- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Healthcare Workers and Infectious Diseases
International Environmental Conventions
The publicity surrounding the UN Conference on Environment and Development (UNCED), which took place in Rio de Janeiro in June 1992, confirmed the central place that global environmental concerns over issues such as global warming and loss of biological diversity have on the world political agenda. In fact, in the twenty years between the 1972 Stockholm Conference on the Human Environment and the 1992 UNCED there has been not only a major increase in awareness of the threats to the environment from human activities on both a local and global scale, but also a massive increase in the number of international legal instruments governing environmental issues. (There are large numbers of collections of environmental treaties: see, e.g., Burhenne 1974a, 1974b,1974c; Hohmann 1992; Molitor 1991. For a contemporary qualitative assessment see Sand 1992.)
It will be recalled that the two main sources of international law (as defined by the 1945 Statute of the International Court of Justice) are international conventions and international customary law (Article 38(1) of the Statute). International customary law derives from state practice repeated over time in the belief that it represents legal obligation. Although it is possible for new rules of custom to emerge relatively swiftly, the speed with which awareness of global environmental problems has reached the international political agenda has meant that customary law has tended to take second place to treaty or conventional law in the evolution of legal norms. Although certain basic principles, such as the equitable utilization of shared resources (Lac Lanoux Arbitration 1957) or the obligation not to allow activities which damage the environment of neighbouring states (Trail Smelter Arbitration 1939, 1941) can be attributed to judicial decisions derived from customary law, treaties have without doubt been the main method by which the international community has responded to the need to regulate activities which threaten the environment. Another important aspect of international environmental regulation is the development of “soft law”: non-binding instruments which lay down guidelines or desiderata for future action, or through which states commit themselves politically to meeting certain objectives. These soft law instruments sometimes develop into formal legal instruments or become linked to binding instruments as, for example, through decisions of the parties to a Convention. (On the significance of soft law in relation to international environmental law see Freestone 1994.) Many of the collections of international environmental law documents cited above include soft law instruments.
This article will give a brief overview of the main international environmental conventions. Although such a review inevitably concentrates on the main global conventions, the significant and growing web of regional and bilateral agreements should also be borne in mind. (For a systematic exposition of the whole body of international environmental law, see Kiss and Shelton 1991; Birnie and Boyle 1992. See also Churchill and Freestone 1991.)
Pre-Stockholm
Prior to the 1972 Stockholm Conference the majority of environmental conventions related to the conservation of wildlife. Of historical interest only are the very early bird protection conventions (e.g., the 1902 Convention for the Protection of Birds Useful to Agriculture; see further Lyster 1985). More significant in the longer term are the general nature conservation conventions, although the 1946 Washington Convention for the Regulation of Whaling (and its 1956 Protocol) is particularly noteworthy in this period—over time it has of course changed its focus from exploitation to conservation. A pioneering convention in conservation terms was the 1968 African Convention on Conservation of Nature and Natural Resources, Algiers, which despite its comprehensive and innovative approach to conservation made the mistake of many other conventions in not establishing an administrative structure to oversee its supervision. Also notable and considerably more successful is the 1971 Ramsar Convention on Wetlands of International Importance, especially as Waterfowl Habitat, which establishes a network of protected wetland areas in the territories of member states.
Other noteworthy developments in this period are the first global Oil Pollution Conventions. The 1954 International Convention for the Prevention of Pollution of the Sea by Oil (OILPOL) (amended 1962 and 1969) broke new ground by developing a regulatory framework for the carriage of oil by sea, but the first conventions to provide for emergency action and for compensation for oil pollution damage were developed directly in response to the world’s first major oil-tanker casualty—the wreck of the Liberian oil tanker Torrey Canyon off the coast of southwest England in 1967. The 1969 International Convention relating to Intervention on the High Seas in cases of Oil Pollution Damage authorized emergency action by coastal states outside territorial waters, and its fellows, the 1969 International Convention on Civil Liability for Oil Pollution Damage and the 1971 International Convention on the Establishment of an International Fund for Compensation for Oil Pollution Damage of Brussels, provided a basis for compensation claims against the owners and operators of oil tankers supplemented by an international compensation fund. (Note also the significant industry voluntary compensation schemes such as TOVALOP and CRISTAL; see further Abecassis and Jarashow 1985.)
From Stockholm to Rio
The years 1972 to 1992 witnessed an astonishing increase in the number and variety of international environmental law instruments. Much of this activity is directly attributable to the Stockholm Conference. Not only did the famous Conference Declaration (Declaration of the United Nations Conference on the Human Environment 1972) lay down certain principles, the majority of which were de lege ferenda (i.e., they stated what the law ought to be rather than what it was), but it also developed a 109-point Environmental Action Plan and a Resolution recommending institutional and financial implementation by the UN. The result of these recommendations was the establishment of the United Nations Environment Programme (UNEP), established by UN General Assembly Resolution (UNGA 1972) and based eventually in Nairobi. UNEP was directly responsible for the sponsoring of a number of key global environmental treaties and for the development of the important Regional Seas Programme, which has resulted in a network of some eight regional framework conventions protecting the marine environment, each with protocols developed to meet the special requirements of the region. A number of new regional programmes are still in the pipeline.
In order to provide an overview of the large number of environmental conventions developed during this period, they are divided into a number of groups: nature conservation; protection of the marine environment; and regulation of transboundary environmental impacts.
Conservation of nature and natural resources
This period saw the conclusion of a number of nature conservation treaties both at a global and regional level. At the global level, particularly noteworthy are the 1972 UNESCO Convention Concerning the Protection of the World Cultural and Natural Heritage, the 1973 Washington Convention on International Trade in Endangered Species (CITES) and the 1979 Bonn Convention on the Conservation of Migratory Species of Wild Animals. At a regional level the large number of treaties include the 1974 Nordic Convention on the Protection of the Environment, the 1976 Convention on Conservation of Nature in the South Pacific (Apia Convention, in Burhenne 1974a) and the 1979 Berne Convention on the Conservation of European Wildlife and Natural Habitats (European Treaty Series). Note also the 1979 EC Directive 79/409 on the conservation of wild birds (OJ 1979), now amended and supplemented by Directive 92/43 on the conservation of natural habitats and of wild flora and fauna (OJ 1992), the 1979 Convention for the Conservation and Management of the Vicuna and the 1985 ASEAN Agreement on the Conservation of Nature and Natural Resources (reproduced in Kiss and Shelton 1991). (Also of note are the treaties relating to the Antarctic—an area of global commons outside the jurisdiction of any state: the 1980 Canberra Convention on the Conservation of Antarctic Marine Living Resources, the 1988 Wellington Convention on the Regulation of Antarctic Mineral Resource Activities and the 1991 Protocol to the Antarctic Treaty on Environmental Protection, signed in Madrid.)
Protection of the marine environment
In 1973 the negotiations began of the Third UN Conference on the Law of the Sea (UNCLOS III). The nine years of UNCLOS negotiations culminated in the 1982 Montego Bay Convention on the Law of the Sea (LOSC), which included in its Part XII a general framework for the regulation of marine environmental issues including vessel and land-based sources of pollution and dumping, as well as laying down certain general duties regarding protection of the marine environment.
At a more detailed level, the International Maritime Organization (IMO) was responsible for the development of two major global conventions: the 1972 London Convention on the Prevention of Marine Pollution by Dumping of Wastes and Other Matter and the 1973 International Convention for the Prevention of Pollution from Ships, as amended in 1978 (MARPOL 1973/78), and a third relating to oil spills entitled the International Convention on Oil Pollution Preparedness, Response and Cooperation in 1990, establishes a global legal framework for collaboration and assistance in response to major oil spills. (Other Maritime Conventions which are not primarily environmental but are of relevance include the 1972 Convention on the International Regulations for Preventing Collisions at Sea (COLREG); the 1974 International Convention for the Safety of Life at Sea (SOLAS); the 1976 ILO Merchant Shipping (Minimum Standards) Convention (No. 147) and the 1978 Convention on Standards of Training, Certification and Watch Keeping for Sea Farers).
The 1972 London Convention adopted what has now become a common approach by listing substances (Annex I) which could not be dumped in the ocean; Annex II listed substances which could be dumped only with a permit. The regulatory structure, which requires signatory states to enforce these obligations against any vessels loading in their ports or their flag vessels anywhere in the world, has progressively tightened its regime to the extent that parties have now effectively ended the ocean dumping of industrial waste. The 1973/78 MARPOL Convention replaces the 1954 OILPOL Convention (above) and provides the main regulatory regime for pollution from vessels of all sorts, including oil tankers. MARPOL requires flag states to impose controls on the “operational discharges” of all controlled substances. The MARPOL regime was amended in 1978 so that it would progressively extend its regime over different forms of vessel sources pollution contained in the five Annexes. All the Annexes are now in force covering oil (Annex I), noxious liquid substances (Annex II), packaged waste (Annex III), sewage (Annex IV) and garbage (Annex V). Stricter standards are enforced within Special Areas agreed by the Parties.
At a regional level, the UNEP Regional Seas Programme provides a wide, although not comprehensive, network of marine protection treaties covering: the Mediterranean (Convention for the Protection of the Mediterranean Sea against Pollution, Barcelona, 16 February, 1976; protocols in 1976 (2), 1980 and 1982); Gulf (Kuwait Regional Convention for Co-operation on the Protection of the Marine Environment from Pollution, Kuwait, 24 April 1978; protocols in 1978, 1989 and 1990); West Africa (Convention for Co-operation in the Protection and Development of the Marine and Coastal Environment of the West and Central African Region (Abidjan, 23 March 1981), with a 1981 protocol); South East Pacific (Convention for the Protection of the Marine Environment and Coastal Areas of the South-East Pacific (Lima, 12 November 1981); protocols in 1981, 1983 (2) and 1989); Red Sea (Regional Convention for the Conservation of the Red Sea and Gulf of Aden Environment (Jeddah, 14 February 1982); protocol in 1982); Caribbean (Convention for the Protection and Development of the Marine Environment of the Wider Caribbean Region, (Cartagena des Indias, 24 March 1983); protocols in 1983 and 1990); East Africa (Convention for the Protection, Management and Development of the Marine and Coastal Environment of the East African Region (Nairobi, 21 June 1985); 2 protocols in 1985); and the South Pacific (Convention for the Protection of the Natural Resources and Environment of the South Pacific Region, (Noumea, 24 November 1986); 2 protocols in 1986)—with another six or so in various stages of planning. (For texts of all the above Conventions and their protocols, as well as details of developing programmes, see Sand 1987.) These treaties are supplemented by protocols covering a wide range of issues including regulation of land-based sources of pollution, ocean dumping, pollution from (and decommissioning of) off-shore oil rigs, specially protected areas and protection of wildlife.
Other regional regimes have been developed outside the UNEP framework, notably in the North East Atlantic, where a highly comprehensive network of regional instruments covers regulation of ocean dumping (1972 Oslo Convention for the Prevention of Marine Pollution by Dumping from Ships and Aircraft; protocols in 1983 and 1989), land-based sources of pollution (1974 Paris Convention for the Prevention of Marine Pollution from Land Based Sources; protocol in 1986), oil pollution monitoring and cooperation (1983 Bonn Agreement for Co-operation in Dealing with Pollution of the North Sea by Oil and other Harmful Substances: Amending Decision 1989), inspection of vessels for safety and protection of the marine environment (1982 Paris Memorandum of Understanding on Port State Control in Implementing Agreements on Maritime Safety and Protection of the Marine Environment, as well as nature conservation and fisheries. (See generally Freestone and IJlstra 1991. Note also the new 1992 Paris Convention for the Protection of the Marine Environment of the North-East Atlantic, which will replace the Oslo and Paris Conventions; text and analysis in Hey, IJlstra and Nollkaemper 1993.) In the Baltic the 1974 Helsinki Convention on the Protection of the Marine Environment of the Baltic Sea Area has recently been revised (for text and analysis of 1992 Convention see Ehlers 1993)), and a new Convention developed for the Black Sea Region (1992 Bucharest Convention on the Protection of the Black Sea; see also 1993 Odessa Ministerial Declaration on the Protection of the Black Sea.)
Transboundary impacts
Principle 21 of the Stockholm Declaration provided that States had “the responsibility to ensure that activities under their jurisdiction and control do not cause damage to the environment of other States or of areas beyond national jurisdiction”. Although this principle is now widely regarded as having become part of customary international law, the principle grosso modo requires considerable fine tuning to provide the basis for regulation of such activities. Addressing these issues, and largely in response to well publicized crises, international conventions have been developed to address issues such as long-range transboundary air pollution, protection of the ozone layer, notification and cooperation in response to nuclear accidents, transboundary movement of hazardous waste and global climate change.
Long-range transboundary air pollution
Long-range air pollution in Europe was first addressed by the 1979 Geneva Convention (Convention on Long-Range Transboundary Air Pollution). This, however, was a framework convention whose modestly expressed aims were “to limit and, as far as possible, gradually to reduce and prevent air pollution including long range transboundary pollution”. Substantive progress in regulating emissions of specific substances was made only with the development of the protocols, of which there are now four: the 1984 Geneva Protocol (Geneva Protocol on Long-term Financing of the Co-operative Programme for Monitoring and Evaluation of the Long-Range Transmission of Air Pollution in Europe) established a network of air quality monitoring stations; the 1985 Helsinki Protocol (on the Reduction of Sulphur Emissions) aimed to reduce sulphur emissions by 30% by 1993; the 1988 Sofia Protocol (Concerning the Control of Emissions of Nitrogen Oxides or their Transboundary Fluxes), now replaced by the Second Sulphur Protocol, Oslo, 1994, provided for a freeze on national emissions of nitrogen oxides at 1987 levels by 1994; and the 1991 Geneva Protocol (Concerning the Control of Emissions of Volatile Organic Compounds or their Transboundary Fluxes) provided a range of options for emission abatement of volatile organic compounds and fluxes.
Transboundary implications of nuclear accidents
World attention had been brought to the transboundary implications of nuclear accidents after the 1986 Chernobyl accident, but even prior to that, previous conventions had addressed a number of the issues relating to the risks from nuclear devices, including the 1961 Convention on Third Party Liability in the Field of Nuclear Energy (1960), and the Vienna Convention on Civil Liability for Nuclear Damage (1963). Note also the 1963 Treaty Banning Nuclear Weapon Tests in the Atmosphere, in Outer Space and Under Water. The 1980 Vienna Convention on the Physical Protection of Nuclear Material had attempted to establish standards for the protection of nuclear material from a number of threats, including terrorism. In the wake of Chernobyl two further conventions were agreed upon in 1986, on early notification of accidents (Vienna Convention on the Early Notification of a Nuclear Accident) and international cooperation in the event of such accidents (Vienna Convention on Assistance in the Case of a Nuclear Accident or Radiological Emergency).
Protection of the ozone layer
The 1985 Vienna Convention for the Protection of the Ozone Layer imposes general obligations on each party “in accordance with the means at their disposal and their capabilities” to:
a) cooperate by means of systematic observation, research and information exchange in order to better understand and assess the effects of human activities on the ozone layer and the effects on human health and the environment from modification of the ozone layer; (b) adopt appropriate legislative or administrative measures and cooperate in harmonizing appropriate policies to control, limit, reduce or prevent human activities under their jurisdiction or control should it be found that these activities have or are likely to have adverse effects resulting from modification or likely modification of the ozone layer; (c) cooperate in the formulation of agreed measures, procedures and standards for the implementation of the Convention, with a view to the adoption of protocols and annexes; (d) cooperate with competent international bodies to implement effectively the Convention and protocols to which they are party.
The Vienna Convention was supplemented by the 1987 Montreal Protocol on Substances that Deplete the Ozone Layer, itself adjusted and amended by the London Meeting of 1990 and most recently by the Copenhagen Meeting of November 1992. Article 2 of the Protocol requires parties to impose controls on ozone-depleting chemicals, namely CFCs, halons, other fully halogenated CFCs, carbon tetrachloride and 1,1,1-tri-chloroethane (methyl chloroform).
Article 5 provides an exemption from emissions restrictions for certain developing countries, “to meet (Their) basic domestic needs” for up to ten years, subject to certain provisos set out in Article 5(2) (3). The Protocol also provides for technical and financial cooperation for developing country parties claiming exemption under Article 5. A Multilateral Fund was agreed upon to assist such parties to research and meet their obligations (Article 10). In Copenhagen in November 1992, in the light of the 1991 Scientific Assessment of Ozone Depletion, which found that there was new evidence of ozone decreases in both hemispheres at middle and high latitudes, a number of new measures were agreed upon, subject of course to the general regime outlined above; delays under Article 5 are still possible for developing states. All parties were required to cease using halons by 1994, and CFCs, HBFCs, carbon tetrachloride and methyl chloroform by 1996. The use of HCFCs should be frozen by 1996, reduced 90% by 2015 and eliminated by 2030. Methyl bromide, still used as a fruit and grain preservative, was subjected to voluntary controls. Contracting parties agreed to “make every effort” to freeze its use by 1995 at 1991 levels. The overall aim was to stabilize atmospheric chlorine loading by the year 2000 and then reduce it to below critical levels by about 2060.
Transboundary movement of hazardous wastes
Following a series of notorious incidents in which shipments of hazardous waste from developed countries were found in uncontrolled and hazardous conditions in developing countries, the transboundary movement of hazardous wastes was made the subject of international regulation by the 1989 Basel Convention on the Control of Transboundary Movement of Hazardous Wastes and their Disposal (see also Kummer 1992). This Convention is premised upon the principle of prior informed consent on a state to state basis before the movement of such waste can take place. The Organization of African Unity has however gone further than this with its 1991 Bamako Convention on the Ban of the Import into Africa and the Control of Transboundary Movement and Management of Hazardous Wastes within Africa, which seeks to ban entirely the import of hazardous waste into Africa.
Environmental impact assessment (EIA) in a transboundary context
The 1991 Espoo Convention on Environmental Impact Assessment in a Transboundary Context sets out a framework for neighbourly relations. It extends the EIA concept, developed to date exclusively in the context of national planning laws and procedures, to the transboundary impacts of development projects and related procedures and decisions.
1992 and Post-Rio Conventions
The Rio UNCED prompted, or coincided with, a large number of new global and regional environment conventions, as well as a major declaration of principles for the future in the Rio Declaration on Environment and Development. In addition to the two conventions concluded at Rio—the Framework Convention on Climate Change and the Convention on Biological Diver-sity—new environmental conventions signed in 1992 included those regulating the use of international watercourses as well as the transboundary effects of industrial accidents. At a regional level 1992 saw the Helsinki Convention on the Protection and Use of the Baltic Sea Area (text and analysis in Ehlers 1993) and the Bucharest Convention on the Protection of the Black Sea against Pollution. Note also the 1993 Ministerial Declaration on the Protection of the Black Sea, which advocates a precautionary and holistic approach, and the Paris Convention for the Protection of the Marine Environment of the North East Atlantic (text and analysis in Hey, IJlstra and Nollkaemper 1993).
The United Nations Framework Convention on Climate Change (UNFCCC)
The UNFCCC, signed at Rio de Janeiro in June 1992 by some 155 states, is loosely modelled on the 1985 Vienna Convention. As its name suggests, it provides a framework within which more detailed obligations will be negotiated by the means of detailed protocols. The basic objective of the Convention is to achieve
stabilization of greenhouse gas concentrations in the atmosphere at a level that will prevent dangerous anthropogenic interference with the climate system ...hin a time-frame sufficient to allow ecosystems to adapt naturally to climate change, to ensure food production is not threatened and to enable economic development to proceed in a sustainable manner. (Article 2)
Two primary duties are imposed on all Parties by Article 4: (a) to develop, periodically update, publish and make available a national inventory of anthropogenic emissions by sources and removals by sinks of all greenhouse gases using comparable (and yet to be agreed upon) methodologies; and (b) to formulate, implement, publish and regularly update national and regional programmes of measures to mitigate climate change by addressing anthropogenic emissions by sources and removals by sinks of all greenhouse gases and measures to facilitate adequate adaptation to climate change. In addition developed country parties agree to a number of general obligations which will be made specific by more detailed protocols.
For example, to undertake to promote, and cooperate in, the development of technologies; to control, prevent or reduce anthropogenic emissions of greenhouse gases; to promote sustainable development and the conservation and enhancement of sinks and reservoirs including biomass, forests, oceans and other terrestrial, coastal and marine ecosystems; to cooperate in adaptation to impacts of climate change, by elaboration of plans for integrated coastal zone management, water resources and agriculture and for protection and rehabilitation of areas affected by, inter alia, floods; to promote and cooperate in the exchange of scientific, technological, socioeconomic and legal information relevant to climate, climate change and response strategies; and to promote and cooperate in relevant education, training and public awareness.
The Biological Diversity Convention
The objectives of the Convention on Biological Diversity, also approved at the 1992 UNCED in Rio de Janeiro, are to conserve biological diversity, the sustainable use of its components and the fair and equitable sharing of the benefits arising out of the utilization of genetic resources (Article 1) (for a useful critique, see Boyle 1993). Like the UNFCCC this convention too will be supplemented by protocols, but it establishes general obligations regarding conservation and sustainable use of natural resources, for identification and monitoring of biological diversity, for in situ and ex situ conservation, research and training as well as public education and awareness and EIA of activities likely to affect biodiversity. There are also general provisions relating to access to genetic resources and access to, and transfer of, relevant technology, including biotechnology, as well as international exchange of information and cooperation.
Regulation of the use of international watercourses
The 1992 Helsinki Convention on the Protection and Use of Transboundary Watercourses and International Lakes seeks to establish cooperative frameworks for joint monitoring and assessment, common research and development and information exchange between riparian states. It imposes basic duties on such states to prevent control and reduce transboundary impacts on such shared resources, particularly regarding water pollution, through proper management techniques, including EIA and contingency planning as well as through the adoption of low- or non-waste technology and reduction of pollution from point and diffuse sources.
The transboundary effects of industrial accidents
The Convention on the Transboundary Effects of Industrial Accidents, also signed in Helsinki in March 1992, covers the prevention of, preparedness for and response to industrial accidents capable of having a transboundary effect. The primary obligations are to cooperate and exchange information with other parties. The detailed system of thirteen annexes establishes systems to identify hazardous activities with transboundary implications, for the development of EIA with a transboundary dimension (in accordance with the 1991 Espoo Convention, above) for decisions on siting of potentially hazardous activities. It also provides for emergency preparedness and for access to information for the public as well as the other parties.
Conclusion
As this brief review should have demonstrated, over the last two decades there has been a major change in the attitude of the world community to environmental conservation and management. Part of that change has been a substantial increase in the numbers and the scope of international instruments addressing environmental concerns. The sheer number of instruments has been matched by new principles and institutions. The polluter pays principle, the precautionary principle (Churchill and Freestone 1991; Freestone and Hey 1996) and concern for the rights of future generations (Kiss, in Freestone and Hey 1996) are all reflected in the international conventions reviewed above. The role of the UN Environment Programme and the treaty secretariats established to service and monitor the burgeoning number of treaty regimes lead commentators to suggest that international environmental law, like, for example, the international law of human rights, has emerged as a new discrete branch of international law (Freestone 1994). UNCED played an important role in this, it has established a major agenda—much of which remains unfinished. Detailed protocols are still needed to add substance to the framework of the Climate Change Convention and, arguably, also to the Convention on Biological Diversity. Concern with the environmental impact of fishing in high seas areas led to the conclusion of the UN Agreement on Straddling Fish Stocks and Highly Migratory Fish Stocks was in 1995. Also held in 1995 was another UN Conference on Land Based Sources of Marine Pollution—now agreed to be the cause of more than 70% of all pollution of the oceans. The environmental dimensions of world trade as well as deforestation and desertification are also issues to be addressed for the future at a global level while progress continues to enhance our awareness of impacts of human activities on world eco-systems. The challenge for this emerging international environmental law is not simply to respond with an increase in the numbers of environmental instruments, but also to enhance their impact and effectiveness.
Laws and Regulations
The relationship between human health and the human environment has been recognized from time immemorial. This tenet of medicine can be traced back to Hippocrates, who taught his pupils to “attend to the airs, waters, and places” if they sought to understand the sources of health and diseases in their patients (Lloyd 1983).
This ancient view of the link between human health and the environment has persisted. The degree of a society’s acceptance of this link has been influenced by three factors: development of a scientific understanding of the human body; increased capacity to cure individual illnesses; and the evolution of parallel scientific, religious and cultural concepts.
Environmental factors as a cause of health or diseases of entire classes of people were given increased attention during the Industrial Revolution. The trend has continued to this day, assisted by the development of the environmental sciences and of techniques for determining causality and assessing risks.
It was in the workplace that causal links between health and the environment were first clearly established. It was also in the workplace that the consequences of the increase in the amount and variety of contaminants resulting from the diversification of industrial processes were first felt. Yet these contaminants cannot be confined to the occupational environment. Once released, their pathway may become difficult to follow or trace, but it inevitably ends in nature: environmental toxins are present in the soil, water and air of even the most remote environments. Human health, in turn, is affected by the pollution of the natural environment, whether of local, national or transboundary origin. Along with other types of environmental degradation, which cause worldwide depletion of natural resources, this accords a planetary dimension to the interaction between environmental conditions and public health.
The conclusion is inescapable that the quality of the work environment and of the natural environment are inextricably linked. Lasting solutions to either of these problems can be successful only if both are tackled in tandem.
Environmental Law: A Means to an End
The formulation of policies to maintain and improve both the natural and the work environment is a prerequisite to successful environmental management. Policies, however, remain a dead letter unless they are implemented. Such implementation is only achievable through the translation of policy principles into rules of law. From this perspective, law is at the service of policy, giving it concreteness and a degree of permanency through appropriate legislation.
Legislation, in turn, is a framework structure which is useful only if implemented and enforced. Implementation and enforcement are dependent on the political and social contexts in which they take place; if they are not backed by the public, they are likely to remain inefficient.
Therefore, enactment, implementation and enforcement of environmental legislation are, to a large extent, dependent on understanding and acceptance of the rules established by those to whom these rules are addressed—hence the importance of disseminating environmental information and knowledge to the public at large, as well as to specific target groups.
The Role of Environmental Law: Prevention and Cure
The role of law in the environmental field, as in many other fields, is twofold: first, to create rules and conditions which are conducive to the control or prevention of damage to the environment or human health; and, second, to offer remedies for situations where damage has occurred in spite of these rules and conditions.
Prevention through command techniques
Land use controls
The regulation of land use is a major element of environmental law, and a prerequisite to the control and guidance of land development and the utilization of natural resources. The issue is usually whether a particular environment may be put to another use, it being understood that non-use is also a type of land use.
Land use controls allow siting human activities where they are best located (or least damaging), and also subject contemplated activities to restrictions. These two goals are usually achieved by establishing a requirement for prior authorization.
Prior authorization
Prior authorization is a generic term for any form of permission (e.g., licence, permit) which must be obtained from a regulatory authority before certain activities may be undertaken.
The first step is to determine by law those private and public sector activities which are subject to prior authorization. Several approaches are possible and are not mutually exclusive:
Controls of sources. When a category of sources of environmental harm is clearly identifiable, it is usually subject to prior authorization as such (e.g., all classes of industrial facilities and motor vehicles).
Controls of substances. When a particular substance or class of substances is identified as potentially harmful to the environment, the use or release of these substances may be made subject to prior authorization.
Media-oriented controls, and integrated pollution control. Media-oriented controls are those which are directed at protecting a specific component of the environment (air, water, soil). Such controls may lead to shifting environmental harm from one medium to another, and thus fail to reduce (or may even increase) the overall degree of environmental harm. This has led to the development of coordinated prior authorization systems, whereby all pollution from one source and all recipient media are considered before one single, all-embracing authorization is granted.
Environmental standards
Environmental standards are maximum permissible limits which may be imposed directly by a law, or indirectly as conditions to obtain an authorization. These limits may be related either to the effects or the causes of environmental harm:
- Effect-related standards are those which take the target as a baseline. They include:
- (1) biological standards, (2) exposure standards and (3) environmental quality standards.
- Cause-related standards are those which take the cause of the possible environmental harm as a baseline. They include: (1) emission standards, (2) product standards and (3) process or operating standards.
A variety of factors, including the nature of the pollutant, the recipient media and the state of the art, determine which type of standard is most appropriate. Other considerations also play an important role: standard-setting provides a means to achieve a balance between what is environmentally desirable in a particular place at a particular point in time, and the socioeconomic feasibility of achieving a specific environmental goal.
It goes without saying that the stricter the standards are, the higher production costs become. Therefore, differing standards in different locations within a state or between states play an important role in determining competitive market advantages or disadvantages, and may constitute non-tariff barriers to trade—hence the desirability of seeking harmonization at the regional or global level.
Prevention through incentives and disincentives
Controls voluntarily submitted to may be used as flanking measures or as alternatives to command techniques. They usually consist of setting recommended (rather than compulsory) values, and of providing economic incentives or disincentives to achieve them.
The purpose of an incentive (e.g., accelerated depreciation allowance, tax benefit, subsidy) is to reward and, therefore, to generate, a specific environmentally friendly conduct or activity. Thus, instead of trying to achieve a certain emission level by the stick, the carrot of economic benefit is offered.
The purpose of a disincentive (e.g., fees, such as effluent or emission charge, tax or levy) is to induce environmentally friendly conduct so as to avoid paying the fee in question.
There are also other ways of inducing adherence to recommended values, for instance, through the creation of eco-label award schemes, or providing marketing advantages where consumers are sensitized to environmental concerns.
These so-called voluntary approaches are often referred to as alternatives to “legal” controls, forgetting that incentives and disincentives also have to be established by law!
Cure through sanctions or remedies
Sanctions imposed by the regulatory agency
In cases where environmental management measures may be prescribed by the regulatory agency (e.g., through a prior authorization mechanism), legal regimes usually also provide the agency with enforcement powers. A variety of techniques are available, ranging from the imposition of monetary sanctions (e.g., per day) until compliance with the requirement, to execution of the measures required (e.g., building filters) at the cost of the addressee, and finally to closure of the facility for non-compliance with administrative requirements, etc.
Each legal system provides for ways in which these measures may be challenged by those to whom they are applied. Equally important is to provide the possibility for other interested parties (e.g., NGOs representing the public interest) to challenge the decisions of the regulatory agency. In the latter case, it is not only the action of the administration which should be eligible for challenge, but also its inaction.
Penal sanctions
Legislation prescribing a certain environmental norm or conduct usually indicates that disregarding the established rules, whether intentionally or not, constitutes an offence, and determines the type of penal sanctions which are to be applied to each case. Penal sanctions may be monetary (fines) or, in serious cases, may entail incarceration, or a combination of both. Penal sanctions for environmental offences depend upon the penal system of each country. Thus, sanctions are often imposed in reference to the main body of criminal law in a particular country (e.g., a penal code), which may also include a chapter on environmental offences. Penal sanctions can be triggered by the administration or by an aggrieved party.
The legislation of many countries has been criticized for failing to declare certain environmental misconducts as penal offences, or for providing overly mild penalties for environmental offences. It has often been observed that if the quantum of the sanctions is less than the cost of internalizing environmental management measures, the culprits are likely to deliberately prefer the risk of a penal sanction, especially if this sanction may be only a fine. This is especially true when there is an enforcement deficit—that is, when the enforcement of environmental norms is lax or lenient, as is often the case.
Liability for damages
Each legal system’s rules applying to liability for damage naturally also apply to health and environmental damage. This usually means that compensation is due either in kind or specie only when the damage proves to have been caused directly by the fault of one or more originators.
In the environmental field, the difficulties in applying these principles are numerous, and have led to the enactment of sui generis environmental liability laws in an increasing number of countries. This has made it possible to provide for liability without fault, and, therefore, to allow for compensation independently of the circumstances which caused the damage. In such cases, however, a certain monetary ceiling is usually set with a view to permitting eligibility for insurance coverage, which may also be made compulsory by law.
These special regimes also attempt to better provide redress in cases of damage to the environment per se (ecological damage as opposed to economic damage), usually requiring the restoration of the environment to the status quo ante whenever the nature of the damage permits. In such a scenario, monetary damages are in order only if restoration is impossible.
Access to remedies
Not everyone may take action to generate sanctions or obtain remedies. These may traditionally be triggered only by the administration, or a physical or legal person directly affected by a certain situation. In cases where it is the environment that is affected, this is usually insufficient, since much environmental damage is not directly linked to individual human interests. Therefore, it is important for legal systems to grant “representatives” of the public interest the right to sue the administration for failure to act or for insufficient action, or to sue individuals or enterprises for breaking the law or causing damage to the environment. There are various ways in which this can be achieved: designated non-governmental organizations may be given this right; the legal system may provide for class action or citizens’ suits, etc. The right to sue in defence of the public interest, rather than only to defend a proprietary interest, is one of the most important elements of modern environmental legislation.
Conclusion
Good environmental legislation is a prerequisite to achieve and maintain the desired levels of quality in the natural, as well as in the work environment.
What “good” environmental legislation is, might be difficult to define. Some wish to see a decline in command and control methods, and their replacement by softer incitation techniques but, in practice, there is no standard formula to decide what the ingredients of the law should be. What is important, however, is to make legislation relevant to the particular situation of the country concerned, adapting available principles, methods and techniques to the needs, capacities and legal traditions of each country.
This is all the more true at a time when large numbers of developing nations and nations with economies in transition seek to equip themselves with “good” environmental legislation, or to retrofit legislation already in place. In striving towards this goal, however, legislation which is successful in a particular legal, economic and social context, frequently that of an industrialized country, is still too often imported as a model in countries and legal systems for which it is totally inappropriate.
“Particularizing” legislation is, therefore, perhaps the most important element in achieving the goal of effective environmental legislation.
Environment and the World of Work: An Integrated Approach to Sustainable Development, Environment and the Working Environment
It should come as no surprise to occupational health and safety practitioners that if one traces back from most of our present major environmental problems—one arrives at a workplace! Likewise, the serious occupational health and safety consequences of some chemicals and substances have become an early warning system of potential environmental health consequences far beyond the workplace.
Despite the obvious inter-relationship between the working environment and the environment, many governments, employers and workers continue to respond to the causes and consequences of both working environment and environment issues in very disparate and isolated ways. (Given the importance of distinguishing between the working environment and those broader environmental perspectives represented by such adjectives as physical, general or external, this article will use the term working environment to encompass all occupational health, safety and environment issues within the workplace and the term environment to encompass those environmental issues beyond the workplace.) The goal of this article is to draw attention to the significant advantages which may arise from responding to the environment—within and outside the workplace—in a more integrated and strategic fashion. This is true not only for industrialized countries, which have made significant progress regarding both occupational safety and health and environment, but as well in transition economies and developing countries, which have a much broader and overwhelming challenge yet before them.
As this article has been specifically prepared for the Fourth Edition of the Encyclopaedia of Occupational Health and Safety it does not attempt to review the full range of occupational health and safety (OHS) issues related to the environment, many of which are reflected in other chapters of the Encyclopaedia. In fact, occupational health and safety is an integral part of every enterprise’s “environmental” performance. This is not to suggest that OHS and environmental protection are always totally compatible and mutually reinforcing; occasionally they may also be antagonistic. Nevertheless, the objective should be to find ways to protect both workers’ health and safety and the broader environment, and to avoid options which suggest that one needs to choose one or the other. The identification of environmental problems and response strategies has too often led to the creation of false dichotomies—environmental protection versus worker safety or environmental protection versus job security. While such conflicts may indeed exist in very specific and special circumstances, the majority of situations require a series of trade-offs and careful longer-term approaches for meeting both environmental and worker protection and employment objectives. This leads to a corollary thesis that worker-employer collaboration is a critical factor necessary for improved performance regarding both OHS and environment.
This perspective on environment and the world of work is especially evident if one assumes that OHS performance at the workplace should be driven by a focus on prevention rather than simply on control and remediation. The concept of prevention is fundamental to future improvements in OHS and the environment. Early in the 20th century in industrialized countries, OHS was often driven by a simplistic focus on control—the protection of workers from exposure to health and safety risks. Special emphasis was given to engineering solutions to limit accidents by improving machinery—for example, by introducing protective devices. As our knowledge of the health consequences related to the exposure of workers to certain chemicals and substances expanded, the “logical” response strategy was often first to protect the worker from exposure by improving ventilation systems or the wearing of protective devices. While important early exceptions exist, particularly in industrialized countries, it is a relatively recent phenomenon of the past few decades that so much public attention is being increasingly devoted in a number of key industrial sectors to eliminating or replacing the dangerous or toxic chemicals/substances with those which are significantly less harmful. It is interesting to note that this growing emphasis on prevention of the emission itself, or the use of specific chemicals, has grown at the same time as the public has become increasingly aware of and actively involved in environmental challenges.
This new environmental awareness has stressed both the immediate and longer-term consequences of environmental degradation for our societies and our economies. Such public interest in the environment appears to have also supported workers’ ongoing efforts to collaborate with employers to improve occupational safety and health. Nevertheless, it is blatantly clear that serious action to date regarding OHS and environment represents only a tip of the proverbial iceberg of OHS and environmental problems evident on our planet, and even more dramatically evident in developing countries and transition economies.
Environmental priorities and policies in industrialized countries have travelled a very similar path from control to prevention strategies, albeit in a much shorter time span than that of OHS. Concern for the environment in its early stages was in fact limited to a concern about “pollution”. Attention was focused primarily on emissions to air, water and soils generated by the production process. Therefore, response strategies similarly often focused on “end-of-pipe” strategies to deal with the problem of local emissions. Citing just one rather simple example, this narrow approach led to solutions such as taller chimneys, which unfortunately did not eliminate the pollution but rather dispersed it far beyond the enterprise gate and the local community. While this often satisfied the local community and the workers who lived and worked there, new environmental problems were created—long-distance and even transboundary air pollution, which in some cases leads to what has been called “acid rain”. Once the secondary effects of this end-of-pipe solution became evident, there followed considerable delay before some of the relevant stakeholders accepted that there were indeed other serious negative consequences created by the tall-chimney solution. The next innovative step in this process was to add on a sophisticated filtering system to trap the problem emissions before they left the chimney. As this example demonstrates, the focus of policy-makers was not on the prevention of the emissions but rather on various actions to control those emissions. Today, increasing efforts are being made to prevent the emissions by changing fuels and improving combustion technologies, as well as changing the production process itself through the introduction of so-called cleaner production technologies.
This preventive approach—which also requires a more holistic approach—has at least four significant advantages for the world of work and the environment:
- Unlike end-of-pipe technologies, which create additional costs for the production process without usually providing improvements in productivity or economic return, cleaner production technologies often lead to improvements in productivity and in measurable economic returns. In other words, end-of-pipe technologies clean up the environment but usually do not help the balance sheet. Cleaner production technologies prevent environmental degradation while also creating viable economic benefits.
- Cleaner production technologies often lead to significant improvements in the efficient use of natural resources and energy (i.e., use less natural resources to achieve comparable outputs) and also often lead to decreases in the amount of—and the toxicity of—the wastes generated.
- Efforts to introduce cleaner production technologies can and should explicitly identify measures to also improve OHS performance within the enterprise.
- Worker involvement concerning the protection of health, safety and environment as part of the cleaner technology process will lead to improvements in worker morale, understanding and job performance—all of which are well-documented factors in achieving good quality production.
Environmental policies, legislation and regulation have evolved and are leading—or at least are trying to keep up with—this process of transition from control-based approaches to prevention-centred strategies.
Both end-of-pipe and cleaner production strategies, however, have direct consequences for employment protection and creation. It is clear that in many parts of the world, particularly in industrialized countries and transition economies, there are major opportunities for job creation related to clean-up and remediation activities. At the same time, cleaner production technologies also represent a vibrant new industry which will lead to the creation of new job opportunities and, of course, will require new efforts to meet skill and training requirements. This is particularly evident in the dire need to ensure that those workers involved in meeting the challenge of environmental remediation receive effective OHS and environmental training. While much attention is being given to the potential negative impact on employment of increased regulations and controls, in the field of environment, regulation and controls, if properly developed, can lead to the creation of new jobs and promote improved environmental and OHS performance.
Another critical change in perspective towards the environment has occurred since the 1960s: a shift from an exclusive focus on production processes to give attention also to the environmental consequences of the products themselves. The most obvious example is the automobile, where considerable efforts have been made to improve its environmental “efficiency”, although much animated debate remains over whether a more efficient car should be complemented by an efficient public transport system. But clearly, all products have some environmental implications—if not in their production or use, most certainly in their eventual disposal. This shift in emphasis has led to an increasing number of environmental laws and regulations concerning the use and disposal of products, even the restriction or elimination of certain products. It also has led to new analytical techniques such as environmental impact assessments, life-cycle analysis, risk assessment and environmental auditing (see the articles later in this chapter). These new, broader perspectives on environment have implications as well for the world of work—for example, upon conditions of work for those involved in the safe disposal of products and on future employment prospects for those involved in the manufacture, sale and servicing of prohibited and restricted products.
Another driving force for environmental policy has been the rather dramatic number and scope of major industrial accidents, particularly since the Bhopal disaster in 1984. Bhopal and other major accidents like Chernobyl and the Exxon Valdez, demonstrated to the world—the public, politicians, employers and workers—that the traditional view that what happened within the gates of the workplace could not or would not affect the external environment, the general public or the health and livelihood of surrounding communities, is false. While major accidents had occurred before, the global, visual coverage of these events shocked wide segments of the public in developed and developing countries and transitional economies into a new awareness and support for environmental protection which would also protect workers and the public. It should be noted, however, that this provides another similarity to the history of action to improve occupational health and safety laws and regulations, which was also significantly promoted, for example, following early major factory fires and mining disasters.
One of the most obvious examples of the effects of these environmental driving forces, and particularly recent major “environmental” accidents, may be seen within the ILO itself, as reflected in recent decisions by its tripartite constituents. For example, the ILO has significantly enhanced its activities related to environment and the world of work. Most importantly, since 1990 three major sets of ILO working environment Conventions and Recommendations have been adopted:
- Convention No. 170 and Recommendation No. 177 concerning Safety in the Use of Chemicals at Work (1990)
- Convention No. 174 and Recommendation No. 181 concerning the Prevention of Major Industrial Accidents (1992)
- Convention No. 176 and Recommendation No. 183 concerning Safety and Health in Mines (1995).
These standards reflect an explicit extension of the traditional ILO scope from that of an exclusive focus on worker protection to also include a more holistic approach to these matters by references in the preambular or operative paragraphs to relevant aspects of the protection of the public and the environment. For example, Article 3 of Convention No. 174 states that the term major accident means “a sudden occurrence leading to a serious danger to workers, the public or environment, whether immediate or delayed”, and Article 4 states: “each Member shall formulate, implement and periodically review a coherent national policy concerning the protection of workers, the public and the environment against risk of major accidents.” The ILO’s wide range of Conventions and Recommendations related to the working environment provides a very useful source of guidance for countries working to improve their OHS and environmental performance. In this regard, it may also be useful to note that the ILO provides advisory assistance and support to its tripartite constituents with a view to helping them to ratify and implement relevant ILO standards.
In addition to these driving forces, however, there is a wide range of other factors which significantly influence the relationship between the working environment and the general environment. Clearly one of the most obvious is that despite many common concerns and issues (e.g., chemicals, accidents, health) the OHS and environmental aspects are often governed by different government ministries, different legislation, regulations and standards, and different enforcement and inspection mechanisms. These differences lead to considerable confusion, possibly additional costs as a result of duplication and, most disconcerting, to the existence of possible gaps which may lead to serious omissions concerning the protection of workers, the public and the environment. For example, recent reviews of a number of national inspectorates have drawn attention to potential problems of duplication, gaps and inconsistencies in the responsibilities assigned to factory, labour and environmental inspectorates. These reviews have also cited examples of situations in which labour inspectorates have been assigned new environmental inspection responsibilities without receiving adequate new staff and financial resources or specialized training. This has tended to deflect existing staff away from fully meeting their OHS inspection responsibilities. In addition, in many countries these legislative and inspectorate responsibilities still remain extremely limited and are not receiving adequate political and financial support. More emphasis will need to be given to developing a more integrated approach to the monitoring, enforcement and dispute settlement mechanisms related to OHS and environment regulations and standards.
While inspectorates will be essential components in any OHS and environmental protection system, by themselves they can never be sufficient. Workplace health and safety and the link between environment and the world of work will need to remain largely the responsibility of those at the enterprise level. The best way to ensure optimal performance is to ensure optimum confidence and collaboration between the workforce and management. This will need to be supported by effective training of workers and management as well as efficient joint mechanisms to support collaboration. These efforts at the enterprise level will be all the more successful if they are supported by good relations with, and access to, an adequately financed, well-trained and independent inspectorate.
The present wave of support for deregulation and structural adjustment, particularly within the public sector, if properly designed and implemented could lead to the more effective and efficient management of occupational safety and health and environmental protection. However, there are very troubling signs that suggest that this process may also lead to a deterioration of both OHS and environmental performance if governments, employers, workers and the public do not give adequate priority to these issues. All too often, OHS and environment are seen as issues which can be dealt with “later”, once more immediate economic requirements have been met. Experience suggests, however, that today’s short-term savings may lead to expensive remediation activities in the future to rectify the problems which could have been prevented at lower costs today. OHS and environment should not simply be seen as end-of-pipe and unproductive costs but rather as critical and productive social, environmental and economic investments.
Collaborative action between employers and workers at the workplace to deal with OHS issues has a long history and has clearly demonstrated its value. It is interesting to note that initially OHS issues were considered the exclusive prerogative of employers. Nevertheless, today, following very extensive efforts by the social partners, OHS issues are now seen as a matter of bipartite and/or tripartite collaboration in most countries throughout the world. In fact, many countries have established legislation requiring the creation of joint occupational health and safety committees at the workplace.
Here again, however, similar paths of development between OHS and environment are evident. When workers and their trade unions first raised issues of occupational health and safety as issues of direct concern to them, they were often dismissed as not having the knowledge and technical competence to understand or to deal with these issues. It has taken decades of dedicated effort for workers and their unions to demonstrate their fundamental role in understanding and effectively responding to these issues at the enterprise level. Workers had to insist that it was their health and safety and that they had a right to be involved in the process leading to decisions, and a positive contribution to make. Similarly, many employers and their organizations have come to recognize the benefits which have come from this collaborative process. Today, workers and their trade unions are often confronted with similar dismissive attitudes by some employers as regards their capacity and right to contribute to environmental protection. It should also be noted, however, that it is again the far-sighted and responsible employers in a limited number of high-profile sectors who are in the forefront of recognizing the talent, experience and practical common sense approach which workers can provide to improving environmental performance, and who support a well-trained, well-motivated, fully informed and fully involved workforce.
Nevertheless, some employers still argue that environment is an exclusive management responsibility and have opposed the establishment of joint safety, health and environment committees or separate joint environmental committees. Others have recognized the very critical and practical contribution that collaborative employer/worker action can make to ensuring that enterprises set and meet appropriate environmental performance standards. Such standards are no longer restricted to simply meeting mandatory legal requirements, but also include voluntary action to respond to the needs of local communities, global competitiveness, green marketing and so on. Voluntary environmental performance policies and programmes within individual enterprises or through sectoral associations (e.g., the chemical industries Responsible Care programme) often explicitly integrate both OHS and environmental considerations. Similarly, specialized and often voluntary standards prepared by organizations such as the International Organization for Standardization (ISO) also have had an increasing influence on both OHS and environmental protection.
The positive experience with collaboration between employers’ and workers’ organizations has also led to new collaborative partnerships and alliances which go beyond the workplace to ensure that all the stakeholders concerned with safety, health and environment are able to constructively participate in the process. Within the ILO we have called this new effort to expand collaborative links beyond the workplace to local community groups, environmental NGOs and other institutions involved in helping to make improvements in the world of work, “tripartite-plus” collaboration.
Several emerging issues are on the horizon which may lead to special challenges and opportunities for more effective linkages between OHS and environment. Two sectors which have been particularly difficult to reach as regards both OHS and environmental performance are small- and medium-sized enterprises (SMEs) and the urban informal sector. This is especially relevant as regards the awesome implications of one of the most critical environmental and developmental challenges of the 21st century: clean water and sanitation. New participatory approaches will need to be developed in order to better communicate the significant risks for workers and the environment related to many existing activities. Beyond the risks, however, there are also new opportunities to make improvements in productivity and to increase incomes from traditional activities, as well as the prospect of the creation of new income-generating activities directly related to the environment. Given the many direct and indirect linkages between the formal sector and SMEs and the urban informal sector, innovative approaches need to be designed which will facilitate the sharing of experiences on ways to improve OHS and environmental performance. Employers’ and workers’ organizations could play a very positive and practical role in this process.
Another emerging issue area is that of indoor air pollution. In the past we have tended to see large industrial establishments as the primary target to correct unhealthy working conditions. Today, however, there is growing recognition that many offices and commercial premises may also be encountering new occupational health problems due to indoor air pollution. This pollution is related to the increased use of chemicals and electronic equipment, intake of contaminated ambient air, the use of closed air recirculation and air conditioning systems, and the possible increased sensitivity of workers as a result of changing health patterns—for example, the growing number of cases of allergies and asthma. It may be expected that action to respond to indoor air pollution concerns will require a more integrated approach to both OHS and environmental factors than has been the case in the past.
Links to Sustainable Development
This article has so far briefly and superficially highlighted some of the past and potential future inter-relationships between OHS and the environment. This, however, already should be seen as a rather narrow perspective compared to the more holistic and integrated approach represented by the concept of sustainable development. This concept was the key—if not the “magic formula”—underlying the preparatory process to negotiate and endorse Agenda 21, the action plan for the 21st century adopted at the United Nations Conference on Environment and Development (UNCED) in Rio de Janeiro in June 1992 (see Robinson 1993). The concept of sustainable development is and will continue to be the subject of great discussion, debate and dispute. Much of this debate has been focused on semantics. For the purpose of this article, sustainable development represents both a goal and a process. As a goal, sustainable development implies development which equitably meets the needs of today’s and future generations. As a process, it means setting policies in such a way that they take into account not only economic factors but environmental and social factors as well.
If such a holistic concept is to be successfully operationalized, then the approach to all these factors will require new analysis and responses. It is essential that OHS issues become a fundamental factor in evaluating future investment and development decisions at all levels from the workplace to the negotiation of international standards. The protection of workers will need to be assessed not simply as one of the costs of doing business, but as a critical factor necessary to the achievement of economic, environmental and social objectives which are an integral part of sustainable development. This means that the protection of workers should be seen and calculated as an investment with a potentially positive rate of return within projects aimed at the achievement of environmental, social and economic objectives. The protection of workers as well cannot simply be seen as protecting them at their workplace, but should take into account the inter-relationship between their work, general health, living conditions (water, sanitation, housing), transport, culture and so on. It also implies that action to improve OHS is a prerequisite for meeting the basic economic and social development perspectives in developing countries, and not simply a luxury to be reserved for the rich countries.
As the Director-General of the ILO, Michel Hansenne, stated in his Report to the International Labour Conference in 1990:
There is in fact one central issue which pervades almost every environmental policy discussion—how to share equitably the costs and benefits of environmental action. “Who will pay for environmental improvements?” is a question which will need to be discussed and resolved at all levels, from the perspective of consumers, workers, employers, as well as from that of local, national, regional and international institutions.
For the ILO, the social and human implications of how these potential environmental costs and benefits are shared within society and between countries may be as important as the environmental actions themselves. An inequitable sharing of the social, economic and environmental costs and benefits of development, within and between countries, cannot lead to global sustainable development. Rather, it could accentuate poverty, injustice and division (ILO 1990).
In the past, and too frequently still today, workers have been called upon to pay an inequitable part of the costs of economic development through deplorable safety and health conditions (e.g., the tragic fire at the Kader Industrial Toy Company in Thailand, which took the lives of 188 workers), inadequate wages (insufficient income to meet basic family needs of food, shelter, education), lack of freedom of association and even the loss of human dignity (e.g., the use of bonded child labour). Similarly, workers and their local communities also have assumed much of the direct costs of day-to-day environmental degradation or decisions to close plants for environmental reasons. It also should be remembered that while most attention in industrialized countries has been focused on ways to avoid the potential loss of jobs as a result of environmental legislation and regulations, millions of people have already lost or have had their traditional livelihoods severely reduced as a result of ongoing desertification, deforestation, flooding and soil erosion.
Sustainable development implies that these environmental and social costs which have been “externalized” by industry and society in the past must now be internalized and reflected in the market costs of products and services. This internalization process is being encouraged by market forces and consumer groups, new laws and regulations including so-called economic instruments, as well as by decisions taken by the enterprises themselves. Nevertheless, to be successful this process of integrating the actual social and environmental costs of production and consumption will require new approaches to collaboration, communication and participation in decision-making processes. Workers’ and employers’ organizations have a critical stake in this process. They should also have a say in its design, implementation and monitoring.
In this context it may be useful to draw attention to the major diplomatic effort under way as part of the follow-up process of the UNCED Conference to facilitate an examination of the current imbalances in the global patterns of production and consumption. Chapter 4 of
Agenda 21, entitled “Changing Consumption Patterns”, indicates that action is needed to meet the following objectives:
(a) to promote patterns of consumption and production that reduce environmental stress and will meet the basic needs of humanity
(b) to develop a better understanding of the role of consumption and how to bring about more sustainable consumption patterns.
It also clearly encompasses the concept of the need for greatly expanding the basic consumption of millions of people in many parts of our world currently confronted with dire poverty and hardship. Ongoing negotiations and discussions within the framework of the Commission on Sustainable Development (CSD) may be expected to be very slow and complex. Nevertheless they could lead to significant changes in present production and consumption patterns, particularly in some of the most critical industrial sectors of our economies, including chemicals, energy and transport. They also will have significant repercussions on international trade and commerce. Such changes will no doubt also have important implications for OHS and environment practices in developed and developing countries and for many other areas of the world of work, especially employment, incomes and training.
Although these issues currently are being discussed primarily at the global level, it is obvious that it is at each workplace where they will need to be implemented. Therefore, it is essential that this global negotiation process reflect reality, that is, the constraints and opportunities at the workplace level all across our planet. With the globalization of our economies, and the rapid changes in the organization and structures of our workplaces (e.g., sub-contracting, part-time work, homeworkers, teleworking), and indeed changes in our perception of work, livelihoods and employment itself in the 21st century, this will be no easy task. If this process is to be successful, however, it will require the support of a tripartite collaborative process between governments and employers’ and workers’ organizations at all stages. Clearly such a bottom-up approach will play a vital role in guiding the national and global CSD process to achieve more sustainable production and consumption patterns in the future.
Conclusion
Articles in this chapter focus on action at the national and international levels as well as on practical policy tools to improve environmental performance. It is clear, however, that the most important environmental policies of the future will not be set at the national or international level or even by local communities—although each of these has an essential role to play. The real changes must and will come at the enterprise and workplace level. From the chief executive officer of large multinational corporations to the managers of small family businesses to rural farmers and independent workers in the informal sector will come the true impetus and commitment to follow through to achieve sustainable development. Change will be possible only through the growing awareness and joint action by employers and workers within enterprises and other relevant sectors (e.g., local communities, non-governmental organizations, etc.) to integrate OHS and environmental objectives within the overall objectives and priorities of the enterprise. Despite the magnitude of the challenge, one can foresee the range of formal and informal safety, health and environmental policies at the enterprise level developed, implemented and monitored by a collaborative process between management and workers and other stakeholders.
Occupational health and safety clearly has a significant impact on the achievement of our overall economic, environmental and social objectives. Therefore, OHS must be seen as a critical element to be included within the complex integration process to achieve sustainable development. Following the UNCED Conference, all national governments have been called upon to develop their own national Agenda 21 strategies and plans for sustainable development. Environmental objectives already are seen as an integral part of that process. Much work remains, however, before OHS and employment and social objectives and targets will become an explicit and intrinsic part of that process and the economic and political support necessary for the achievement of those objectives is mobilized.
The preparation of this article has been greatly facilitated by the technical support, useful advice and comments and regular encouragement from colleagues, governments, employers and workers from around the world who are keenly committed and competent in this field, but particularly key representatives from the International Federation of Chemical, Energy and General Workers’ Unions (ICEF); Canadian Labour Congress; the Communications, Energy and Paper Workers’ Unions of Canada; and the Labourers’ International Union of North America, who have stressed the urgent need for action in this field.
Overview: Occupational Safety and Health and the Environment - Two Sides of the Same Coin
This is the first edition of the Encyclopaedia of Occupational Health and Safety to explicitly integrate relevant environmental issues within its scope. This chapter highlights a number of basic environmental policy issues which are increasingly linked to occupational safety and health. Other specialized environmental chapters include Environmental Health Hazards and Environmental Pollution Control. In addition, a special effort has been made to include sections concerning environment within each of the chapters on key industrial sectors. When first considering whether such a strategy to integrate environmental issues was indeed warranted in the Encyclopaedia, we began with the very limited perspective of including only a single chapter which would serve as a useful “cross-reference” demonstrating how occupational safety and health issues and the working environment have become increasingly linked to environmental issues. As the ILO has been stating for the past twenty-plus years: the working environment and the general environment represent “two sides of the same coin”.
It is also blatantly clear, however, that the magnitude and scope of the challenges this “two-sided coin” represents for the workers of this world are grossly underestimated and under-targeted for action. The meritable successes which receive legitimate attention and praise in this Encyclopaedia risk leading us towards a dangerous and false sense of security and confidence as regards the present state of the art in occupational safety and health and the environment. The very best of our technologies, management practices and tools have indeed made impressive strides towards remediating and preventing problems in a number of key sectors, particularly in industrialized countries. But it is also true that the global reach of these technologies, management practices and tools is indeed insufficient and limited, especially in developing countries and in transition economies.
This chapter describes a few of the most useful tools and practices available to deal with occupational health and safety and environmental problems and challenges, although it would be misleading to suggest that these are already in fact widely applied throughout the world. It is important, however, that occupational health and safety practitioners all over the world learn more about these tools and practices as a step towards their greater application and practical adaptation to different economic and social conditions.
The first article in this chapter provides a brief review of inter-relationships between occupational safety and health and the working environment, policies and issues related to the general environment and the concept of “sustainable development”. This concept became the guiding principle for Agenda 21, the action plan for the 21st century adopted at the United Nations Conference on Environment and Development (UNCED) in Rio de Janeiro in June 1992. The past comfortable—and yet seriously misleading—view that it was not only possible but essential to differentiate problems and responses between those that deal with action at the workplace and those that deal with what occurs outside the gates of the enterprise has become blurred. In fact, today both workers and employers and their organizations have begun to recognize explicitly that the enterprise gate is far from impermeable to the effects of policies and problems encountered on both sides of that gate.
Given the growing recognition that occupational safety and health issues may have been treated in too isolated a manner in the past, this chapter provides a series of brief descriptions of a number of environmental policy issues which occupational safety and health practitioners may find particularly relevant to their own activities and concerns. The chapter contains two articles on environmental law and regulations which describe the present state of the art as regards the rapid expansion of international and national legal responses to existing and potential future environmental problems and concerns.
The chapter contains four articles describing some of the most important environmental policy tools being used today to improve environmental performance not only in industry, but also in all other sectors of our economy and throughout our societies. The articles focus upon environmental impact assessments, life-cycle analysis, risk assessment and communication and environmental auditing. The final section of this chapter provides two perspectives on pollution prevention and control: one focusing on making pollution prevention a corporate priority and the other providing a trade union perspective of pollution prevention and cleaner production technologies.
The overall objective of this chapter is to enable the reader to better perceive and understand the growing inter-relationships between occupational safety and health and the working environment, and the broader environmental issues beyond the workplace. A greater recognition of these linkages will hopefully also lead to more extensive and effective exchanges of experience and information between occupational health and safety and environmental specialists, with a view to enhancing our capacity to respond to challenges in the working environment and beyond.
Case Study: Occupational Health Surveys in China
To understand the magnitude of occupational health problems in China, the Ministry of Public Health (MOPH) has organized a number of nationwide surveys, including the following:
- a survey on occupational exposures to benzene, lead, mercury, TNT and organophosphates (1979-81)
- a retrospective epidemiological investigation on occupational cancers in workers exposed to eight chemicals (1983-85)
- an epidemiological survey on pneumoconioses (1952-86)
- a survey on occupational health problems of small-scale industries and the relevant intervention strategies (1984-85, 1990-92).
The results of these surveys have served as a very important foundation for formulating national policies and regulations. At the same time, a national occupational health reporting system has been established by MOPH. The Annual Report of the National Occupational Health Situation has been published since 1983. The data are compiled and analysed by the National Center of Occupational Health Reporting (NCOHR) and then reported to the MOPH. There are local reporting offices in Occupational Health Institutes (OHIs) or Health Epidemic Prevention Stations (HEPS) at all levels from county to province. The reporting follows a “bottom-up” procedure annually, but, if an acute poisoning accident happened which involved three or more cases of poisoning or one death, it must be reported to the local OHI and also directly to the MOPH within 24 hours by the primary-contact medical institutions. The information required to be reported every year includes the following: registered new cases of compensable occupational diseases, the results of health examinations of workers and the monitoring of working environments (MOPH 1991). China is currently promoting the computerization of the reporting system and its computer network. It currently extends from the national centre to the provincial offices.
Measurement Strategies and Techniques for Occupational Exposure Assessment in Epidemiology
Other articles in this chapter present general principles of medical surveillance of occupational illnesses and exposure surveillance. This article outlines some principles of epidemiological methods that may be used to fulfil surveillance needs. Application of these methods must take into account basic principles of physical measurement as well as standard epidemiological data-gathering practice.
Epidemiology can quantify the association between occupational and non-occupational exposure to chemico-physical stressors or behaviour and disease outcomes, and can thus provide information to develop interventions and prevention programmes (Coenen 1981; Coenen and Engels 1993). Availability of data and access to workplace and personnel records usually dictate the design of such studies. Under the most favourable circumstances, exposures can be determined through industrial hygiene measurements that are carried out in an operating shop or factory, and direct medical examinations of workers are used to ascertain possible health effects. Such evaluations can be done prospectively for a period of months or years to estimate risks of diseases such as cancer. However, it is more often the case that past exposures must be reconstructed historically, projecting backwards from current levels or using measurements recorded in the past, which may not completely meet informational needs. This article presents some guidelines and limitations for measurement strategies and documentation that affect epidemiological assessment of workplace health hazards.
Measurements
Measurements should be quantitative wherever possible, rather than qualitative, because quantitative data are subject to more powerful statistical techniques. Observable data are commonly classified as nominal, ordinal, interval and ratio. Nominal level data are qualitative descriptors which differentiate only types, such as different departments within a factory or different industries. Ordinal variables may be arranged from “low” to “high” without conveying further quantitative relationships. An example is “exposed” vs. “unexposed”, or classifying smoking history as non-smoker (= 0), light smoker (= 1), medium smoker (= 2) and heavy smoker (= 3). The higher the numerical value, the stronger the smoking intensity. Most measurement values are expressed as ratio or interval scales, in which a concentration of 30 mg/m3 is double the concentration of 15 mg/m3. Ratio variables possess an absolute zero (like age) while interval variables (like IQ) do not.
Measurement strategy
Measurement strategy takes into account information about the measurement site, the surrounding conditions (e.g., humidity, air pressure) during the measurement, the duration of the measurement and the measurement technique (Hansen and Whitehead 1988; Ott 1993).
Legal requirements often dictate measurement of eight-hour time-weighted averages (TWAs) of levels of hazardous substances. However, not all individuals work eight-hour shifts all the time, and levels of exposures may fluctuate during the shift. A value measured for one person’s job might be considered representative of an eight-hour shift value if the exposure duration is longer than six hours during the shift. As a practical criterion, a sampling duration of at least two hours should be sought. With time intervals that are too short, the sampling in one time period can show higher or lower concentrations, thereby over- or underestimating the concentration during the shift (Rappaport 1991). Therefore, it can be useful to combine several measurements or measurements over several shifts into a single time-weighted average, or to use repeated measurements with shorter sampling durations.
Measurement validity
Surveillance data must satisfy well-established criteria. The measurement technique should not influence the results during the measurement process (reactivity). Furthermore, the measurement should be objective, reliable and valid. The results should not be influenced either by the measurement technique used (execution objectivity) or by the reading or documentation by the measurement technician (assessment objectivity). The same measurement values should be obtained under the same conditions (reliability); the intended thing should be measured (validity) and interactions with other substances or exposures should not unduly influence the results.
Quality of Exposure Data
Data sources. A basic principle of epidemiology is that measurements made at the individual level are preferable to those made at the group level. Thus, the quality of epidemiolological surveillance data decreases in the following order:
- direct measurements taken of persons; information on exposure levels and time progression
- direct measurements taken of groups; information on current exposure levels for specific groups of workers (sometimes expressed as job-exposure matrices) and their variation over time
- measurements abstracted or reconstructed for individuals; estimation of exposure from company records, purchasing lists, descriptions of product lines, interviews with employees
- measurements abstracted or reconstructed for groups; historical estimation of group-based exposure indexes.
In principle, the most precise determination of the exposure, using documented measurement values over time, should always be sought. Unfortunately, indirectly measured or historically reconstructed exposures are often the only data available for estimating exposure-outcome relationships, even though considerable deviations exist between measured exposures and exposure values reconstructed from company records and interviews (Ahrens et al. 1994; Burdorf 1995). The quality of the data declines in the order exposure measurement, activity-related exposure index, company information, employee interviews.
Exposure scales. The need for quantitative monitoring data in surveillance and epidemiology goes considerably beyond the narrow legal requirements of threshold values. The goal of an epidemiological investigation is to ascertain dose-effect relation-ships, taking into account potentially confounding variables. The most precise information possible, which in general can be expressed only with a high scale level (e.g., ratio scale level), should be used. Separation into larger or smaller threshold values, or coding in fractions of threshold values (e.g., 1/10, 1/4, 1/2 threshold value) as is sometimes done, essentially relies on data measured on a statistically weaker ordinal scale.
Documentation requirements. In addition to information on the concentrations and the material and time of measurement, external measurement conditions should be documented. This should include a description of the equipment used, measurement technique, reason for the measurement and other relevant technical details. The purpose of such documentation is to ensure uniformity of measurements over time and from one study to another, and to permit comparisons between studies.
Exposure and health outcome data gathered for individuals are usually subject to privacy laws that vary from one country to another. Documentation of exposure and health conditions must adhere to such laws.
Epidemiological Requirements
Epidemiological studies strive to establish a causal link between exposure and disease. Some aspects of surveillance measurements that affect this epidemiological assessment of risk are considered in this section.
Type of disease. A common starting point for epidemiological studies is the clinical observation of a surge in a particular disease in a company or area of activity. Hypotheses on potential biological, chemical or physical causal factors ensue. Depending on the availability of data, these factors (exposures) are studied using a retrospective or prospective design. The time between the beginning of the exposure and the onset of the disease (latency) also affects study design. The range of latency can be considerable. Infections from certain enteroviruses have latency/incubation times of 2 to 3 hours, whereas for cancers latencies of 20 to 30 years are typical. Therefore, exposure data for a cancer study must cover a considerably longer period of time than for an infectious disease outbreak. Exposures which began in the distant past can continue up to the onset of disease. Other diseases associated with age, such as cardiovascular disease and stroke, can appear in the exposed group after the study begins and must be treated as competing causes. It is also possible that people classified as “not sick” are merely people who have not yet manifested clinical illness. Thus, continued medical surveillance of exposed populations must be maintained.
Statistical power. As previously stated, measurements should be expressed on as high a data level (ratio scale level) as possible in order to optimize the statistical power to produce statistically significant results. Power in turn is affected by the size of the total study population, the prevalence of exposure in that population, the background rate of illness and the magnitude of risk of the disease that is caused by the exposure under study.
Mandated disease classification. Several systems are available for codifying medical diagnoses. The most common are ICD-9 (International Classification of Diseases) and SNOMED (Systematic Nomenclature of Medicine). ICD-O (oncology) is a particularization of the ICD for codifying cancers. ICD coding documentation is legally mandated in many health systems throughout the world, especially in Western countries. However, SNOMED codification can also codify possible causal factors and external conditions. Many countries have developed specialized coding systems to classify injuries and illnesses that also include the circumstances of the accident or exposure. (See the articles “Case study: Worker protection and statistics on accidents and occupational diseases—HVBG, Germany” and “Development and application of an occupational injury and illness classification system”, elsewhere in this chapter.)
Measurements that are made for scientific purposes are not bound by the legal requirements that apply to mandated surveillance activities, such as determination of whether threshold limits have been exceeded in a given workplace. It is useful to examine exposure measurements and records in such a way as to check for possible excursions. (See, for example, the article “Occupational hazard surveillance” in this chapter.)
Treatment of mixed exposures. Diseases often have several causes. Therefore it is necessary to record as completely as possible the suspected causal factors (exposures/confounding factors) in order to be able to distinguish the effects of suspected hazardous agents from one another and from the effects of other contributory or confounding factors, such as cigarette smoking. Occupational exposures are often mixed (e.g., solvent mixtures; welding fumes such as nickel and cadmium; and in mining, fine dust, quartz and radon). Additional risk factors for cancers include smoking, excess alcohol consumption, poor nutrition and age. Besides chemical exposures, exposures to physical stressors (vibration, noise, electromagnetic fields) are possible triggers for diseases and must be considered as potential causal factors in epidemiological studies.
Exposures to multiple agents or stressors may produce interaction effects, in which the effect of one exposure is magnified or reduced by another that occurs contemporaneously. A typical example is the link between asbestos and lung cancer, which is many times more pronounced among smokers. An example of the mixture of chemical and physical exposures is progressive systemic scleroderma (PSS), which is probably caused by a combined exposure to vibration, solvent mixtures and quartz dust.
Consideration of bias. Bias is a systematic error in classifying persons in the “exposed/not exposed” or “diseased/not diseased” groups. Two types of bias should be distinguished: observation (information) bias and selection bias. With observation (information) bias, different criteria may be used to classify subjects into the diseased/not diseased groups. It is sometimes created when the target of a study includes persons employed in occupations known to be hazardous, and who may already be under increased medical surveillance relative to a comparison population.
In selection bias two possibilities should be distinguished. Case-control studies begin by separating persons with the disease of interest from those without that disease, then examine differences in exposure between these two groups; cohort studies determine disease rates in groups with different exposures. In either type of study, selection bias exists when information on the exposure affects classification of subjects as sick or not sick, or when information on disease status affects classification of subjects as exposed or not exposed. A common example of selection bias in cohort studies is the “healthy worker effect”, which is encountered when disease rates in exposed workers are compared with those in the general population. This can result in underestimation of disease risk because working populations are often selected from the general population on the basis of continued good health, frequently based upon medical examination, whereas the general population contains the ill and infirm.
Confounders. Confounding is the phenomenon whereby a third variable (the confounder) alters the estimate of an association between a presumed antecedent factor and a disease. It can occur when the selection of subjects (cases and controls in a case-control study or exposed and unexposed in a cohort study) depends in some way upon the third variable, possibly in a manner unknown to the investigator. Variables associated only with exposure or disease are not confounders. To be a confounder a variable must meet three conditions:
- It must be a risk factor for the disease.
- It must be associated with the exposure in the study population.
- It must not be in the causal pathway from exposure to disease.
Before any data are collected for a study it is sometimes impossible to predict whether or not a variable is a likely confounder. A variable which has been treated as a confounder in a previous study might not be associated with exposure in a new study within a different population, and would therefore not be a confounder in the new study. For instance, if all subjects are alike with respect to a variable (e.g., sex), then that variable cannot be a confounder in that particular study. Confounding by a particular variable can be accounted for (“controlled”) only if the variable is measured along with exposure and illness outcomes. Statistical control of confounding may be done crudely using stratification by the con-founding variable, or more precisely using regression or other multivariate techniques.
Summary
The requirements of measuring strategy, measuring technology and documentation for industrial workplaces are sometimes statutorily defined in terms of threshold limit value surveillance. Data protection regulations also apply to the protection of company secrets and person-related data. These requirements call for the comparable measuring results and measurement conditions and for an objective, valid and reliable measuring technology. Additional requirements put forward by epidemiology refer to the representativeness of measurements and to the possibility of establishing links between exposures for individuals and subsequent health outcomes. Measurements may be representative for certain tasks, i.e. they may reflect typical exposure during certain activities or in specific branches or typical exposure of defined groups of persons. It would be desirable to have measurement data directly attributed to the study subjects. This would make it necessary to include with measurement documentation information about persons working at the concerned workplace during the measurement or to set up a registry allowing such direct attribution. Epidemiological data collected at the individual level are usually preferable to those obtained at the group level.
Case study: Wismut - A Uranium Exposure Revisited
Historical Development
The Erz mountains have been mined since the twelfth century, and beginning in 1470 silver mining brought the area to prominence. Around the year 1500 the first reports of a specific disease among miners appeared in Agricola’s writings. In 1879 this disease was recognized by Haerting and Hesse as lung cancer, but at that time what caused it was not clear. In 1925 “Schneeberg lung cancer” was added to the list of occupational diseases.
The material from which Marie Curie isolated the elements radium and polonium came from the slag heap of the Joachimstal (Jachymov) in Bohemia. In 1936 Rajewsky’s radon measurements near Schneeberg confirmed the already assumed connection between radon in the mining shafts and lung cancer.
In 1945 the Soviet Union intensified its atomic weapons research programme. The search for uranium was extended to the Erz Mountains, as the conditions for mining were better there than in the Soviet deposits. After initial inquiries, the whole area was placed under Soviet military administration and declared a restricted zone.
From 1946 to 1990 the Soviet Wismut Company (SAG), later the Soviet-German Wismut Company (SDAG), carried out uranium mining in Thuringia and Saxony (figure 1). At the time the Soviet Union was under pressure to obtain sufficient quantities of uranium to construct the first Soviet atomic bomb. Appropriate equipment was not available, so achieving the necessary level of uranium production was possible only by disregarding safety measures. Working conditions were especially bad in the years 1946 to 1954. According to an SAG Wismut health report, 1,281 miners had fatal accidents and 20,000 suffered injuries or other detrimental effects to their health just in the second half of 1949.
Figure 1. Mining areas of SDAG Wismut in East Germany
In post-war Germany, the Soviet Union considered uranium mining a form of reparations. Prisoners, conscripts and “volunteers” were mobilized, but at first there were hardly any skilled personnel. In all, Wismut employed between 400,000 and 500,000 people (figure 2).
Figure 2. Wismut employees 1946-90
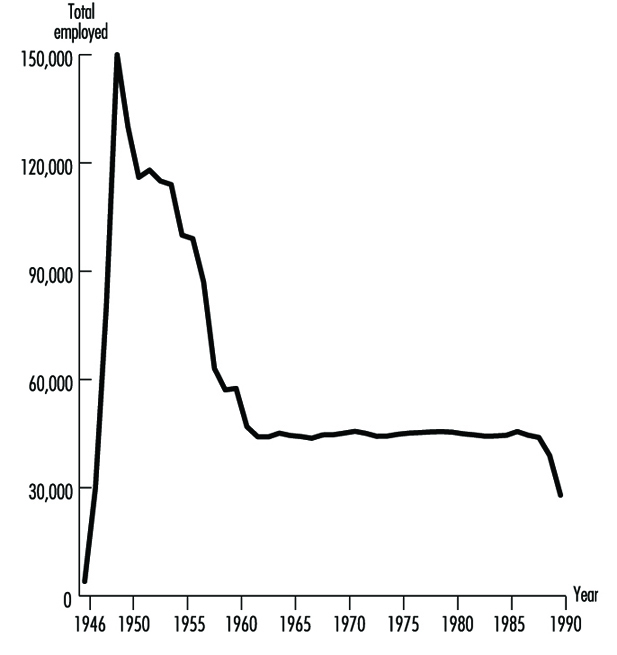
Bad working conditions, the lack of suitable technology and intense work pressure led to extremely high numbers of accidents and illnesses. The working conditions gradually improved beginning in 1953, when German participation in the Soviet company began.
Dry-drilling, which produced high levels of dust, was employed from 1946 to 1955. No artificial ventilation was available, resulting in high radon concentrations. In addition, the workers’ health was adversely affected by the extremely heavy labour due to the lack of equipment, the lack of safety gear and long work shifts (200 hours per month).
Figure 3. Exposure records of former SDAG Wismut
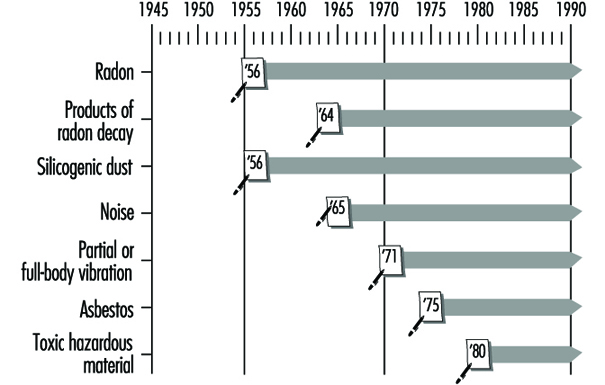
The exposure level varied over time and from shaft to shaft. The systematic measurement of the exposure also ensued in different phases, as is shown in figure 3. The exposures to ionizing radiation (shown in Working Level Months (WLM)) can be given only very roughly (table 1). Today, comparisons with radiation-exposure situations in other countries, measurements made under experimental conditions and assessments of written records permit a more precise statement of the exposure level.
Table 1. Estimates of radiation exposure (Working Level Months/Year) in the Wismut mines
|
Year |
WLM/Year |
|
1946–1955 |
30–300 |
|
1956–1960 |
10–100 |
|
1961–1965 |
5–50 |
|
1966–1970 |
3–25 |
|
1971–1975 |
2–10 |
|
1976–1989 |
1–4 |
In addition to intensive exposure to rock dust, other factors relevant to illnesses were present, such as uranium dust, arsenic, asbestos and emissions from explosives. There were physical effects from noise, hand-arm vibrations and whole-body vibrations. Under these conditions, silicoses and radiation-related bronchial carcinomas dominate the record of occupational diseases from 1952 to 1990 (table 2).
Table 2. Comprehensive overview of known occupational diseases in Wismut uranium mines 1952-90
|
List No. BKVO 1 |
Absolute number |
% |
|
|
Diseases due to quartz |
40 |
14,733 |
47.8 |
|
Malignant tumours or pretumours from ionizing radiation |
92 |
5,276 |
17.1 |
|
Diseases due to partial body vibration |
54 |
— |
— |
|
Diseases of tendons and extremity joints |
71–72 |
4,950 |
16.0 |
|
Impaired hearing due to noise |
50 |
4,664 |
15.1 |
|
Skin diseases |
80 |
601 |
1.9 |
|
Other |
— |
628 |
2.1 |
|
Total |
30,852 |
100 |
1 Occupational disease classification of the former GDR.
Source: Wismut Health System Annual Reports.
Although over time the health services of SAG/SDAG Wismut provided increasing levels of comprehensive care for the miners, including annual medical examinations, the effects on health of extracting the ore were not systematically analysed. Production and working conditions were kept strictly secret; the Wismut companies were autonomous and organizationally were a “state within a state”.
The full magnitude of the events became known only in 1989-90 with the end of the German Democratic Republic (GDR). In December 1990 uranium mining was discontinued in Germany. Since 1991 the Berufsgenossenschaften (preventing, recording and compensating industrial and trade associations), as the statutory accident insurance carrier have been responsible for recording and compensating all accidents and occupational diseases related to the former Wismut operation. This means that the associations are responsible for providing affected individuals with the best possible medical care and for collecting all relevant occupational health and safety information.
In 1990, approximately 600 claims for bronchial carcinoma were still pending with the Wismut social insurance system; some 1,700 cases of lung cancer had been turned down in earlier years. Since 1991 these claims have been pursued or reopened by the responsible Berufsgenossenschaften. On the basis of scientific projections (Jacobi, Henrichs and Barclay 1992; Wichmann, Brüske-Hohlfeld and Mohner 1995), it is estimated that in the next ten years between 200 and 300 cases of bronchial carcinomas per year will be recognized as resulting from working at Wismut.
The Present: After the Change
The production and working conditions at SDAG Wismut left their mark on both the employees and the environment in Thuringia and Saxony. In accordance with the law of the Federal Republic of Germany, the federal government took over responsibility for cleaning up the environment in the affected region. The costs of these activities for the period 1991-2005 have been estimated at DM 13 billion.
After the GDR joined the Federal Republic of Germany in 1990, the Berufsgenossenschaften, as statutory accident insurance carriers, became responsible for managing occupational diseases in the former GDR. In light of the particular conditions at Wismut, the Berufsgenossenschaften decided to form a special unit to handle occupational safety and health for the Wismut complex. To the extent possible, while respecting legal regulations protecting the privacy of personal data, the Berufsgenossenschaften secured records on former working conditions. Thus when the company was dissolved for economic reasons all evidence that could possibly serve to substantiate the claims of employees in case of illness would not be lost. The “Wismut Central Care Office” (ZeBWis) was established by the Federation on 1 January 1992 and bears responsibility for occupational medical treatment, early detection and rehabilitation.
From ZeBWis’s goal of providing appropriate occupational medical care to former uranium mining employees, four essential health surveillance tasks emerged:
- organizing mass screening examinations for early diagnosis and treatment of diseases
- documenting the screening findings and linking them with data from the occupational disease detection procedures
- scientifically analysing the data
- support of research on early detection and treatment of disease.
Screening is provided to the exposed workers in order to assure early diagnosis whenever possible. Ethical, scientific and economic aspects of such screening procedures require a thorough discussion which is beyond the scope of this article.
A programme of occupational medicine was developed, based on the well-founded trade association principles for special occupational medical examinations. Integrated into this were examination methods known from mining and radiation protection. The component parts of the programme follow from the main agents of exposure: dust, radiation and other hazardous materials.
The ongoing medical surveillance of former Wismut employees is aimed primarily at early detection and treatment of bronchial carcinomas resulting from exposure to radiation or other carcinogenic materials. Whereas the connections between ionizing radiation and lung cancers are proven with adequate certainty, the effects on health of long-term, low-dosage radiation exposure have been less researched. Current knowledge is based on extrapolations of data from survivors of the atomic bombings of Hiroshima and Nagasaki, as well as data obtained from other international studies of uranium miners.
The situation in Thuringia and Saxony is exceptional in that significantly more people underwent a much broader range of exposures. Therefore, a wealth of scientific knowledge can be gained from this experience. To what degree radiation works synergistically with exposure to carcinogens like arsenic, asbestos or diesel motor emissions in causing lung cancer should be scientifically examined using newly obtained data. The early detection of bronchial carcinomas through the introduction of state-of-the-art examination techniques should be an important part of the prospective scientific research.
Available Data from the Wismut Health System
In response to the extreme accident and health problems it faced, Wismut established its own health service, which provided, among other things, annual medical screening examinations, including chest x rays. In later years additional occupational disease examination units were set up. Since the Wismut health service took over not only occupational medicine, but also full medical care for employees and their dependents, by 1990 SDAG Wismut had collected comprehensive health information on many former and current Wismut employees. In addition to complete information on the occupational medical examinations, and a complete archive of occupational diseases, a comprehensive x-ray archive exists with over 792,000 x rays.
In Stollberg the Wismut health system had a central pathology department in which comprehensive histological and pathological material was collected from the miners, as well as from the inhabitants of the area. In 1994 this material was given to the German Cancer Research Center (DKFZ) in Heidelberg for safekeeping and research purposes. A portion of the records of the former health system was first taken over by the statutory accident insurance system. For this purpose, ZeBWis established a temporary archive at Shaft 371 in Hartenstein (Saxony).
These records are used for processing insurance claims, for preparing and administering occupational medical care and for scientific study. In addition to being used by the Berufsgenossenschaften, the records are available to experts and to authorized physicians in the context of their clinical work with and management of each former employee.
The core of these archives consists of the complete files of occupational diseases (45,000) which were taken over, together with the corresponding occupational disease tracing files (28,000), the tracing files for monitoring dust-endangered persons (200,000), as well as targeted documentary records with the results of the occupational medical fitness and monitoring examinations. In addition, the autopsy records of Stollberg Pathology are kept in this ZeBWis archive.
These last-mentioned records, as well as the occupational disease tracing files, have in the meantime been prepared for data processing. Both these forms of documentation will be used for extracting data for a 60,000-person comprehensive epidemiological study by the federal ministry for the environment.
In addition to the data on exposure to radon and radon by-products, the records on the exposure of former employees to other agents are of special interest to the Berufsgenossenschaften. Thus the present-day Wismut GmbH has measurement results available for viewing, in list form, from the early 1970s to the present for silicogenic dusts, asbestos dusts, heavy metal dusts, wood dusts, explosives dusts, toxic vapours, welding fumes, diesel motor emissions, noise, partial- and whole-body vibrations and heavy physical labour. For the years 1987 to 1990 the individual measurements are archived in electronic media.
This is important information for retrospective analysis of the exposures in Wismut’s uranium mining operations. It also constitutes the basis for constructing a job-exposure matrix which assigns exposures to tasks for research purposes.
To round out the picture, further records are stored in the department that safeguards health data at Wismut GmbH, including: patient files of former out-patients, accident reports by the former company and by occupational safety inspections, clinical occupational medical records, biological exposure tests, occupational medical rehabilitation and neoplastic disease reports.
However, not all Wismut archives—primarily paper files—were designed for centralized evaluation. Thus, with the dissolution of SDAG Wismut on 31 December 1990, and the dissolution of the Wismut company health system, the question was posed of what to do with these unique records.
Digression: Incorporating the Holdings
The first task for ZeBWis was to define the people who worked underground or in the preparation plants and to determine their current location. The holdings comprise some 300,000 people. Few of the company’s records were in a form that could be used in data processing. Thus it was necessary to tread the wearisome path of viewing one card at a time. The card files from nearly 20 locations had to be collected.
The next step was to collect the vital statistics and addresses of these people. Information from old personnel and wage records was not useful for this. Old addresses were often no longer valid, in part because a blanket renaming of streets, squares and roads took place after the unification treaty was signed. The Central Inhabitant Registry of the former GDR was also not useful, as by this time the information was no longer complete.
Finding these people was eventually made possible with the assistance of the Association of German Pension Insurance Carriers, through which addresses for nearly 150,000 people were collected to communicate the offer of free occupational medical care.
To give the examining doctor an impression of the hazards and exposure that the patient was subject to from the so-called occupational or work case history a job-exposure matrix was constructed.
Occupational Medical Care
Approximately 125 specially trained occupational physicians with experience in diagnosing dust- and radiation-caused diseases were recruited for the examinations. They work under the direction of ZeBWis and are spread throughout the Federal Republic to ensure that the affected individuals can obtain the indicated examination near their current place of residence. Due to intensive training of the participating physicians, standard high-quality examinations are performed at all examination locations. By distributing uniform documentation forms ahead of time, it is ensured that all relevant information is collected according to set standards and is entered into ZeBWis’s data centres. By optimizing the number of files, every examining doctor carries out an adequate number of exams every year and thereby remains practised and experienced in the examination programme. Through regular exchange of information and continuing education, the physicians always have access to current information. All examining physicians are experienced in assessing chest x rays in accordance with the 1980 ILO guidelines (International Labour Organization 1980).
The data pool, which is growing as a result of the ongoing examinations, is geared to acquaint physicians and risk assessment experts in the occupational disease detection programme with relevant preliminary findings. It furthermore provides a basis for addressing specific symptoms or diseases that appear under defined risk situations.
The Future
Comparing the number of people who worked for Wismut underground and/or in preparation plants with the number who were employed in uranium mining in the Western world, it is evident that, even with big gaps, the data on hand present an extraordinary basis for gaining new scientific understanding. Whereas the 1994 overview by Lubin et al. (1994) on the risk of lung cancer covered approximately 60,000 affected individuals and about 2,700 cases of lung cancer in 11 studies, the data from some 300,000 former Wismut employees are now available. At least 6,500 have died to date from radiation-caused lung cancer. Furthermore, Wismut never collected the exposure information on a great number of persons exposed either to ionizing radiation or other agents.
As precise information as possible on exposure is necessary for optimal occupational disease diagnosis as well as for scientific research. This is taken into account in two research projects that are being sponsored or carried out by the Berufsgenossenschaften. A job-exposure matrix was prepared by consolidating available site measurements, analysing geological data, using information on production figures and, in some cases, reconstructing working conditions in the early years of Wismut. Data of this type are a prerequisite for developing a better understanding, through cohort studies or case-control studies, of the nature and extent of illnesses that result from uranium mining. Understanding the effect of long-term, low-level radiation doses and the cumulative effects of radiation, dust and other carcinogenic materials might also be improved in this manner. Studies of this are now beginning or are being planned. With the help of biological specimens that were collected in Wismut’s former pathology laboratories, scientific knowledge can also be obtained about the type of lung cancer and also about the interactive effects between silicogenic dusts and radiation, as well as other carcinogenic hazardous materials that are inhaled or ingested. Such plans are being pursued at this time by the DKFZ. Collaboration on this issue is now underway between the German research facilities and other research groups such as the US NIOSH and the National Cancer Institute (NCI). Corresponding work groups in countries like the Czech Republic, France and Canada are also cooperating in studying the exposure data.
To what extent malignancies other than lung cancer may develop from radiation exposure during uranium ore mining is poorly understood. At the request of the trade associations, a model of this was developed (Jacobi and Roth 1995) to establish under what conditions cancers of the mouth and throat, liver, kidneys, skin or bones can be caused by working conditions such as those at Wismut.
Case Study: Worker Protection and Statistics on Accidents and Occupational Diseases - HVBG, Germany
The German Berufsgenossenschaften (BG)
Under the social insurance system in Germany, statutory accident insurance covers the results of accidents at work and accidents on the way to and from work, as well as occupational diseases. This statutory accident insurance is organized into three areas:
- industrial accident insurance (represented by the BGs)
- agricultural accident insurance
- public sector’s own accident insurance scheme.
The 35 Berufsgenossenschaften (BG) cover the various branches of the industrial economy in Germany. They are responsible for 39 million employees insured in 2.6 million enterprises. Every person in a work, service or training position is insured, regardless of age, sex or income level. Their umbrella organization is the Central Federation of the Berufsgenossenschaften (HVBG).
By law, the BG is responsible for using all appropriate means to prevent workplace accidents and occupational diseases, to provide effective first aid and optimal medical, occupational and social rehabilitation, and to pay benefits to the injured and sick, and to survivors. Thus prevention, rehabilitation and compensation are all under one roof.
The premiums to finance these benefits are paid exclusively by the employers. In 1993 all industrial employers paid on average DM 1.44 to the BG for every DM 100 wages, or 1.44%. In all, the premiums came to DM 16 billion (US billion used—one thousand million), of which about 80% was spent for rehabilitation and pensions. The remainder was used primarily for prevention programmes.
Occupational Safety and Health Protection
The employer is responsible for the health and safety of the employee at work. The legal scope of this responsibility is set by government in laws and ordinances, and in the protective labour regulations of the industrial BGs, which complete and concretize governmental protective labour law for each branch of industry. The system of prevention of the BGs is notable for its orientation to actual practice, its constant adaptation to the needs of the industry and to the state of technology, as well as for its effective support of the employer and the employee.
The BGs’ tasks of prevention, which are primarily carried out by the Technical Inspection Service (TAD) of the BG and the Occupational Medical Service (AMD), include:
- advising and motivating the employer
- supervising industrial occupational protective measures
- occupational medical care
- informing and training company staff
- safety checking on appliances and equipment
- initiating, carrying out and financing research.
Responsibility for implementing industrial occupational protection lies with the employer, who is legally obliged to hire appropriately qualified personnel to assist in occupational protection. These are specialists in work safety (safety officers, safety technicians and safety engineers) and company doctors. In companies with more than 20 employees, one or more safety representatives must be hired. The scope of the responsibility of the company for occupational safety specialists and company doctors is set by trade association regulations that are specific to the branch of industry and degree of hazard. In companies where an occupational safety specialist or a company doctor is employed, the employer must organize an occupational safety committee, made up of one company representative, two workers’ representatives, the company doctor, and occupational safety specialists and safety representatives. First-aid personnel, whose training is directed by the BG, also belong to the company occupational safety organization.
Occupational medical care has a special significance. Every employee who is at risk for a specific type of health threat at the workplace is examined in a uniform manner, and the results of the examination are assessed according to stated guidelines. In 1993 approximately four million occupational preventive medical examinations were carried out by specially authorized doctors. Lasting health concerns were ascertained in less than 1% of the examinations.
Employees who work with hazardous/carcinogenic materials also have a right to be medically examined even after the hazardous activity has been completed. The BGs have established services to be able to examine these employees. There are now three such services:
- Organizational Service for On-going Examinations (ODIN)
- Central Registration Service for Asbestos Dust-Endangered Employees (ZAs)
- Wismut Central Care Office (ZeBWis).
The three services cared for approximately 600,000 people in 1993. Collecting examination data assists in individual care and also helps improve scientific research for early detection of cancer cases.
Statistics on Workplace Accidents
Goal. The primary goal of collecting statistics on workplace accidents is to improve workplace safety by assessing and interpreting data on accident occurrences. These data are compiled from reports on workplace accidents; 5% to 10% of the accidents (approximately 100,000 accidents) are investigated each year by the Technical Inspection Services of the BGs.
Employers’ reporting responsibility. Every employer is obliged to report a workplace accident to his responsible BG within three days if the accident results in an incapacity to work for three calendar days or causes the death of the insured (“legally reportable workplace accident”). This includes accidents going to or from work. Accidents that cause only property damage or prevent the injured person from working for less than three days do not have to be reported. For reportable workplace accidents, a form “Accident Notification” (figure 1) is submitted by the employer. The time away from work is the significant factor for reporting purposes, regardless of the seriousness of the injury. Accidents that appear harmless must be reported if the injured person cannot work for longer than three days. This three-day requirement facilitates pursuing later claims. Failure to file an accident report, or filing one late, constitutes a violation of regulations that can be punished by the BG with a monetary fine of up to DM 5,000.
Figure 1. An example of an accident notification form

Notification by the attending physician. To optimize medical rehabilitation and to determine how long the employee is unable to work, the injured person receives treatment from a medical specialist selected for this work. The doctor is paid by the responsible industrial BG. Thus, the BG also receives notification of reportable workplace injuries from the doctor if the employer has failed to (promptly) file an accident report. The BG can then request the employer to file a workplace accident notification. This dual reporting system (employer and doctor) assures the BG of receiving knowledge of practically all reportable workplace accidents.
Using the information on the accident notification report and the medical report, the BG checks whether the accident is, in the legal sense, a workplace accident within its jurisdictional competence. On the basis of the medical diagnosis, the BG can, if needed, proceed immediately to ensuring optimal treatment.
A correct and complete description of the circumstances of the accident is especially important for prevention. This enables the BG’s Technical Inspection Service to draw conclusions about defective machinery and equipment that require immediate action to avoid further similar accidents. In the case of serious or fatal workplace accidents, regulations require the employer to immediately notify the BG. These occurrences are immediately investigated by the BG’s occupational safety experts.
In calculating a company’s premium, the BG takes into account the number and cost of workplace accidents that have taken place at this company. A bonus/malus procedure set by law is used in the calculation, and a portion of the company’s premium is determined by the company’s accident trend. This can lead to a higher or lower premium, thus creating financial incentives for employers to maintain safe workplaces.
Collaboration of the employees’ representatives and the safety representatives. Any accident report must also be signed by the workers’ council (Betriebsrat) and by the safety representatives (if these exist). The purpose of this rule is to inform the workers’ council and the safety representatives of the company’s overall accident situation, so that they can effectively exercise their collaborative rights in questions of workplace safety.
Compiling workplace accident statistics. On the basis of the information that the BG receives on a workplace accident from the accident report and the doctor’s report, the accounts are translated into statistical code numbers. The coding covers three areas, among others:
- description of the injured (age, sex, job)
- description of the injury (location of injury, type of injury)
- description of the accident (location, object causing the accident and circumstances of the accident).
Coding is performed by highly trained data specialists who are familiar with the organization of BG industries, utilizing a list of accident and injury codes which contains over 10,000 entries. In order to achieve the highest quality statistics, the classifications are regularly reworked, in order, for example, to adapt them to new technological developments. Furthermore, coding personnel are periodically retrained, and the data are subject to formal-logical and content-sensitive tests.
Uses of workplace accident statistics
An important task of these statistics is to describe the circumstances of the accident at the workplace. Table 1 portrays trends in reportable workplace accidents, new accident pension cases and fatal workplace accidents between 1981 and 1993. Column 3 (“New pension cases”) shows cases for which, because of the seriousness of the accident, a pension payment was first made by the industrial BGs in the given year.
Table 1. Occurrences of workplace accidents, Germany, 1981-93
|
Year |
Workplace accidents |
||
|
Reportable accidents |
New pension cases |
Deaths |
|
|
1981 |
1,397,976 |
40,056 |
1,689 |
|
1982 |
1,228,317 |
39,478 |
1,492 |
|
1983 |
1,144,814 |
35,119 |
1,406 |
|
1984 |
1,153,321 |
34,749 |
1,319 |
|
1985 |
1,166,468 |
34,431 |
1,204 |
|
1986 |
1,212,064 |
33,737 |
1,069 |
|
1987 |
1,211,517 |
32,537 |
1,057 |
|
1988 |
1,234,634 |
32,256 |
1,130 |
|
1989 |
1,262,374 |
30,840 |
1,098 |
|
1990 |
1,331,395 |
30,142 |
1,086 |
|
1991 |
1,587,177 |
30,612 |
1,062 |
|
1992 |
1,622,732 |
32,932 |
1,310 |
|
1993 |
1,510,745 |
35,553 |
1,414 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
To judge the average accident risk of an insured, the number of workplace accidents is divided by the actual time worked, to produce an accident rate. The rate per one million hours worked is used for comparison internationally and across years. Figure 2 shows how this rate varied between 1981 and 1993.
Figure 2. Frequency of workplace accidents

Industry-specific accident statistics. In addition to describing general trends, workplace statistics can be broken down by industry. For example, one might ask, “How many workplace accidents with portable grinders in the metalworking trade were there in the last few years; how and where did they take place; and what injuries resulted?” Such analyses may be useful to many people and institutions, such as government ministries, supervisory officials, research institutes, universities, businesses and workplace safety experts (table 2).
Table 2. Workplace accidents with portable grinders in metalworking, Germany, 1984-93
|
Year |
Reportable accidents |
New accident pensions |
|
1984 |
9,709 |
79 |
|
1985 |
10,560 |
62 |
|
1986 |
11,505 |
76 |
|
1987 |
11,852 |
75 |
|
1988 |
12,436 |
79 |
|
1989 |
12,895 |
76 |
|
1990 |
12,971 |
78 |
|
1991 |
19,511 |
70 |
|
1992 |
17,180 |
54 |
|
1993 |
17,890 |
70 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
For example, table 2 shows that reportable workplace accidents with portable grinders in metalworking rose continuously from the middle of the 1980s to 1990. From 1990 to 1991 a considerable increase in the accident figures is to be noted. This is an artefact resulting from the inclusion, beginning in 1991, of figures encompassing the new borders of reunited Germany. (The earlier figures cover only the Federal Republic of Germany.)
Other data compiled from accident reports reveal that not all accidents with metalworking portable grinders take place primarily in companies in the metalworking industry. Portable grinders, which of course are often used as angle grinders to cut pipes, iron bars and other objects, are frequently employed on construction sites. Accordingly, nearly one-third of the accidents are concentrated in companies in the construction industry. Working with portable grinders in metalworking results mainly in head and hand injuries. The most common head injuries affect the eyes and the area surrounding the eyes, which are injured by broken pieces, splinters and flying sparks. The tool has a fast-spinning grinding wheel, and hand injuries result when the person using the portable machine loses control of it. The high number of eye injuries proves that the importance and obligation of wearing safety glasses while grinding metal with this portable machine must be emphasized within companies.
Comparison of accident rates within and between industries. Although in 1993 there were nearly 18,000 workplace accidents with portable grinders in metalworking, compared to only 2,800 workplace accidents with hand-held power saws in woodworking, one cannot automatically conclude that this machinery poses a greater risk to metalworkers. To assess accident risk for specific industries, the number of accidents must first be related to a measure of exposure to danger, such as hours worked (see “Risk analysis of nonfatal workplace injuries and illnesses” [REC05AE]). However, this information is not always available. Therefore, a surrogate rate is derived as the proportion which serious accidents make of all reportable accidents. Comparing the serious-injury proportions for portable grinders in metalworking and portable circular saws in woodworking demonstrates that portable circular saws have an accident seriousness rate ten times higher than portable grinders. For prioritizing workplace safety measures, this is an important finding. This type of comparative risk analysis is an important component of an overall industrial accident prevention strategy.
Occupational Disease Statistics
Definition and reporting
In Germany an occupational disease is legally defined as a disease whose cause can be traced to the occupational activity of the affected person. An official list of occupational diseases exists. Therefore, assessing whether a sickness constitutes an occupational disease is both a medical and legal question and is referred by public law to the BG. If an occupational disease is suspected, it is not sufficient to prove that the employee suffers from, for example, an eczema. Additional knowledge is required about substances used at work and their potential for harming the skin.
Compiling occupational disease statistics. Because the BGs are responsible for compensating workers with occupational diseases as well as for providing rehabilitation and prevention, they have a considerable interest in application of statistics derived from occupational disease reports. These applications include targeting preventive measures on the basis of identified high-risk industries and occupations, and also providing their findings to the public, the scientific community and political authorities.
To support these activities, the BGs introduced in 1975 a set of occupational disease statistics, which contain data on every occupational disease report and its final determination—whether recognized or denied—including the reasons for the decision at the level of the individual case. This data base contains anonymous data on:
- the person, such as sex, year of birth, nationality
- diagnosis
- hazardous exposures
- the legal decision, including outcome of claim, determination of disability and any further actions taken by the BGs.
Results of the occupational disease statistics. An important function of the occupational disease statistics is to track the occurrence of occupational diseases over time. Table 3 charts the notifications of suspected occupational disease, the number of recognized occupational disease cases overall and the payment of pensions, as well as the number of fatal cases between 1980 and 1993. It should be cautioned that these data are not easy to interpret, since definitions and criteria differ widely. Furthermore, during this time period the number of officially designated occupational diseases rose from 55 to 64. Also, the figures from 1991 encompass the new borders of reunited Germany, whereas the earlier ones cover the Federal Republic of Germany alone.
Table 3. Occurrences of occupational disease, Germany, 1980-93
|
Year |
Notifications |
Recognized occupational disease cases |
Of those with |
Occupational disease fatalities |
|
1980 |
40,866 |
12,046 |
5,613 |
1,932 |
|
1981 |
38,303 |
12,187 |
5,460 |
1,788 |
|
1982 |
33,137 |
11,522 |
4,951 |
1,783 |
|
1983 |
30,716 |
9,934 |
4,229 |
1,557 |
|
1984 |
31,235 |
8,195 |
3,805 |
1,558 |
|
1985 |
32,844 |
6,869 |
3,439 |
1,299 |
|
1986 |
39,706 |
7,317 |
3,317 |
1,548 |
|
1987 |
42,625 |
7,275 |
3,321 |
1,455 |
|
1988 |
46,280 |
7,367 |
3,660 |
1,363 |
|
1989 |
48,975 |
9,051 |
3,941 |
1,281 |
|
1990 |
51,105 |
9,363 |
4,008 |
1,391 |
|
1991 |
61,156 |
10,479 |
4,570 |
1,317 |
|
1992 |
73,568 |
12,227 |
5,201 |
1,570 |
|
1993 |
92,058 |
17,833 |
5,668 |
2,040 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
Example: infectious diseases. Table 4 shows the decline in the number of recognized cases of infectious diseases during the period 1980 to 1993. It specifically singles out viral hepatitis, for which one can clearly see that a strongly declining trend developed from approximately the mid-1980s in Germany, when employees at risk in the health service were given preventive inoculations. Thus occupational disease statistics can serve not only to find high rates of illnesses, but can also document the successes of protective measures. Declines in disease rates may of course have other explanations. In Germany, for example, the reduction in the number of cases of silicosis during the past two decades is chiefly a result of the decline in the number of jobs in mining.
Table 4. Infectious diseases recognized as occupational diseases, Germany, 1980-93
|
Year |
Total recognized cases |
Of those: hepatitis viral |
|
1980 |
1173 |
857 |
|
1981 |
883 |
736 |
|
1982 |
786 |
663 |
|
1983 |
891 |
717 |
|
1984 |
678 |
519 |
|
1985 |
417 |
320 |
|
1986 |
376 |
281 |
|
1987 |
224 |
152 |
|
1988 |
319 |
173 |
|
1989 |
303 |
185 |
|
1990 |
269 |
126 |
|
1991 |
224 |
121 |
|
1992 |
282 |
128 |
|
1993 |
319 |
149 |
Source: Central Federation of Berufsgenossenschaften (HVBG), Germany.
Sources of Information
The HVBG, as umbrella organization for the BGs, centralizes the common statistics and produces analyses and brochures. Furthermore, the HVBG sees statistical information as an aspect of the overall information that must be available to carry out the broad range of mandated responsibilities of the accident insurance system. For this reason, the Central Information System of the BGs (ZIGUV) was formed in 1978. It prepares relevant literature and makes it available to the BGs.
Workplace safety as an interdisciplinary, comprehensive approach requires optimum access to information. The BGs in Germany have resolutely taken this path and thereby made a considerable contribution to the efficient workplace safety system in Germany.
Risk Analysis of Nonfatal Workplace Injuries and Illnesses
The United States Bureau of Labor Statistics routinely classifies nonfatal workplace injuries and illnesses by worker and case characteristics, using data from the US Survey of Occupational Injuries and Illnesses. While these counts identify groups of workers who experience large numbers of workplace injuries, they do not measure risk. Thus a particular group may sustain many workplace injuries simply because of the large number of workers in that group, and not because the jobs performed are especially hazardous.
In order to quantify actual risk, data on workplace injuries must be related to a measure of exposure to risk, such as number of hours worked, a labour supply measure which may be available from other surveys. The rate of nonfatal workplace injuries for a group of workers may be calculated by dividing the number of injuries recorded for that group by the number of hours worked during the same time period. The rate obtained this way represents the risk of injury per hour of work:
![]()
A convenient way of comparing the risk of injury among various groups of workers is to compute the relative risk:
![]()
The reference group may be a special group of workers, such as all managerial and professional specialty workers. Alternatively, it might consist of all workers. In any case, the relative risk (RR) corresponds to the rate ratio commonly used in epidemiological studies (Rothman 1986). It is algebraically equivalent to the percentage of all injuries which occur to the special group divided by the percentage of hours accounted for by the special group. When the RR is greater than 1.0, it indicates that members of the selected group are more likely to sustain injuries than members of the reference group; when the RR is less than 1.0, it indicates that, on the average, members of this group experience fewer injuries per hour.
The following tables show how indexes of relative risk for different groups of workers can identify those at greatest risk of workplace injury. The injury data are from the 1993 Survey of Occupational Injuries and Illnesses (BLS 1993b) and measure the number of injuries and illnesses with days away from work. The calculation relies upon estimates of annual hours worked taken from the microdata files of the US Bureau of the Census Current Population Surveys for 1993, which is obtained from household surveys (Bureau of the Census 1993).
Table 1 presents data by occupation on the share of workplace injuries, the share of hours worked and their ratio, which is the RR for injuries and illnesses with days away from work. The reference group is taken to be “All nonfarm private industry occupations” with workers of age 15 and older, which comprises 100%. As an example, the group “Operators, fabricators and labourers” experienced 41.64% of all injuries and illnesses, but contributed only 18.37% of the total hours worked by the reference population. Therefore, the RR for “Operators, fabricators and labourers” is 41.64/18.37 = 2.3. In other words, workers in this group of occupations have on average 2.3 times the injury/illness rate of all nonfarm private industry workers combined. Furthermore, they are about 11 times as likely to sustain a serious injury as employees in a managerial or professional specialty.
Table 1. Risk of occupational injuries and illnesses
|
Occupation |
Percentage1 |
Index |
|
|
Injury and illness cases |
Hours worked |
||
|
All nonfarm private industry occupations |
100.00 |
100.00 |
1.0 |
|
Managerial and professional specialty |
5.59 |
24.27 |
0.2 |
|
Executive, administrative and managerial |
2.48 |
13.64 |
0.2 |
|
Professional specialty |
3.12 |
10.62 |
0.3 |
|
Technical, sales and administrative support |
15.58 |
32.19 |
0.5 |
|
Technicians and related support |
2.72 |
3.84 |
0.7 |
|
Sales occupations |
5.98 |
13.10 |
0.5 |
|
Administrative support, including clerical |
6.87 |
15.24 |
0.5 |
|
Service occupations2 |
18.73 |
11.22 |
1.7 |
|
Protective service3 |
0.76 |
0.76 |
1.0 |
|
Service occupations, except protective service |
17.97 |
10.46 |
1.7 |
|
Farming, forestry and fishing occupations4 |
1.90 |
0.92 |
2.1 |
|
Precision production, craft and repair |
16.55 |
13.03 |
1.3 |
|
Mechanics and repairers |
6.30 |
4.54 |
1.4 |
|
Construction trades |
6.00 |
4.05 |
1.5 |
|
Extractive occupations |
0.32 |
0.20 |
1.6 |
|
Precision production occupations |
3.93 |
4.24 |
0.9 |
|
Operators, fabricators and labourers |
41.64 |
18.37 |
2.3 |
|
Machine operators, assemblers and inspectors |
15.32 |
8.62 |
1.8 |
|
Transportation and material moving occupations |
9.90 |
5.16 |
1.9 |
|
Handlers, equipment cleaners, helpers and laborers |
16.42 |
4.59 |
3.6 |
1 Percentage of injuries and illnesses, hours worked and index of relative risk for occupational injuries and illnesses with days away from work, by occupation, US nonfarm private industry employees 15 years and over, 1993.
2 Excludes private household workers and protective service workers in the public sector
3 Excludes protective service workers in the public sector
4 Excludes workers in agricultural production industries
Sources: BLS Survey of Occupational Injuries and Illnesses, 1993; Current Population Survey, 1993.
The various occupational groups may be ranked according to degree of risk simply by comparing their RR indices. The highest RR in the table (3.6) is associated with “handlers, equipment cleaners, helpers and labourers”, while the group at lowest risk is managerial and professional specialty workers (RR = 0.2). More refined interpretations may be made. While the table suggests that workers with lower levels of skills are in jobs with higher risks of injury and illness, even among blue-collar occupations the injury and illness rate is higher for less-skilled operators, fabricators and labourers compared to precision production, craft and repair workers.
In the above discussion, the RRs have been based upon all injuries and illnesses with days away from work, since these data have long been readily available and understood. Using the extensive and newly developed coding structure of the Survey of Occupational Injuries and Illnesses, researchers may now examine specific injuries and illnesses in detail.
As an example, table 2 shows the RR for the same set of occupation groupings, but restricted to the single outcome “Repetitive Motion Conditions” (event code 23) with days away from work, by occupation and gender. Repetitive motion conditions include carpal tunnel syndrome, tendonitis and certain strains and sprains. The group most severely affected by this type of injury is quite clearly female machine operators, assemblers and inspectors (RR = 7.3), followed by female handlers, equipment cleaners, helpers and labourers (RR = 7.1).
Table 2. Index of relative risk for repetitive motion conditions with days away from work, by occupation and gender, US nonfarm private industry employees 15 years and over, 1993
|
Occupation |
All |
Men |
Women |
|
All nonfarm private industry occupations |
1.0 |
0.6 |
1.5 |
|
Managerial and professional specialty |
0.2 |
0.1 |
0.3 |
|
Executive, administrative and managerial |
0.2 |
0.0 |
0.3 |
|
Professional specialty |
0.2 |
0.1 |
0.3 |
|
Technical, sales and administrative support |
0.8 |
0.3 |
1.1 |
|
Technicians and related support |
0.6 |
0.3 |
0.8 |
|
Sales occupations |
0.3 |
0.1 |
0.6 |
|
Administrative support, including clerical |
1.2 |
0.7 |
1.4 |
|
Service occupations1 |
0.7 |
0.3 |
0.9 |
|
Protective service2 |
0.1 |
0.1 |
0.4 |
|
Service occupations, except protective service |
0.7 |
0.4 |
0.9 |
|
Farming, forestry and fishing occupations3 |
0.8 |
0.6 |
1.8 |
|
Precision production, craft and repair |
1.0 |
0.7 |
4.2 |
|
Mechanics and repairers |
0.7 |
0.6 |
2.4 |
|
Construction trades |
0.6 |
0.6 |
— |
|
Extractive occupations |
0.1 |
0.1 |
— |
|
Precision production occupations |
1.8 |
1.0 |
4.6 |
|
Operators, fabricators and laborers |
2.7 |
1.4 |
6.9 |
|
Machine operators, assemblers and inspectors |
4.1 |
2.3 |
7.3 |
|
Transportation and material moving occupations |
0.5 |
0.5 |
1.6 |
|
Handlers, equipment cleaners, helpers and laborers |
2.4 |
1.4 |
7.1 |
1 Excludes private household workers and protective service workers in the public sector
2 Excludes protective service workers in the public sector
3 Excludes workers in agricultural production industries
Note: Long dashes — indicate that data do not meet publication guidelines.
Source: Calculated from the BLS Survey of Occupational Injuries and Illnesses, 1993, and Current Population Survey, 1993.
The table shows striking differences in the risk of repetitive motion conditions that depend on the gender of the worker. Overall, a woman is 2.5 times as likely as a man to lose work due to repetitive motion illness (2.5 = 1.5/0.6). However, this difference does not simply reflect a difference in the occupations of men and women. Women are at higher risk in all of the major occupational groups, as well as the less aggregated occupational groupings reported in the table. Their risk relative to men is especially high in sales and blue-collar occupations. Women are six times as likely as men to lose work time from repetitive motion injuries in sales and in precision production, craft and repair occupations.
Musicians
The musician relies on the skilled use of the muscles, nerves and bones (neuromusculoskeletal system). Playing an instrument requires finely controlled repetitive motions and often entails working in unnatural postures for extended periods of practice and performance (figure 1). These demands on the body can result in specific types of health problems. In addition, adverse working conditions, such as excessive sound exposure levels, prolonged periods of performance without rest, and inadequate preparation for new and difficult repertoire or instruments may affect the health of musicians in all age groups and at all levels of performing ability. Recognition of these hazards, accurate diagnosis and early treatment will prevent occupational disabilities that may interfere with, interrupt or end careers.
Figure 1. Orchestra.

Neuromusculoskeletal Problems
Studies from the United States, Australia and Canada suggest that around 60% of musicians will face career-threatening injuries during their working lifetime. Clinical cross-sectional studies have examined the prevalence of muscle-tendon disorders, of peripheral nerve entrapment syndromes and motor control problems. These studies have revealed several common diagnoses, which include various overuse syndromes, including strain of the muscles and connective tissue which control the bending and extending motions in the wrist and fingers. These syndromes result from the repetitive forceful movement of the muscle-tendon units. Other common diagnoses relate to pain in body parts which are involved in prolonged strain from awkward and imbalanced postures while playing musical instruments. Playing the instruments in the groups described below involves putting pressure on the branches of the nerves in the wrist and forearm, the shoulders, arm and neck. Occupational cramp or muscle spasms (focal dystonia) are also common problems which often can affect performers at the pinnacle of their careers.
String instruments: Violin, viola, cello, bass, harp, classical guitar and electric guitar
Health problems in musicians who play string instruments often are caused by the manner in which the musician supports the instrument and the posture assumed while sitting or standing and playing. For example, most violinists and violists support their instruments between the left shoulder and chin. Often the musician’s left shoulder will be elevated and the left chin and jaw will bear down in order to allow the left hand to move over the fingerboard. Elevating a joint and bearing down at the same time leads to a state of static contraction which promotes neck and shoulder pain, temporomandibular joint disorders involving the nerves and muscles of the jaw, and thoracic outlet syndrome, which can include pain or numbness in the neck, shoulder and upper chest area. Prolonged static sitting postures, particularly while assuming a bent posture, promote pain in the large muscle groups which support posture. Static twisting rotation of the spine is often required to play the string bass, harp and classical guitar. Heavy electric guitars are usually supported by a strap over the left neck and shoulder, contributing to pressure on the nerves of the shoulder and upper arm (the brachial plexus) and thus to pain. These problems of posture and support contribute to the development of strain and pressure of the nerves and muscles of the wrist and fingers by promoting their faulty alignment. For example, the left wrist may be used for excessive repetitive bending motions which result in strain of the extensor muscles of the wrist and fingers and the development of carpal tunnel syndrome. Pressure on the nerves of the shoulder and arm (lower trunks of the brachial plexus) may contribute to problems with the elbow, such as a double crush syndrome and ulnar neuropathy.
Keyboard instruments: Piano, harpsichord, organ, synthesizers and electronic keyboards
Playing a keyboard instrument requires assuming a similar posture to that of typing. Often the forward and downward orientation of the head to look at the keys and hands and repetitive upward movement to look at the music causes pain in the nerves and muscles of the neck and back. The shoulders will often be rounded, combined with a forward head poking posture and a shallow breathing pattern. A condition known as thoracic outlet syndrome can develop from chronic compression of the nerves and blood vessels that pass between the muscles in the neck, shoulder and rib cage. In addition, a musician’s tendency to bend the wrists and curl the fingers while keeping the hand/finger joints flat places excessive strain on the wrist and finger muscles in the forearm. Additionally, the repeated use of the thumb kept in a position under the hand strains the thumb muscles which extend and binds the finger extensor muscles across the back of the hand. The high repetitive force needed to play large chords or octaves may strain the capsule of the wrist joint and result in ganglion formation. Prolonged co-contraction of the muscles that turn and move the arms up and down can lead to nerve entrapment syndromes. Muscle spasms and cramps (focal dystonia) are common among this group of instrumentalists, sometimes requiring long periods of neuromuscular retraining to correct movement patterns which can lead to these difficulties.
Wind and brass instruments: Flute, clarinet, oboe, saxophone, bassoon, trumpet, french horn, trombone, tuba and bagpipes
A musician who plays one of these instruments will vary his or her posture according to the need to control airflow since posture will control the area from which diaphragmatic and intercostal breath is drawn. Playing these instruments depends on the way the mouthpiece is held (the embouchure) which is controlled by the facial and pharyngeal muscles. The embouchure controls sound production of vibrating reeds or the mouthpiece. Posture also affects how the musician supports the instrument while sitting or standing and in operating the keys or valves of the instrument that govern the pitch of the note played by the fingers. For example, the traditional French open-holed flute requires sustained adduction and flexion (bending forward) of the left shoulder, sustained abduction (drawing away) of the right shoulder and rotation of the head and neck to the left in slight movement. The left wrist is often held in an extremely bent position while the hand is also extended in order to support the instrument by the curled left index finger and both thumbs, counter balanced by the right little finger. This promotes strain of the forearm muscles and the muscles which permit extension of the fingers and thumbs. The tendency to project the head and neck forward and use shallow breathing increases the chances of developing thoracic outlet syndrome.
Percussion instruments: Drums, timpani, cymbals, xylophone, marimba, tabla and taiko
The use of sticks, mallets and bare hands to strike various percussion instruments results in rapid pulling back of the wrists and fingers at impact. The impulse vibration caused by striking the instrument is transmitted up the hand and arm and contributes to repetitive strain injuries of the muscle-tendon units and the peripheral nerves. Biomechanical factors, such as the amount of force used, the repetitive nature of the playing and static load placed on the muscles can add to the injuries. Carpal tunnel syndrome and nodule formation in tendon sheaths are common in this group of musicians.
Hearing Loss
The risk of hearing loss from music exposure depends on the intensity and duration of exposure. It is not uncommon to have exposure levels of 100 dB during a quiet passage of orchestral music, with peak values of 126 dB measured at the shoulder of an instrumentalist in the middle of the orchestra. At the position of the conductor or teacher, levels of 110 dB in an orchestra or band are common. Exposure levels for pop/rock and jazz musicians may be significantly higher, depending on the physical acoustics of the stage or pit, amplification system and placement of speakers or other instruments. The average duration of exposure may be approximately 40 hours per week, but many professional musicians will perform 60 to 80 hours per week on occasion. Hearing loss among musicians is far more common than expected, with approximately 89% of professional musicians who were found to have suffered musculoskeletal injuries also showing an abnormal hearing test result, with a hearing loss in the 3 to 6 KHz region.
Personal ear protection can be used but it must be adapted for each instrument type (Chasin and Chong 1992). By inserting an acoustic attenuator or filter into custom-moulded earplugs, the intensity of higher frequency sounds transmitted by ordinary earplugs is reduced to a flat attenuation as measured at the eardrum, which should be less damaging to the ear. The use of a tuned or adjustable vent in a custom earplug will allow the lower frequencies and some harmonic energy to pass through the earplug unattenuated. Earplugs can be designed to provide a slight amplification to alter perception of the singer’s voice, thus allowing the artist to reduce the risk of vocal strain. Depending on the psycho-acoustical nature of the instrument and surrounding music exposures, substantial reduction in risk for the development of hearing loss can be obtained. Improvement in the perception of the relative intensity of the musician’s own performance may reduce the risk of repetitive strain injuries by a relative reduction of the force of repetitive movements.
There are practical strategies for reducing the exposure of musicians that do not interfere with music production (Chasin and Chong 1995). Loudspeaker enclosures can be elevated above floor level, which results in minimal loss of low-frequency sound energy, while preserving sufficient loudness for the musician to perform at a lower intensity level. Musicians who play high-intensity, highly directional instruments such as trumpets and trombones should be on risers so that the sound passes above the other musicians, thereby lowering its impact. There should be 2 m of unobstructed floor space in front of the orchestra. Small stringed instruments should always have at least 2 m of unobstructed space above them.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."