Generally speaking, the term accident is used to denote events resulting in undesired or unplanned physical injury or damage; an accident model is a conceptual scheme applied to the analysis of such events. (Some models may explicitly declare that “near accidents”—sometimes known as “near misses”—are covered by the model; however, the distinction is not important to this article.) Models of accidents can serve different purposes. First, they may provide a conceptual understanding of how accidents occur. Second, models may be used to record and store information on accidents. Third, they may provide a mechanism for investigating accidents. These three aims are not entirely distinct, but form a useful means of categorization.
This article describes MAIM, the Merseyside Accident Information Model, which is most naturally adapted to the second purpose—recording and storing accident information. Following an outline of the rationale for MAIM, some early studies evaluating the model are described. The article ends with recent progress with MAIM, including the use of “intelligent software” to collect and analyse information on injury accidents.
Early Accident Modelling
In Heinrich’s model (1931), the causal sequence leading to an accident was likened to a sequence of five falling dominoes, each of the first four being necessary before the final event could occur. In a precursor to MAIM, Manning (1971) concluded that “the basic requirements of an accidental injury are the presence of a host [a worker, for example] and an environmental object which contributes to the accident. The host or the object or both move in relation to each other.” Kjellén and Larsson (1981) developed their own model, which posited two levels: the accident sequence and the underlying, determining factors. In a later paper, Kjellén and Hovden (1993) described subsequent progress in the context of other literature and noted the need for “efficient use of existing information from routine accident and near accident reports by means of a powerful information retrieval system”. This has been achieved for MAIM.
Rationale for MAIM
There appears to be a substantial consensus that useful information on accidents should not merely concentrate on the immediate circumstances of the damage or injury, but should also include an understanding of the preceding chain of events and factors causing the accident sequence to occur. Some early classification systems failed to achieve this. Understanding objects, movements (of people or objects) and events were commonly mixed and successive events were not distinguished.
A simple example illustrates the problem. A worker slips on a patch of oil, falls and strikes his or her head on a machine and suffers a concussion. We can easily distinguish the (immediate) cause of the accident (slipping on oil) and the cause of the injury (hitting the head on the machine). Some classification systems, however, include the categories “falls of persons” and “striking against objects”. The accident could be allocated to either of these, although neither describes even the immediate cause of the accident (slipping on oil) or causal factors (such as how did the oil get on the floor).
Essentially, the problem is that just one factor is considered in a multifactorial situation. An accident does not always consist of a single event; there may be many. These points formed the basis for the development of MAIM by Derek Manning, an occupational physician.
Description of MAIM
The centrepiece of the accident is the first unforeseen (undesired or unplanned) event involving the damaged equipment or injured person (figure 1). This will not always be the first event in the accident process described as a preceding event. In the example above, the slip counts as the first unforeseen event of the accident. (Given the presence of oil patches on the floor, it is not unforeseen that someone will slip on one and fall, but the person walking does not foresee this.)
Figure 1. The MAIM Accident Model
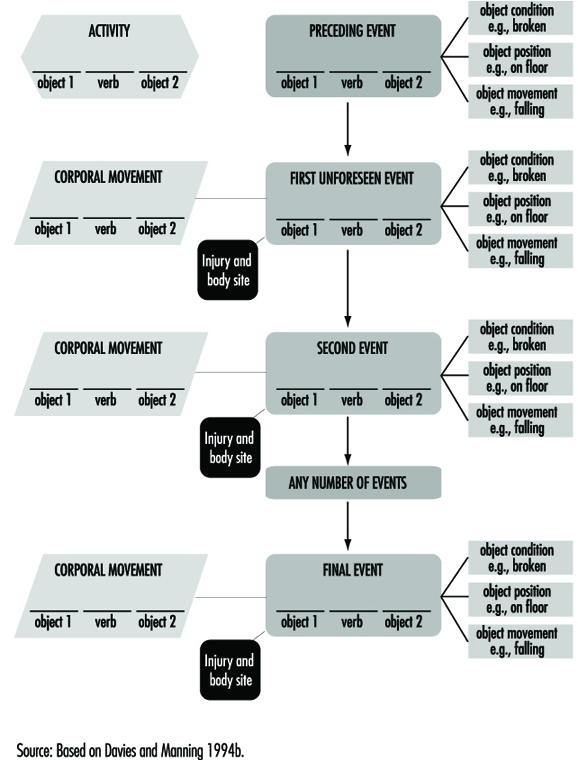
The behaviour of the equipment or person is described by the general activity at the time and a more specific description of the type of corporal movement when the first event occurred. Objects involved are described, and for those related to events, characteristics of objects include position, movement and condition. On occasion, a second object which inter-relates with the first object may be involved (for example, striking a chisel with a hammer).
As noted above, there may be more than one event and the second event may also have an object (perhaps different) involved in it. Additionally, the equipment or person may make an additional corporal movement, such as throwing out a hand to prevent or break a fall. These can be included in the model. A third fourth or later event may occur before the sequence finally leads to an injury. The model can be expanded in all directions by recording factors related to each component. For example, branches from activities and corporal movements would record psychological factors, medications or physical limitations of a worker.
In general, separate events may be easily distinguished intuitively, but a stricter definition is useful: an event is an unexpected change, or lack of change, in the energy state of the situation. (The term energy includes both kinetic and potential energy.) The first event is always unexpected. Subsequent events may be expected, even inevitable, after the first event, but are always unexpected before the accident. An example of unexpected lack of change of energy is when a hammer being swung misses the nail at which it is aimed. The example of a worker who slips on a patch of oil, falls and hits his or her head provides an illustration. The first event is “foot slipped”—instead of remaining still, the foot acquires kinetic energy. The second event is “fell”, when further kinetic energy is acquired. This energy is absorbed by the collision of the worker’s head with the machine when the injury occurs and the sequence ends. This can be “plotted” onto the model as follows:
- 1st event: foot slipped on oil.
- 2nd event: person fell.
- 3rd event: head struck against machine.
Experience with MAIM
An earlier version of the MAIM model was used in a study of all 2,428 reported accidents in 1973 in a gearbox manufacturing plant on the grounds of an automobile company. (See Shannon 1978 for further details.) The operations included cutting and grinding of gears, heat treatment and gearbox assembly. The cutting process produced sharp metal splinters and shavings, and oil was used as a coolant. Purpose-designed forms were used to collect information. Each accident was plotted independently onto the model by two people and discrepancies were resolved by discussion. For each accident, the components were given numerical codes, so the data could be stored on a computer and analyses performed. The following outlines some basic results and presents an examination made what was learned specifically from the use of the model.
The accident rate was substantially reduced (by nearly 40%), apparently as a result of the study being conducted. The researchers learned that because of the additional questioning that the study called for (and the consequent time involved) many employees “could not be bothered” to report minor injuries. Several items of evidence confirmed this:
- The rate rose again in 1975 after the study ended.
- The rate of lost-time injuries was unaffected.
- Visits to the medical centre for non-industrial complaints were unaffected.
- Accident rates on the rest of the grounds were unaffected.
Thus the reduced rate did indeed appear to be an artefact of reporting.
Another interesting finding was that there were 217 injuries (8%) for which the workers involved could not be certain how or when they occurred. This was discovered because workers were explicitly asked if they were sure of what happened. Typically, the injuries involved were cuts or splinters, relatively common given the nature of work at this plant.
Of the remaining accidents, nearly half (1,102) consisted of just one event. Two- and three-event accidents were successively less common, and 58 accidents involved four or more events. There was a marked increase in the proportion of accidents resulting in lost time with an increase in the number of events. One possible explanation is that there was an increase in kinetic energy with each event, so that with more events, there was more energy to dissipate when the worker and the object involved collided.
Further examination of differences between lost-time and non-lost-time accidents found very marked differences in the distributions for separate components of the model. For example, when the first event was “person slipped”, nearly a quarter of the accidents resulted in lost time; but for “body punctured by”, only 1% did so. For combinations of components, such differences were accentuated. For example, with respect to the final events and related objects, none of the 132 accidents in which the casualty was “punctured by” or “splintered” resulted in lost time, but when the final event was “strained/sprained” with “no object involved”, 40% of the injuries caused lost time.
These results contradicted the view that the severity of injury is largely a matter of luck and prevention of all types of accidents would lead to a reduction of serious injuries. This means that analysing all accidents and attempting to prevent the most common types would not necessarily have an effect on those causing serious injuries.
A sub-study was conducted to assess the usefulness of information in the model. Several potential uses of accident data were identified:
- to measure safety performance—the extent to which accidents in a plant, or area of a plant, continue to occur over time
- to identify causes
- to identify errors (in the broadest meaning of the term)
- to check on control—that is, to see whether safety measures taken to prevent some type(s) of accident are indeed effective
- to provide a basis of expertise, as knowledge of a wide range of accident situations and circumstances might help provide accident prevention advice.
Three safety officers (practitioners) rated the usefulness of the verbal descriptions and the plotted models for a series of accidents. Each rated at least 75 accidents on a scale from 0 (no useful information) to 5 (perfectly adequate for use). For the majority of accidents, the ratings were identical—that is, no information was lost in the transfer from the written descriptions to the model. Where there was a loss of information it was mostly just one point on the 0 to 5 scale—that is, only a small loss.
The information available, though, was rarely “perfectly adequate”. This was partly because the safety officers were used to conducting detailed on-the-spot investigations, something not done in this study because all reported accidents, both minor and more serious ones, were included. It should be remembered, however, that the information plotted onto the models was taken directly from written descriptions. Since relatively little information was lost, this suggested the possibility of excluding the intermediate step. The more widespread use of personal computers and availability of improved software make automated data collection possible—and allow checklists to be used by way of insuring that all relevant information is obtained. A program has been written for this purpose and has undergone some initial testing.
MAIM Intelligent Software
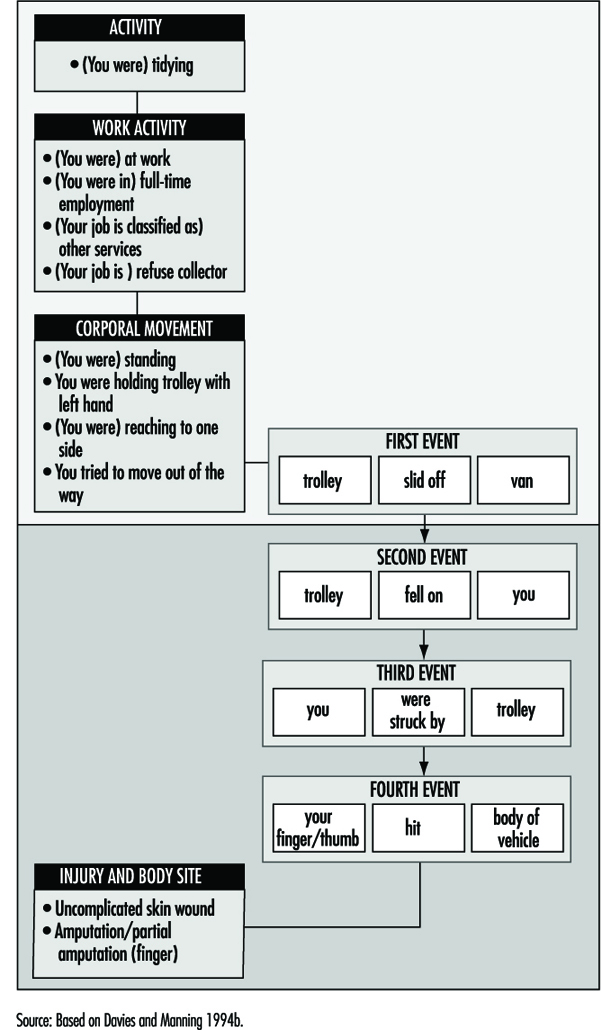
The MAIM model was used by Troup, Davies and Manning (1988) to investigate accidents causing back injuries. A database was created on an IBM PC by coding results from patient interviews conducted by an interviewer who was experienced with the MAIM model. The analysis of interviews to obtain the MAIM description (figure 2 ) was done by the interviewer and it was only at this stage that the data were entered into the database. While the method was quite satisfactory, there were potential problems in making the method generally accessible. In particular, two areas of expertise were required—interviewing skills and the familiarity with the analysis needed to form the MAIM description of the accident.
Figure 2. Accident summary as recorded by patient interview
Software was developed by Davies and Manning (1994a) to conduct a patient interview and produce a database of accidents using the MAIM model. The purpose of the software was to provide two areas of expertise—the interview and the analysis to form the MAIM event structure. The MAIM software is, in effect, an intelligent “front end” to a database, and by 1991 it was sufficiently developed to be tested in a clinical environment. The MAIM software was designed to interact with the patient by means of “menus”—the patient selects options from lists which require only the use of cursor keys and the “Enter” key. The choice of an item from the list of options affected to some extent the path through the interview and also had the effect of recording information at the appropriate part of the MAIM description of the accident. This method of data collection eliminated the need for spelling and typing skills and also gave a repeatable and consistent interview.
The event structure of the MAIM model uses verbs and objects to form simple sentences. Verbs in events can be associated with different accident scenarios, and this property of the model forms the basis for the construction of a set of linked questions that form an interview. Questions are presented in such a way that at any stage only simple choices are needed, effectively breaking the complex account of the accident into a set of simple descriptions. Once an event verb has been identified, associated nouns can be found by locating the objects to form a sentence giving the full detail of the description of the particular event. It is clear that this strategy requires the use of an extensive dictionary of objects which can be searched quickly and efficiently.
The Home Accident Surveillance System (HASS) (Department of Trade and Industry 1987) monitors objects involved in accidents, and the list of objects used by HASS was used as the basis of an object dictionary for the MAIM software and was extended to include objects found in the workplace. Objects can be grouped into classes, and with this structure a hierarchical menu system can be defined—classes of objects form layers that correspond to menu lists. Thus a linked list of associated objects can be used to locate individual items. As an example, the object hammer could be found by selecting, in order: (1) tools, (2) hand tools and (3) hammer from three successive menu lists. A given object could potentially be classified into several different groups—for example, a knife could be associated with kitchen items, tools or sharp objects. This observation was used to create redundant links in the object dictionary, allowing many different paths to find the required object. The object dictionary currently has a vocabulary of about 2,000 entries covering work and leisure environments.
The MAIM interview also collects information on activities at the time of the accident, corporal movements, the location of the accident, contributory factors, injuries and disability. All of these elements can occur more than once in an accident, and this is reflected in the structure of the underlying relational database which was used to record the accident.
At the end of the interview, several sentences describing events in the accident will have been recorded and the patient is asked to put them in the correct order. In addition, the patient is asked to link injuries with the recorded events. A summary of the information collected is then presented on the screen of the computer for information.
An example of an accident summary as seen by the patient is shown in figure 2 . This accident has been superimposed on the MAIM diagram in figure 2 . Details relating to factors and the location of the accident have been omitted.
The first unforeseen or unintended event (first event) involving the injured person is usually the first event in the accident sequence. For example, when a person slips and falls, the slip is normally the first event in the accident sequence. If, on the other hand, a person is injured by a machine because another person operates the machine before the victim is standing clear, the first event involving the victim is “trapped by machine” but the first event in the accident sequence is “other person operated machine prematurely”. In the MAIM software, the first event in the accident sequence is recorded and it may arise either from the first event involving the injured person or as a preceding event (figure 1). Theoretically, this way of viewing matters may be unsatisfactory, but from the accident prevention point of view, it identifies the beginning of the accident sequence, which can then be targeted to prevent similar accidents in the future. (The term action of deviation is used by some authorities to describe the beginning of the accident sequence, but it is not yet clear if this is always synonymous with the first event in the accident.)
When the MAIM software was first used in a clinical setting it was clear that there were problems in correctly appraising some types of “underfoot” accidents. The MAIM model identifies the first unforeseen event as the starting point of the accident sequence. Consider two similar accidents, one in which a worker intentionally steps onto an object which then breaks, and a second accident in which a worker unintentionally steps onto an object which breaks. In the first accident stepping on the object is a body movement and the first unforeseen event is the object breaking. In the second accident stepping on the object is the first unforeseen event in the accident. The resolution of these two scenarios is to ask, “Did you accidentally step on something?” This demonstrates how important the correct design of the interview is in obtaining accurate data. The analysis of these two accidents allows recommendations on accident prevention as follows; the first accident could have been prevented by making the patient aware that the object would break. The second accident could have been prevented by making the patient aware that the object was an underfoot hazard.
The MAIM software has been tested successfully in three clinical settings, including a 1-year project in the Accident and Emergency Department of the Royal Liverpool University Hospital. Patient interviews took between 5 and 15 minutes, and on average two patients were interviewed per hour. In all, 2,500 accidents were recorded. Work on publications based on these data is in progress.