A public health approach to occupational injury prevention is based on the assumption that injury is a health problem, and as such can either be prevented or its consequences mitigated (Occupational Injury Prevention Panel 1992; Smith and Falk 1987; Waller 1985). When a worker falls from a scaffold, the tissue damage, internal haemorrhage, shock and death that follow are, by definition, a disease process—and also by definition a concern for public health professionals. Just as malaria is defined as a disease whose causal agent is a specific protozoan, injuries are a family of diseases caused by exposure to a particular form of energy (kinetic, electrical, thermal, radiation or chemical) (National Committee for Injury Prevention and Control 1989). Drowning, asphyxiation and poisoning are also considered injuries because they represent a relatively rapid departure from the body’s structural or functional norm, as does acute trauma.
As a health problem, injuries are the leading cause of premature death (i.e., before age 65) in most countries (Smith and Falk 1987; Baker et al. 1992; Smith and Barss 1991). In the United States, for example, injury is the third leading cause of death following cardiovascular disease and cancer, the leading cause of hospitalization under the age of 45, and an imposed economic burden of 158 billion dollars in direct and indirect costs in 1985 (Rice et al. 1989). One out of three nonfatal injuries and one out of six fatal injuries to working-aged persons in the United States occur on the job (Baker et al. 1992). Similar patterns apply in most of the developed world (Smith and Barss 1991). In middle- and low-income countries, a rapid and relatively unregulated pace of industrialization may result in a nearly global pandemic of occupational injuries.
Public Health Models for Injury Control
The traditional practice of workplace safety usually focuses on minimizing risks and losses within a single company. Public health practitioners engaged in occupational injury control are interested not only in individual worksites but also in improving the health status of populations in geographic areas that may be exposed to the hazards associated with multiple industries and occupations. Some events such as workplace fatalities may be rare at individual plants, but by studying all fatalities in a community, risk patterns and prevention policy may become evident.
Most models of public health practice are based on three elements: (1) assessment, (2) development of prevention strategies, and (3) evaluation. Public health practice is usually multidisciplinary and founded on the applied science of epidemiology. Epidemiology is the study of the distribution and determinants of diseases and injuries in a population. The three main applications of epidemiology are surveillance, aetiological research and evaluation.
Surveillance is “the ongoing and systematic collection, analysis and interpretation of health data in the process of describing and monitoring a health event. This information is used for planning, implementing and evaluating public health interventions and programs” (CDC 1988).
Aetiological research tests hypotheses regarding the determinants of disease and injuries through the use of controlled, usually observational, studies.
Evaluation in both applied social sciences and epidemiology is “a process that attempts to determine as systematically and objectively as possible the relevance, effectiveness and impact of activities in light of their objectives” (Last 1988). Epidemiological evaluation usually entails the use of controlled study designs to measure the effects of an intervention on the occurrence of health-related events in a population.
The basic model of public health practice is described by a cycle of epidemiological surveillance, research on causes, interventions (targeted to high-risk populations and specific to severe health conditions), and epidemiological evaluation. Important modifications of this model include community-oriented primary care (Tollman 1991), community-based health education and health promotion (Green and Kreuter 1991), community health development (Steckler et al. 1993), participatory action research (Hugentobler, Israel and Schurman 1992) and other forms of community-oriented public health practice that rely on greater participation of communities and labour—as opposed to government officials and industrial management—to define problems, develop solutions and evaluate their effectiveness. Family farming, fishing and hunting, self-employed work, many small business operations and work in the informal economy are all primarily influenced by family and community systems and occur outside the context of an industrial management system. Community-oriented public health practice is a particularly viable approach to occupational injury prevention in these populations.
Outcomes of Interest
The public health approach to workplace safety moves from the concept of accident prevention to a broader approach to injury control where the primary outcomes of interest are both the occurrence and severity of injury. Injury is by definition physical damage due to the transfer of energy. A transfer of mechanical energy can cause trauma, as in the case of a fall or automobile crash. Thermal, chemical, electrical or radiation energy can cause burns and other injuries (Robertson 1992). Not only is the occurrence of injury of interest to public health practitioners, but so is the severity and long-term outcome of injury. Injury severity can be measured in several dimensions, including anatomical (the amount and nature of tissue damage in various regions of the body), physiological (how close to death the patient is, based on vital signs), disability, impairment of quality of life, and indirect and direct costs. Of considerable importance to injury epidemiologists is anatomical severity, often measured by the Abbreviated Injury Score and the Injury Severity Scale (MacKenzie, Steinwachs and Shankar 1989). These measures can predict survival and are a useful indicator of the energy transferred in severe events, but are not sensitive enough to discriminate between severity levels among the relatively less severe, but much more frequent occupational injuries such as sprains and strains.
Among the least useful, but most common measures of severity is days lost from work following injury. From an epidemiological point of view, lost work days are often difficult to interpret because they are a function of some unknown combination of disability, demands of the job, availability of alternative light work, workplace policies such as sick leave, disability qualification criteria and individual differences in pain tolerance, the propensity to work with pain, and possibly the same factors that motivate attendance. More work is needed to develop and validate more interpretable occupational injury severity measures, particularly anatomical scales, disability scales and measures of impairment in the various dimensions of quality of life.
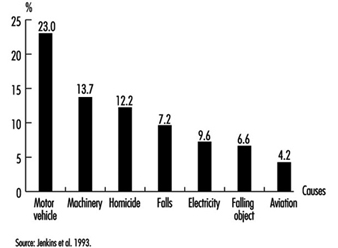
Unlike traditional safety practice, the public health community is not restricted to an interest in unintentional (“accidental”) injuries and the events that cause them. Through looking at the individual causes of fatalities in the workplace, it was found, for example, that in the United States, homicide (an intentional injury) is the leading cause of death at work among women and the third leading cause among men (Baker et al. 1992; Jenkins et al. 1993). Such fatalities are very rare events in individual workplaces and thus their importance is often overlooked, as is the fact that motor vehicle injuries are the single leading cause of fatal injuries on the job (figure 1). Based on these surveillance data, injuries and death due to violence in the workplace and to motor vehicle crashes are priorities in the public health approach to occupational injury prevention in the United States.
Figure 1.Leading causes of work-related injury/death, US 1980-1989
Assessment in Public Health
Assessment in public health is a multidisciplinary effort which involves surveillance, aetiological research, and community and organizational needs assessment. The purpose of injury surveillance is to identify high-risk populations, to identify injuries with significant public health impact, to detect and monitor trends and to generate hypotheses. Surveillance programmes can collect data on injury fatalities, non-fatal injuries, incidents with injury potential, and exposure to hazards. Data sources for occupational injury surveillance include health care providers (hospitals and physicians), death certificates, medical examiner/coroner reports, employer-based reporting to departments of labour or health, workers’ compensation agencies, periodic surveys of employers or households, and individual corporate records. Many of these reports and records are required by law but often offer incomplete information due to a lack of coverage of all workers, incentives to under-report, and a poor level of specificity in injury details.
In-depth investigations of individual incidents employ a variety of approaches which permit the use of expert judgement to draw conclusions about what caused the event and how it could have been prevented (Ferry 1988). Preventive action is often taken based on the findings from a single incident. Rate-based surveillance, on the other hand, has a broader significance than the individual incident. Indeed, some information from traditional accident investigations can have little epidemiological interpretation when aggregated into statistics. Accident investigation in the tradition of Heinrich (1959), for example, often produces statistics indicating that in excess of 80 of industrial injuries are caused solely by unsafe acts. From an epidemiological point of view, such statistics are difficult to interpret except as a survey of value judgements, and are rarely included in rate-based surveillance. Many other risk factors such as shift work, work stress, poorly designed work environments and so on, are often not included in investigation forms and thus are not considered in examining statistics on injury causes.
One of the primary purposes of surveillance is to identify high-risk groups in order to target further investigation and prevention. Injuries, like infectious and chronic diseases, have distinct patterns of risk that vary by age, sex, race, geographic region, industry and occupation (Baker et al. 1992). In the United States during the 1980s, for example, surveillance by the National Institute for Occupational Safety and Health (NIOSH) revealed the following high-risk groups for occupational injury fatality: males; elderly workers; blacks; workers in rural Western states; transportation and materials moving occupations; farming, forestry and fishing occupations; and labourers (Jenkins et al. 1993). Another important aspect of surveillance is to identify the types of injury that occur with the greatest frequency and severity, such as the leading external causes of work-related injury fatality in the United States (see figure 1 ). At an individual company level, problems such as homicide and motor vehicle fatalities are rare events and thus are seldom addressed by many traditional safety programmes. However, national surveillance data identified these among the three leading causes of occupational injury fatalities. Assessing the impact of non-fatal injuries requires the use of severity measures in order to make meaningful interpretations. For example, back injuries are a common cause of lost days of work, but an infrequent cause of hospitalization for work-related injuries.
Surveillance data alone do not represent a complete assessment in the public health tradition. Particularly in community-oriented public health practice, needs assessment and community diagnosis using surveys, focus groups and other techniques are important steps to assess what problems workers or communities perceive are important, what are the prevalent attitudes, intentions and barriers regarding the adoption of prevention measures, and how an organization or community really functions. A community-based agricultural safety programme, for example, might need to identify whether or not farmers perceive that tractor rollovers are a critical problem, what barriers such as financial or time constraints may prevent the installation of rollover protective structures, and through whom an intervention strategy should be implemented (e.g., trade association, youth organization, organization of farm wives). In addition to a diagnosis of the community, organizational needs assessment identifies an organization’s capacity, workload and constraints to implement fully any already existing prevention programmes such as the enforcement activities of a governmental department of labour (or health) or the safety department of a large corporation.
Investigating the aetiology or causation of loss incidents and injuries is another step in the public health approach to occupational injury control. Such studies of occupational disease have been the mainstay of developing disease-control programmes in the workplace. Aetiological research involves the application of epidemiology to identify risk factors for injury. It also involves applied social sciences to identify the determinants of organizational and individual behaviours that lead to unsafe conditions. Epidemiological research seeks to identify modifiable risk factors through the use of controlled, usually observational study designs such as the case-control study, the cohort study, the panel study and the cross-sectional study. As with epidemiological studies of other acute health events (e.g., asthma attacks, sudden cardiac arrests), aetiological research on injuries is challenged by the need to study either rare or recurrent events that are highly influenced by situational exposures that occur immediately before the event (e.g., distraction by impact noise) and by social and behavioural constructs that are difficult to measure (e.g., safety climate, job strain) (Veazie et al. 1994). Only recently have epidemiological and statistical methods been developed to accommodate the study of these types of health events.
Epidemiological studies that focus on the occurrence of injury are expensive and are not always needed. It does not require a controlled epidemiological study to document the impact of a lack of machine guarding on amputations due to a particular machine; a series of case investigations would suffice. Similarly, if an easily measurable individual behaviour such as failing to use a seat-belt is already a known risk factor, then studies focusing on the determinants of the behaviour and how to improve usage rates, are more useful than studying the injury. However, controlled epidemiological studies of injury and injury severity are needed to provide an understanding of a variety of causal mechanisms that are responsible for decrements in the performance of humans or technology that are difficult to measure. The effect of noise exposure or shift work, for example, on the risk and severity of injury is unlikely to be quantified by case investigations or by studies of easy-to-measure behaviours.
A recent review of studies on risk factors of occupational injuries revealed that age, job title, physical attributes or impairments and experience in the job or task were the most commonly studied human variables (Veazie et al. 1994). Shift work and scheduling were the most commonly studied job content variables. The work environment was the least studied. Most environment factors related to design features or recognized material hazards. Some studies examined factors in the organization and social environment. A few studies evaluated physical stressors such as heat and noise exposure as risk factors for injury. Many of these studies were of poor methodological quality, and few were replicated in different populations. Thus, little is known about risk factors for injury at work, except for the most obvious immediate causes. Future research may benefit by examining the impact on injury rates of risk factors predicted by theory in human factors, ergonomics, occupational stress and organizational behaviour. These may include design and scheduling of tasks and jobs, psychosocial factors (e.g., worker control, social support, psychological demands), and organizational structure and change (e.g., continuous quality improvement and management commitment to safety).
The public health approach also integrates injury epidemiology with the applied behavioural sciences (particularly health promotion, health behaviour and health policy research) to identify the modifiable, environmental reasons for unsafe worker behaviour and, most important, for behaviours on the part of employers and managers that lead to the creation and persistence of hazards. In the large organizational setting, this effort must involve research in organizational behaviour and industrial psychology. Thus, the assessment phase in the public health approach involves epidemiological surveillance, in-depth investigations, community and organizational needs assessment, and aetiological research based on the application of epidemiology and applied behavioural sciences.
Prevention Strategies
A number of principles guide the selection and implementation of prevention measures in a public health approach to injury control. These include:
(1) The importance of basing prevention measures on prior assessment and evaluation. The first principle acknowledges the importance of selecting interventions that are targeted to have a high impact on community health status and are likely to be successfully implemented. Thus, interventions selected on the basis of a thorough assessment phase, rather than merely common sense, are more likely to be effective. Interventions that have been demonstrated as effective in the past are even more promising. Unfortunately, very few occupational injury interventions have been scientifically evaluated (Goldenhar and Schulte 1994).
(2) The relative importance of control measures that automatically protect the worker. The second principle emphasizes the continuum between active and passive protection. Active protection is that which requires constant repetitive individual action; passive protection offers relatively automatic protection. For example, seat-belts require individual action to initiate protection each time someone gets into a vehicle. An air bag, on the other hand, bestows protection on a vehicle occupant without any initiating action—it automatically protects that person. Active interventions require modifying and sustaining individual behaviour change, which has been the least successful of injury prevention strategies to date. This principle is similar to the traditional hierarchy of controls in occupational safety which emphasizes the importance of engineering controls over administrative controls, personal protective equipment and training.
(3) The importance of behaviour modification rather than education. The third principle recognizes the importance of behaviour modification and that not all hazards can be engineered out of the environment at the manufacturing stage. Modification of the behaviour of employers, managers and employees is central, not only to the installation and maintenance of passive protection, but to most other occupational injury control strategies as well. Another important aspect of this principle is that classroom instruction, posters, pamphlets and other forms of education that merely seek to increase knowledge, usually have little effect on behaviour when used alone. Most health behaviour theories applied in health promotion focus on a variety of factors that motivate behaviour change other than awareness of a physical hazard or safe behaviour. The Health Belief Model, for example, emphasizes that self-protective behaviour is most influenced by the perception of risk, the perception of severity and the perception of the benefits and barriers associated with taking protective action (Green and Kreuter 1991).
While credible educational messages may alter some of these perceptions, sometimes the best way to alter these perceptions is to change the physical and social environment. A potentially effective approach to behaviour modification is to redesign equipment and the physical environment to make safe behaviour easier, quicker, and more comfortable or socially desirable than unsafe behaviour. If the layout of machine shop equipment is designed to make walking through hazardous zones difficult and unnecessary, then this unsafe behaviour will be reduced. Similarly, if hard hats are designed to be comfortable and to enhance the social image of the construction worker, they may be used more often.
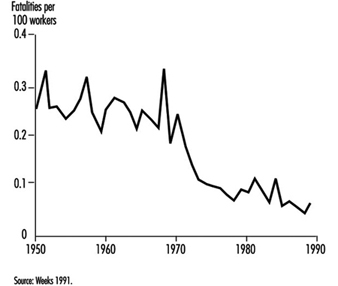
The social environment can also be modified to change behaviour. For example, legislation and enforcement is another far-reaching strategy in injury prevention that changes behaviour and extends beyond education alone. Seat-belt laws and laws requiring the use of infant safety seats, for example, have dramatically reduced motor vehicle fatalities in the United States. The effect of legislation and enforcement on occupational safety, however, is less well-described. One notable exception is the documented clear, dramatic decline in US mine fatalities that followed the implementation of the Federal Coal Mine Health and Safety Act of 1969 (figure 2 ). The resources and administrative authority devoted to mine safety enforcement is, however, much greater than that available to most other agencies (Weeks 1991).
Figure 2.Coal mining regulations and mortality rates, US 1950-1990
Well-designed occupational safety training often involves modifying the social environment by including a role modelling process, incentives, and feedback on safety performance (Johnston, Cattledge and Collins 1994). Another form of training, labour education, represents an altered social environment (Wallerstein and Baker 1994). It empowers workers to recognize hazards and to modify the behaviour of their employers so as to reduce those hazards. While education alone is not usually sufficient, it is usually a necessary component of any injury prevention programme (Gielen 1992). Educating employers and employees is a necessary part of the implementation of a specific injury prevention programme. Educating legislators, policy makers, health care providers and others is also important to initiating and sustaining community-wide injury prevention efforts. Indeed, interventions most likely to succeed in the field use a multifaceted approach which combines environmental modifications with policy changes and education (National Committee for Injury Prevention and Control 1989).
(4) Systematic consideration of all available options, including those that reduce not only injury occurrence but the severity and long-term consequences of injuries. The fourth principle is that the process of choosing interventions should systematically consider a wide range of options. The choice of countermeasures should not be determined by the relative importance of the causal factors or by their earliness in the sequence of events; rather priority must be given to those which most effectively reduce injury. A useful scheme for systematically considering injury control options was proposed by Haddon (1972). The Haddon Matrix reveals that interventions targeted at humans, the vehicles which can transfer damaging energy (e.g., cars, machinery), or the physical or psychosocial environment may operate to control injury in the pre-event, event or post-event phases. Table 1 shows the application of the Haddon Matrix to the problem of preventing motor vehicle injuries, which are the leading cause of occupational injury fatalities in many countries.
Table 1. The Haddon Matrix applied to motor vehicle injuries
|
Phases |
Factors |
||
|
Human |
Vehicles and equipment |
Environment |
|
|
Pre-event |
Educate public in the use of seat-belts and child restraints |
Safe brakes and tires |
Improved road design; restrict alcohol advertising and availability at gas stations |
|
Event |
Prevention of osteoporosis to decrease likelihood of fracture |
Air bags and a crashworthy vehicle design |
Breakaway utility poles and crash barriers |
|
Post-event |
Treatment of haemophilia and other conditions that result in impaired healing |
Safe design of fuel tank to prevent rupture and fire |
Adequate emergency medical care and rehabilitation |
Source: National Committee for Injury Prevention and Control 1989.
Traditional occupational safety interventions most often operate in the pre-event phase to prevent the initiation of an incident with potential to cause injury (i.e., an accident). Event phase interventions such as building cars to be more crashworthy or using safety lanyards while working at elevations, do not prevent accidents, but minimize the probability and severity of injury. After the event is over—the cars in a crash have stopped moving or the worker has stopped falling—post-event interventions such as first aid and prompt transport to appropriate surgical care seek to minimize the health consequences of injury (i.e., the probability of death or long-term disability).
In the public health approach, it is important to avoid getting locked into one phase of the matrix. Just as injury is multifactorial in causation, prevention strategies should address as many phases and aspects of injury as possible (but not necessarily all). The Haddon Matrix, for example, emphasizes that injury control is not limited to preventing accidents. In fact, many of our most effective control strategies do not prevent accidents or even injuries, but can considerably reduce their severity. Seat-belts and air bags in cars, safety helmets, fall protection in construction, rollover protective structures in agriculture, and emergency eyewash fountains in the laboratory are but a few examples of event-phase strategies that do nothing to prevent an accident from occurring. Instead, they reduce the severity of injury after the accident has been initiated. Even after the anatomical damage has been done, much can be done to reduce the risk of death and long-term disability. In the United States, it has been estimated that many major trauma deaths could be prevented by systems that minimize the time delay between injury and definitive surgical care. This broader framework is called injury control and goes far beyond traditional accident prevention. A commonly used phrase to illustrate this point is “Injuries are not an accident”. They can be predicted and their impact on society controlled.
Another useful scheme often used for systematically considering injury control options is Haddon’s Ten Countermeasure Strategies (Haddon 1973). Table 2 shows how these strategies can be applied to controlling injury from falls in construction. As shown, not all strategies will be applicable for specific problems.
(5) Involvement of the community, workers and management. The fifth principle is the importance of involving the target population (communities, workers, managers) in choosing and implementing intervention strategies. Cost, feasibility, convenience and acceptability can all be barriers to developing effective prevention strategies (Schelp 1988).
Table 2. Haddon’s Ten Countermeasure Strategies applied to injuries due to falls in construction
|
Countermeasure |
Intervention (and relevant notes) |
|
Prevent the creation of the hazard. |
Do not construct buildings—generally not a practical option, to be sure. |
|
Reduce the amount of the hazard |
Lower the height of construction project to below fatal levels—usually not practical, but may be possible in some work zones. |
|
Prevent the release of the hazard. |
Install non-slip walking surfaces on roofs and other heights. |
|
Modify the rate of release of the hazard from |
Use safety lanyards. Use safety nets. |
|
Separate the hazard from the worker by time and space. |
Do not schedule unnecessary foot traffic near fall hazards until the hazards are abated. |
|
Separate the hazard from the worker by physical barriers. |
Install guardrails on elevated surfaces. |
|
Modify basic qualities of the hazard. |
Remove sharp or protruding projections on the ground surface where workers can |
|
Make worker as injury resistant as possible. |
Require, e.g., safety helmets. |
|
Begin to counter damage done by the hazard. |
Apply first aid. |
|
Stabilize, treat and rehabilitate worker. |
Develop a regionalized trauma system; provide |
Evaluation in Public Health
Evaluation in both applied social sciences and epidemiology is “a process that attempts to determine as systematically and objectively as possible the relevance, effectiveness and impact of activities in light of their objectives” (Last 1988). Evaluation is an essential component of public health practice. It occurs at two levels. The first level relies on surveillance systems to determine whether or not entire communities have met their disease and injury reduction objectives, without attempting to determine what caused the observed changes. Federal, state and local government agencies in the United States, for example, have set objectives for the year 2000. One of these objectives is to reduce work-related injures resulting in medical treatment, lost time from work, or restricted work activity to no more than 6 cases per 100 full-time workers per year. Progress in meeting these objectives will be monitored with the national surveillance systems in place.
The second level of evaluation focuses on determining the effectiveness of policies, programmes and specific interventions. Ideally, this requires the application of controlled experimental or quasi-experimental study designs. Mohr and Clemmer (1989), for example, conducted a time series study of injury rates in those mobile off-shore oil rigs that opted to implement a new technology to assist workers in connecting drill pipes, compared with rates in those rigs that did not have the new technology. Although injury rates were going down over the period of the installation of the new equipment, the authors were able to attribute a decrease of 6 injuries per 100 workers per year to the new safety equipment and to demonstrate that the savings from injury prevention resulted in a full recovery of the initial capital and installation costs within 5.7 years. Unfortunately, this type of scientific evaluation of programmes and interventions in occupational health and safety is rare and often methodologically flawed (Goldenhar and Schulte 1994).
Summary
The above-mentioned programme demonstrates well the various components in the public health approach to reducing injuries in the workplace. Assessing the injury problem and establishing an ongoing surveillance system was an essential part of this and earlier studies of injuries on oil rigs that were conducted by these authors. The subsequent development of a simple engineering prevention strategy was then followed by a rigorous evaluation strategy which included an evaluation of cost savings. Such studies have been the mainstay of the public health approach to the prevention of other occupational diseases. In the future, the integration of occupational injury prevention into the assessment, intervention and evaluation phases of public health practice has the potential to be an important step toward more effective protection and promotion of health in communities.