appropriate questions may be prepared for inclusion into general audits. In this manner, the coherence of work processes and occupational health and safety considerations is made unmistakably clear to the worker. Experience has shown that workers may at first be surprised when an audit team on the construction site in their particular division routinely asks questions on accident prevention as a matter of course. The consequent increase in the attention paid to safety and health by the workforce confirms the value of the integration of prevention into the quality management programme.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."