Description, Sources, Mechanisms
Apart from the transportation of radioactive materials, there are three settings in which radiation accidents can occur:
- use of nuclear reactions to produce energy or arms, or for research purposes
- industrial applications of radiation (gamma radiography, irradiation)
- research and nuclear medicine (diagnosis or therapy).
Radiation accidents may be classified into two groups on the basis of whether or not there is environmental emission or dispersion of radionuclides; each of these types of accident affects different populations.
The magnitude and duration of the exposure risk for the general population depends on the quantity and the characteristics (half-life, physical and chemical properties) of the radionuclides emitted into the environment (table 1). This type of contamination occurs when there is rupture of the containment barriers at nuclear power plants or industrial or medical sites which separate radioactive materials from the environment. In the absence of environmental emissions, only workers present onsite or handling radioactive equipment or materials are exposed.
Table 1. Typical radionuclides, with their radioactive half-lives
|
Radionuclide |
Symbol |
Radiation emitted |
Physical half-life* |
Biological half-life |
|
Barium-133 |
Ba-133 |
γ |
10.7 y |
65 d |
|
Cerium-144 |
Ce-144 |
β,γ |
284 d |
263 d |
|
Caesium-137 |
Cs-137 |
β,γ |
30 y |
109 d |
|
Cobalt-60 |
Co-60 |
β,γ |
5.3 y |
1.6 y |
|
Iodine-131 |
I-131 |
β,γ |
8 d |
7.5 d |
|
Plutonium-239 |
Pu-239 |
α,γ |
24,065 y |
50 y |
|
Polonium-210 |
Po-210 |
α |
138 d |
27 d |
|
Strontium-90 |
Sr-90 |
β |
29.1 y |
18 y |
|
Tritium |
H-3 |
β |
12.3 y |
10 d |
* y = years; d = days.
Exposure to ionizing radiation may occur through three routes, regardless of whether the target population is composed of workers or the general public: external irradiation, internal irradiation, and contamination of skin and wounds.
External irradiation occurs when individuals are exposed to an extracorporeal radiation source, either point (radiotherapy, irradiators) or diffuse (radioactive clouds and fallout from accidents, figure 1). Irradiation may be local, involving only a portion of the body, or whole body.
Figure 1. Exposure pathways to ionizing radiation after an accidental release of radioactivity in the environment
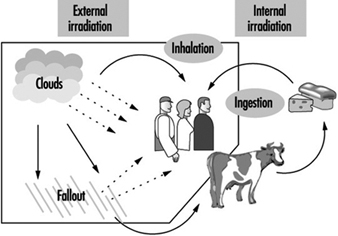
Internal radiation occurs following incorporation of radioactive substances into the body (figure 1) through either inhalation of airborne radioactive particles (e.g., caesium-137 and iodine-131, present in the Chernobyl cloud) or ingestion of radioactive materials in the food chain (e.g., iodine-131 in milk). Internal irradiation may affect the whole body or only certain organs, depending on the characteristics of the radionuclides: caesium-137 distributes itself homogeneously throughout the body, while iodine-131 and strontium-90 concentrate in the thyroid and the bones, respectively.
Finally, exposure may also occur through direct contact of radioactive materials with skin and wounds.
Accidents involving nuclear power plants
Sites included in this category include power-generating stations, experimental reactors, facilities for the production and processing or reprocessing of nuclear fuel and research laboratories. Military sites include plutonium breeder reactors and reactors located aboard ships and submarines.
Nuclear power plants
The capture of heat energy emitted by atomic fission is the basis for the production of electricity from nuclear energy. Schematically, nuclear power plants can be thought of as comprising: (1) a core, containing the fissile material (for pressurized-water reactors, 80 to 120 tonnes of uranium oxide); (2) heat-transfer equipment incorporating heat-transfer fluids; (3) equipment capable of transforming heat energy into electricity, similar to that found in power plants that are not nuclear.
Strong, sudden power surges capable of causing core meltdown with emission of radioactive products are the primary hazards at these installations. Three accidents involving reactor-core meltdown have occurred: at Three Mile Island (1979, Pennsylvania, United States), Chernobyl (1986, Ukraine), and Fukushima (2011, Japan) [Edited, 2011].
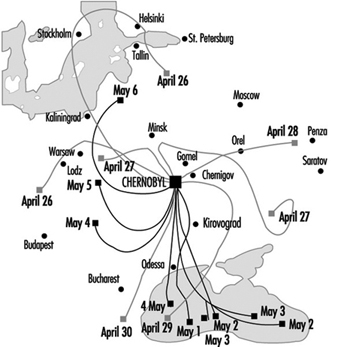
The Chernobyl accident was what is known as a criticality accident—that is, a sudden (within the space of a few seconds) increase in fission leading to a loss of process control. In this case, the reactor core was completely destroyed and massive amounts of radioactive materials were emitted (table 2). The emissions reached a height of 2 km, favouring their dispersion over long distances (for all intents and purposes, the entire Northern hemisphere). The behaviour of the radioactive cloud has proven difficult to analyse, due to meteorological changes during the emission period (figure 2) (IAEA 1991).
Table 2. Comparison of different nuclear accidents
|
Accident |
Type of facility |
Accident |
Total emitted |
Duration |
Main emitted |
Collective |
|
Khyshtym 1957 |
Storage of high- |
Chemical explosion |
740x106 |
Almost |
Strontium-90 |
2,500 |
|
Windscale 1957 |
Plutonium- |
Fire |
7.4x106 |
Approximately |
Iodine-131, polonium-210, |
2,000 |
|
Three Mile Island |
PWR industrial |
Coolant failure |
555 |
? |
Iodine-131 |
16–50 |
|
Chernobyl 1986 |
RBMK industrial |
Critically |
3,700x106 |
More than 10 days |
Iodine-131, iodine-132, |
600,000 |
|
Fukushima 2011
|
The final report of the Fukushima Assessment Task Force will be submitted in 2013. |
|
|
|
|
|
Source: UNSCEAR 1993.
Figure 2. Trajectory of emissions from the Chernobyl accident, 26 April-6 May 1986
Contamination maps were drawn up on the basis of environmental measurements of caesium-137, one of the main radioactive emission products (table 1 and table 2). Areas of Ukraine, Byelorussia (Belarus) and Russia were heavily contaminated, while fallout in the rest of Europe was less significant (figure 3 and figure 4 (UNSCEAR 1988). Table 3 presents data on the area of the contaminated zones, characteristics of the exposed populations and routes of exposure.
FIgure 3. Caesium-137 deposition in Byelorussia, Russia and Ukraine following the Chernobyl accident.

Figure 4. Caesium-137 fallout (kBq/km2) in Europe following the Chernobyl accident
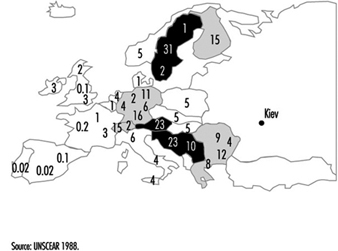
Table 3. Area of contaminated zones, types of populations exposed and modes of exposure in Ukraine, Byelorussia and Russia following the Chernobyl accident
|
Type of population |
Surface area ( km2 ) |
Population size (000) |
Main modes of exposure |
|
Occupationally exposed populations: |
|||
|
Employees onsite at |
≈0.44 |
External irradiation, |
|
|
General public: |
|||
|
Evacuated from the |
|
115 |
External irradiation by |
* Individuals participating in clean-up within 30 km of the site. These include fire-fighters, military personnel, technicians and engineers who intervened during the first weeks, as well as physicians and researchers active at a later date.
** Caesium-137 contamination.
Source: UNSCEAR 1988; IAEA 1991.
The Three Mile Island accident is classified as a thermal accident with no reactor runaway, and was the result of a reactor-core coolant failure lasting several hours. The containment shell ensured that only a limited quantity of radioactive material was emitted into the environment, despite the partial destruction of the reactor core (table 2). Although no evacuation order was issued, 200,000 residents voluntarily evacuated the area.
Finally, an accident involving a plutonium production reactor occurred on the west coast of England in 1957 (Windscale, table 2). This accident was caused by a fire in the reactor core and resulted in environmental emissions from a chimney 120 metres high.
Fuel-processing facilities
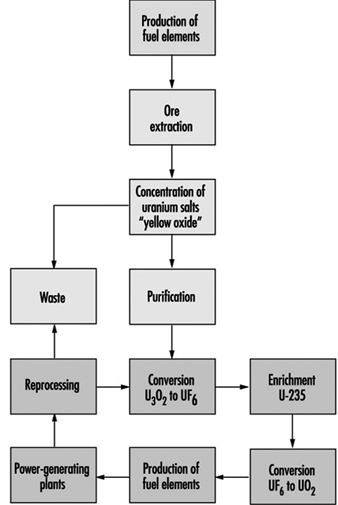
Fuel production facilities are located “upstream” from nuclear reactors and are the site of ore extraction and the physical and chemical transformation of uranium into fissile material suitable for use in reactors (figure 5). The primary accident hazards present in these facilities are chemical in nature and related to the presence of uranium hexafluoride (UF6), a gaseous uranium compound which may decompose upon contact with air to produce hydrofluoric acid (HF), a very corrosive gas.
Figure 5. Nuclear fuel processing cycle.
“Downstream” facilities include fuel storage and reprocessing plants. Four criticality accidents have occurred during chemical reprocessing of enriched uranium or plutonium (Rodrigues 1987). In contrast to accidents occurring at nuclear power plants, these accidents involved small quantities of radioactive materials—tens of kilograms at most—and resulted in negligible mechanical effects and no environmental emission of radioactivity. Exposure was limited to very high dose, very short term (of the order of minutes) external gamma ray and neutron irradiation of workers.
In 1957, a tank containing highly radioactive waste exploded at Russia’s first military-grade plutonium production facility, located in Khyshtym, in the south Ural Mountains. Over 16,000 km2 were contaminated and 740 PBq (20 MCi) were emitted into the atmosphere (table 2 and table 4).
Table 4. Surface area of the contaminated zones and size of population exposed after the Khyshtym accident (Urals 1957), by strontium-90 contamination
|
Contamination ( kBq/m2 ) |
( Ci/km2 ) |
Area ( km2 ) |
Population |
|
≥ 37,000 |
≥ 1,000 |
20 |
1,240 |
|
≥ 3,700 |
≥100 |
120 |
1,500 |
|
≥ 74 |
≥ 2 |
1,000 |
10,000 |
|
≥ 3.7 |
≥ 0.1 |
15,000 |
270,000 |
Research reactors
Hazards at these facilities are similar to those present at nuclear power plants, but are less serious, given the lower power generation. Several criticality accidents involving significant irradiation of personnel have occurred (Rodrigues 1987).
Accidents related to the use of radioactive sources in industry and medicine (excluding nuclear plants) (Zerbib 1993)
The most common accident of this type is the loss of radioactive sources from industrial gamma radiography, used, for example, for the radiographic inspection of joints and welds. However, radioactive sources may also be lost from medical sources (table 5). In either case, two scenarios are possible: the source may be picked up and kept by a person for several hours (e.g., in a pocket), then reported and restored, or it may be collected and carried home. While the first scenario causes local burns, the second may result in long-term irradiation of several members of the general public.
Table 5. Accidents involving the loss of radioactive sources and which resulted in exposure of the general public
|
Country (year) |
Number of |
Number of |
Number of deaths** |
Radioactive material involved |
|
Mexico (1962) |
? |
5 |
4 |
Cobalt-60 |
|
China (1963) |
? |
6 |
2 |
Cobalt 60 |
|
Algeria (1978) |
22 |
5 |
1 |
Iridium-192 |
|
Morocco (1984) |
? |
11 |
8 |
Iridium-192 |
|
Mexico |
≈4,000 |
5 |
0 |
Cobalt-60 |
|
Brazil |
249 |
50 |
4 |
Caesium-137 |
|
China |
≈90 |
12 |
3 |
Cobalt-60 |
|
United States |
≈90 |
1 |
1 |
Iridium-192 |
* Individuals exposed to doses capable of causing acute or long-term effects or death.
** Among individuals receiving high doses.
Source: Nénot 1993.
The recovery of radioactive sources from radiotherapy equipment has resulted in several accidents involving the exposure of scrap workers. In two cases—the Juarez and Goiânia accidents—the general public was also exposed (see table 5 and box below).
The Goiвnia Accident, 1987
Between 21 September and 28 September 1987, several people suffering from vomiting, diarrhoea, vertigo and skin lesions at various parts of the body were admitted to the hospital specializing in tropical diseases in Goiânia, a city of one million inhabitants in the Brazilian state of Goias. These problems were attributed to a parasitic disease common in Brazil. On 28 September, the physician responsible for health surveillance in the city saw a woman who presented him with a bag containing debris from a device collected from an abandoned clinic, and a powder which emitted, according to the woman “a blue light”. Thinking that the device was probably x-ray equipment, the physician contacted his colleagues at the hospital for tropical diseases. The Goias Department of the Environment was notified, and the next day a physicist took measurements in the hygiene department’s yard, where the bag was stored overnight. Very high radioactivity levels were found. In subsequent investigations the source of radioactivity was identified as a caesium-137 source (total activity: approximately 50 TBq (1,375 Ci)) which had been contained within radiotherapy equipment used in a clinic abandoned since 1985. The protective housing surrounding the caesium had been disassembled on 10 September 1987 by two scrapyard workers and the caesium source, in powder form, removed. Both the caesium and the fragments of the contaminated housing were gradually dispersed throughout the city. Several people who had transported or handled the material, or who had simply come to see it (including parents, friends and neighbours) were contaminated. In all, over 100,000 people were examined, of whom 129 were very seriously contaminated; 50 were hospitalized (14 for medullary failure), and 4, including a 6-year-old girl, died. The accident had dramatic economic and social consequences for the entire city of Goiânia and the state of Goias: 1/1000 of the city’s surface area was contaminated, and the price of agricultural produce, rents, real estate, and land all fell. The inhabitants of the entire state suffered real discrimination.
Source: IAEA 1989a
The Juarez accident was discovered serendipitously (IAEA 1989b). On 16 January 1984, a truck entering the Los Alamos (New Mexico, United States) scientific laboratory loaded with steel bars triggered a radiation detector. Investigation revealed the presence of cobalt-60 in the bars and traced the cobalt-60 to a Mexican foundry. On January 21, a heavily contaminated scrapyard in Juarez was identified as the source of the radioactive material. Systematic monitoring of roads and highways by detectors resulted in the identification of a heavily contaminated truck. The ultimate radiation source was determined to be a radiotherapy device stored in a medical centre until December 1983, at which time it was disassembled and transported to the scrapyard. At the scrapyard, the protective housing surrounding the cobalt-60 was broken, freeing the cobalt pellets. Some of the pellets fell into the truck used to transport scrap, and others were dispersed throughout the scrapyard during subsequent operations, mixing with the other scrap.
Accidents involving the entry of workers into active industrial irradiators (e.g., those used to preserve food, sterilize medical products, or polymerize chemicals) have occurred. In all cases, these have been due to failure to follow safety procedures or to disconnected or defective safety systems and alarms. The dose levels of external irradiation to which workers in these accidents were exposed were high enough to cause death. Doses were received within a few seconds or minutes (table 6).
Table 6. Main accidents involving industrial irradiators
|
Site, date |
Equipment* |
Number of |
Exposure level |
Affected organs |
Dose received (Gy), |
Medical effects |
|
Forbach, August 1991 |
EA |
2 |
several deciGy/ |
Hands, head, trunk |
40, skin |
Burns affecting 25–60% of |
|
Maryland, December 1991 |
EA |
1 |
? |
Hands |
55, hands |
Bilateral finger amputation |
|
Viet nam, November 1992 |
EA |
1 |
1,000 Gy/minute |
Hands |
1.5, whole body |
Amputation of the right hand and a finger of the left hand |
|
Italy, May 1975 |
CI |
1 |
Several minutes |
Head, whole body |
8, bone marrow |
Death |
|
San Salvador, February 1989 |
CI |
3 |
? |
Whole body, legs, |
3–8, whole body |
2 leg amputations, 1 death |
|
Israel, June 1990 |
CI |
1 |
1 minute |
Head, whole body |
10–20 |
Death |
|
Belarus, October 1991 |
CI |
1 |
Several minutes |
Whole body |
10 |
Death |
* EA: electron accelerator CI: cobalt-60 irradiator.
Source: Zerbib 1993; Nénot 1993.
Finally, medical and scientific personnel preparing or handling radioactive sources may be exposed through skin and wound contamination or inhalation or ingestion of radioactive materials. It should be noted that this type of accident is also possible in nuclear power plants.
Public Health Aspects of the Problem
Temporal patterns
The United States Radiation Accident Registry (Oak Ridge, United States) is a worldwide registry of radiation accidents involving humans since 1944. To be included in the registry, an accident must have been the subject of a published report and have resulted in whole-body exposure exceeding 0.25 Sievert (Sv), or skin exposure exceeding 6 Sv or exposure of other tissues and organs exceeding 0.75 Sv (see "Case Study: What does dose mean?" for a definition of dose). Accidents that are of interest from the point of view of public health but which resulted in lower exposures are thus excluded (see below for a discussion of the consequences of exposure).
Analysis of the registry data from 1944 to 1988 reveals a clear increase in both the frequency of radiation accidents and the number of exposed individuals starting in 1980 (table 7). The increase in the number of exposed individuals is probably accounted for by the Chernobyl accident, particularly the approximately 135,000 individuals initially residing in the prohibited area within 30 km of the accident site. The Goiânia (Brazil) and Juarez (Mexico) accidents also occurred during this period and involved significant exposure of many people (table 5).
Table 7. Radiation accidents listed in the Oak Ridge (United States) accident registry (worldwide, 1944-88)
|
1944–79 |
1980–88 |
1944–88 |
|
|
Total number of accidents |
98 |
198 |
296 |
|
Number of individuals involved |
562 |
136,053 |
136,615 |
|
Number of individuals exposed to doses exceeding |
306 |
24,547 |
24,853 |
|
Number of deaths (acute effects) |
16 |
53 |
69 |
* 0.25 Sv for whole-body exposure, 6 Sv for skin exposure, 0.75 Sv for other tissues and organs.
Potentially exposed populations
From the point of view of exposure to ionizing radiation, there are two populations of interest: occupationally exposed populations and the general public. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR 1993) estimates that 4 million workers worldwide were occupationally exposed to ionizing radiation in the period 1985-1989; of these, approximately 20% were employed in the production, use and processing of nuclear fuel (table 8). IAEA member countries were estimated to possess 760 irradiators in 1992, of which 600 were electron accelerators and 160 gamma irradiators.
Table 8. Temporal pattern of occupational exposure to ionizing radiation worldwide (in thousands)
|
Activity |
1975–79 |
1980–84 |
1985–89 |
|
Nuclear fuel processing* |
560 |
800 |
880 |
|
Military applications** |
310 |
350 |
380 |
|
Industrial applications |
530 |
690 |
560 |
|
Medical applications |
1,280 |
1,890 |
2,220 |
|
Total |
2,680 |
3,730 |
4,040 |
* Production and reprocessing of fuel: 40,000; reactor operation: 430,000.
** including 190,000 shipboard personnel.
Source: UNSCEAR 1993.
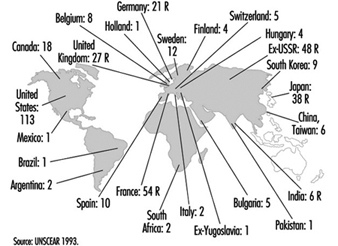
The number of nuclear sites per country is a good indicator of the potential for exposure of the general public (figure 6).
Figure 6. Distribution of power-generating reactors and fuel reprocessing plants in the world, 1989-90
Health Effects
Direct health effects of ionizing radiation
In general, the health effects of ionizing radiation are well known and depend on the dose level received and the dose rate (received dose per unit of time (see "Case Study: What does dose mean?").
Deterministic effects
These occur when the dose exceeds a given threshold and the dose rate is high. The severity of the effects is proportional to the dose, although the dose threshold is organ specific (table 9).
Table 9. Deterministic effects: thresholds for selected organs
|
Tissue or effect |
Equivalent single dose |
|
Testicles: |
|
|
Temporary sterility |
0.15 |
|
Permanent sterility |
3.5–6.0 |
|
Ovaries: |
|
|
Sterility |
2.5–6.0 |
|
Crystalline lens: |
|
|
Detectable opacities |
0.5–2.0 |
|
Impaired vision (cataracts) |
5.0 |
|
Bone marrow: |
|
|
Depression of haemopoiesis |
0.5 |
Source: ICRP 1991.
In the accidents such as those discussed above, deterministic effects may be caused by local intense irradiation, such as that caused by external irradiation, direct contact with a source (e.g., a misplaced source picked up and pocketed) or skin contamination. All these result in radiological burns. If the local dose is of the order of 20 to 25 Gy (table 6, "Case Study: What does dose mean?") tissue necrosis may ensue. A syndrome known as acute irradiation syndrome, characterized by digestive disorders (nausea, vomiting, diarrhoea) and bone marrow aplasia of variable severity, may be induced when the average whole-body irradiation dose exceeds 0.5 Gy. It should be recalled that whole-body and local irradiation may occur simultaneously.
Nine of 60 workers exposed during criticality accidents at nuclear fuel processing plants or research reactors died (Rodrigues 1987). Decedents received 3 to 45 Gy, while survivors received 0.1 to 7 Gy. The following effects were observed in survivors: acute irradiation syndrome (gastro-intestinal and haematological effects), bilateral cataracts and necrosis of limbs, requiring amputation.
At Chernobyl, power plant personnel, as well as emergency response personnel not using special protective equipment, suffered high beta and gamma radiation exposure in the initial hours or days following the accident. Five hundred people required hospitalization; 237 individuals who received whole-body irradiation exhibited acute irradiation syndrome, and 28 individuals died despite treatment (table 10) (UNSCEAR 1988). Others received local irradiation of the limbs, in some cases affecting over 50% of the body surface and continue to suffer, many years later, multiple skin disorders (Peter, Braun-Falco and Birioukov 1994).
Table 10. Distribution of patients exhibiting acute irradiation syndrome (AIS) after the Chernobyl accident, by severity of condition
|
Severity of AIS |
Equivalent dose |
Number of |
Number of |
Average survival |
|
I |
1–2 |
140 |
– |
– |
|
II |
2–4 |
55 |
1 (1.8) |
96 |
|
III |
4–6 |
21 |
7 (33.3) |
29.7 |
|
IV |
>6 |
21 |
20 (95.2) |
26.6 |
Source: UNSCEAR 1988.
Stochastic effects
These are probabilistic in nature (i.e., their frequency increases with received dose), but their severity is independent of dose. The main stochastic effects are:
- Mutation. This has been observed in animal experiments but has been difficult to document in humans.
- Cancer. The effect of irradiation on the risk of developing cancer has been studied in patients receiving radiation therapy and in survivors of the Hiroshima and Nagasaki bombings. UNSCEAR (1988, 1994) regularly summarizes the results of these epidemiological studies. The duration of the latency period is typically 5 to 15 years from the date of exposure depending on organ and tissue. Table 11 lists the cancers for which an association with ionizing radiation has been established. Significant cancer excesses have been demonstrated among survivors of the Hiroshima and Nagasaki bombings with exposures above 0.2 Sv.
- Selected benign tumours. Benign thyroid adenomas.
Table 11. Results of epidemiological studies of the effect of high dose rate of external irradiation on cancer
|
Cancer site |
Hiroshima/Nagasaki |
Other studies |
|
|
Mortality |
Incidence |
||
|
Haematopoietic system |
|||
|
Leukaemia |
+* |
+* |
6/11 |
|
Lymphoma (not specified) |
+ |
0/3 |
|
|
Non-Hodgkin lymphoma |
+* |
1/1 |
|
|
Myeloma |
+ |
+ |
1/4 |
|
Oral cavity |
+ |
+ |
0/1 |
|
Salivary glands |
+* |
1/3 |
|
|
Digestive system |
|||
|
Oesophagus |
+* |
+ |
2/3 |
|
Stomach |
+* |
+* |
2/4 |
|
Small intestine |
1/2 |
||
|
Colon |
+* |
+* |
0/4 |
|
Rectum |
+ |
+ |
3/4 |
|
Liver |
+* |
+* |
0/3 |
|
Gall bladder |
0/2 |
||
|
Pancreas |
3/4 |
||
|
Respiratory system |
|||
|
Larynx |
0/1 |
||
|
Trachea, bronchi, lungs |
+* |
+* |
1/3 |
|
Skin |
|||
|
Not specified |
1/3 |
||
|
Melanoma |
0/1 |
||
|
Other cancers |
+* |
0/1 |
|
|
Breast (women) |
+* |
+* |
9/14 |
|
Reproductive system |
|||
|
Uterus (non-specific) |
+ |
+ |
2/3 |
|
Uterine body |
1/1 |
||
|
Ovaries |
+* |
+* |
2/3 |
|
Other (women) |
2/3 |
||
|
Prostate |
+ |
+ |
2/2 |
|
Urinary system |
|||
|
Bladder |
+* |
+* |
3/4 |
|
Kidneys |
0/3 |
||
|
Other |
0/1 |
||
|
Central nervous system |
+ |
+ |
2/4 |
|
Thyroid |
+* |
4/7 |
|
|
Bone |
2/6 |
||
|
Connective tissue |
0/4 |
||
|
All cancers, excluding leukaemias |
1/2 |
||
+ Cancer sites studied in the Hiroshima and Nagasaki survivors.
* Positive association with ionizing radiation.
1 Cohort (incidence or mortality) or case-control studies.
Source: UNSCEAR 1994.
Two important points concerning the effects of ionizing radiation remain controversial.
Firstly, what are the effects of low-dose irradiation (below 0.2 Sv) and low dose rates? Most epidemiological studies have examined survivors of the Hiroshima and Nagasaki bombings or patients receiving radiation therapy—populations exposed over very short periods to relatively high doses—and estimates of the risk of developing cancer as a result of exposure to low doses and dose rates depends essentially on extrapolations from these populations. Several studies of nuclear power plant workers, exposed to low doses over several years, have reported cancer risks for leukaemia and other cancers that are compatible with extrapolations from high-exposure groups, but these results remain unconfirmed (UNSCEAR 1994; Cardis, Gilbert and Carpenter 1995).
Secondly, is there a threshold dose (i.e., a dose below which there is no effect)? This is currently unknown. Experimental studies have demonstrated that damage to genetic material (DNA) caused by spontaneous errors or environmental factors are constantly repaired. However, this repair is not always effective, and may result in malignant transformation of cells (UNSCEAR 1994).
Other effects
Finally, the possibility of teratogenic effects due to irradiation during pregnancy should be noted. Microcephaly and mental retardation have been observed in children born to female survivors of the Hiroshima and Nagasaki bombings who received irradiation of at least 0.1 Gy during the first trimester (Otake, Schull and Yoshimura 1989; Otake and Schull 1992). It is unknown whether these effects are deterministic or stochastic, although the data do suggest the existence of a threshold.
Effects observed following the Chernobyl accident
The Chernobyl accident is the most serious nuclear accident to have occurred to date. However, even now, ten years after the fact, not all the health effects on the most highly exposed populations have been accurately evaluated. There are several reasons for this:
- Some effects appear only many years after the date of exposure: for example, solid-tissue cancers typically take 10 to 15 years to appear.
- As some time elapsed between the accident and the commencement of epidemiological studies, some effects occurring in the initial period following the accident may not have been detected.
- Useful data for the quantification of the cancer risk were not always gathered in a timely fashion. This is particularly true for data necessary to estimate the exposure of the thyroid gland to radioactive iodides emitted during the incident (tellurium-132, iodine-133) (Williams et al. 1993).
- Finally, many initially exposed individuals subsequently left the contaminated zones and were probably lost for follow-up.
Workers. Currently, comprehensive information is unavailable for all the workers who were strongly irradiated in the first few days following the accident. Studies on the risk to clean-up and relief workers of developing leukaemia and solid-tissue cancers are in progress (see table 3). These studies face many obstacles. Regular follow-up of the health status of clean-up and relief workers is greatly hindered by the fact that many of them came from different parts of the ex-USSR and were redispatched after working on the Chernobyl site. Further, received dose must be estimated retrospectively, as there are no reliable data for this period.
General population. The only effect plausibly associated with ionizing radiation in this population to date is an increase, starting in 1989, of the incidence of thyroid cancer in children younger than 15 years. This was detected in Byelorussia (Belarus) in 1989, only three years after the incident, and has been confirmed by several expert groups (Williams et al. 1993). The increase was particularly noteworthy in the most heavily contaminated areas of Belarus, especially the Gomel region. While thyroid cancer was normally rare in children younger than 15 years, (annual incidence rate of 1 to 3 per million), its incidence increased tenfold on a national basis and twentyfold in the Gomel area (table 12, figure 7), (Stsjazhko et al. 1995). A tenfold increase of the incidence of thyroid cancer was subsequently reported in the five most heavily contaminated areas of Ukraine, and an increase in thyroid cancer was also reported in the Bryansk (Russia) region (table 12). An increase among adults is suspected but has not been confirmed. Systematic screening programmes undertaken in the contaminated regions allowed latent cancers present prior to the accident to be detected; ultrasonographic programmes capable of detecting thyroid cancers as small as a few millimetres were particularly helpful in this regard. The magnitude of the increase in incidence in children, taken together with the aggressiveness of the tumours and their rapid development, suggests that the observed increases in thyroid gland cancer are partially due to the accident.
Table 12. Temporal pattern of the incidence and total number of thyroid cancers in children in Belarus, Ukraine & Russia, 1981-94
|
Incidence* (/100,000) |
Number of cases |
|||
|
1981–85 |
1991–94 |
1981–85 |
1991–94 |
|
|
Belarus |
||||
|
Entire country |
0.3 |
3.06 |
3 |
333 |
|
Gomel area |
0.5 |
9.64 |
1 |
164 |
|
Ukraine |
||||
|
Entire country |
0.05 |
0.34 |
25 |
209 |
|
Five most heavily |
0.01 |
1.15 |
1 |
118 |
|
Russia |
||||
|
Entire country |
? |
? |
? |
? |
|
Bryansk and |
0 |
1.00 |
0 |
20 |
* Incidence: the ratio of the number of new cases of a disease during a given period to the size of the population studied in the same period.
Source: Stsjazhko et al. 1995.
Figure 7. Incidence of cancer of the thyroid in children younger than 15 years in Belarus

In the most heavily contaminated zones (e.g., the Gomel region), the thyroid doses were high, particularly among children (Williams et al. 1993). This is consistent with the significant iodine emissions associated with the accident and the fact that radioactive iodine will, in the absence of preventive measures, concentrate preferentially in the thyroid gland.
Exposure to radiation is a well-documented risk factor for thyroid cancer. Clear increases in the incidence of thyroid cancer have been observed in a dozen studies of children receiving radiation therapy to the head and neck. In most cases, the increase was clear ten to 15 years after exposure, but was detectable in some cases within three to seven years. On the other hand, the effects in children of internal irradiation by iodine-131 and by short half-life iodine isotopes are not well established (Shore 1992).
The precise magnitude and pattern of the increase in the coming years of the incidence of thyroid cancer in the most highly exposed populations should be studied. Epidemiological studies currently under way should help to quantify the association between the dose received by the thyroid gland and the risk of developing thyroid cancer, and to identify the role of other genetic and environmental risk factors. It should be noted that iodine deficiency is widespread in the affected regions.
An increase in the incidence of leukaemia, particularly juvenile leukaemia (since children are more sensitive to the effects of ionizing radiation), is to be expected among the most highly exposed members of the population within five to ten years of the accident. Although no such increase has yet been observed, the methodological weaknesses of the studies conducted to date prevent any definitive conclusions from being drawn.
Psychosocial effects
The occurrence of more or less severe chronic psychological problems following psychological trauma is well established and has been studied primarily in populations faced with environmental disasters such as floods, volcanic eruptions and earthquakes. Post-traumatic stress is a severe, long-lasting and crippling condition (APA 1994).
Most of our knowledge on the effect of radiation accidents on psychological problems and stress is drawn from studies conducted in the wake of the Three Mile Island accident. In the year following the accident, immediate psychological effects were observed in the exposed population, and mothers of young children in particular exhibited increased sensitivity, anxiety and depression (Bromet et al. 1982). Further, an increase in depression and anxiety-related problems was observed in power-plant workers, compared to workers in another power plant (Bromet et al. 1982). In the following years (i.e., after the reopening of the power plant), approximately one-quarter of the surveyed population exhibited relatively significant psychological problems. There was no difference in the frequency of psychological problems in the rest of the survey population, compared to control populations (Dew and Bromet 1993). Psychological problems were more frequent among individuals living close to the power plant who were without a social support network, had a history of psychiatric problems, or who had evacuated their home at the time of the accident (Baum, Cohen and Hall 1993).
Studies are also under way among populations exposed during the Chernobyl accident and for whom stress appears to be an important public health issue (e.g., clean-up and relief workers and individuals living in a contaminated zone). For the moment, however, there are no reliable data on the nature, severity, frequency and distribution of psychological problems in the target populations. The factors that must be taken into account when evaluating the psychological and social consequences of the accident on residents of the contaminated zones include the harsh social and economic situation, the diversity of the available compensation systems, the effects of evacuation and resettlement (approximately 100,000 additional people were resettled in the years following the accident), and the effects of lifestyle limitations (e.g., modification of nutrition).
Principles of Prevention and Guidelines
Safety principles and guidelines
Industrial and medical use of radioactive sources
While it is true that the major radiation accidents reported have all occurred at nuclear power plants, the use of radioactive sources in other settings has nevertheless resulted in accidents with serious consequences for workers or the general public. The prevention of accidents such as these is essential, especially in light of the disappointing prognosis in cases of high-dose exposure. Prevention depends on proper worker training and on the maintenance of a comprehensive life-cycle inventory of radioactive sources which includes information on both the sources’ nature and location. The IAEA has established a series of safety guidelines and recommendations for the use of radioactive sources in industry, medicine and research (Safety Series No. 102). The principles in question are similar to those presented below for nuclear power plants.
Safety in nuclear power plants (IAEA Safety Series No. 75, INSAG-3)
The goal here is to protect both humans and the environment from the emission of radioactive materials under any circumstance. To this end, it is necessary to apply a variety of measures throughout the design, construction, operation and decommissioning of nuclear power plants.
The safety of nuclear power plants is fundamentally dependent on the “defence in depth” principle—that is, the redundancy of systems and devices designed to compensate for technical or human errors and deficiencies. Concretely, radioactive materials are separated from the environment by a series of successive barriers. In nuclear power production reactors, the last of these barriers is the containment structure (absent on the Chernobyl site but present at Three Mile Island). To avoid the breakdown of these barriers and to limit the consequences of breakdowns, the following three safety measures should be practised throughout the power plant’s operational life: control of the nuclear reaction, cooling of fuel, and containment of radioactive material.
Another essential safety principle is “operating experience analysis”—that is, using information gleaned from events, even minor ones, occurring at other sites to increase the safety of an existing site. Thus, analysis of the Three Mile Island and Chernobyl accidents has resulted in the implementation of modifications designed to ensure that similar accidents do not occur elsewhere.
Finally, it should be noted that significant efforts have been expended to promote a culture of safety, that is, a culture that is continually responsive to safety concerns related to the plant’s organization, activities and practices, as well as to individual behaviour. To increase the visibility of incidents and accidents involving nuclear power plants, an international scale of nuclear events (INES), identical in principle to scales used to measure the severity of natural phenomena such as earthquakes and wind, has been developed (table 12). This scale is not however suitable for the evaluation of a site’s safety or for performing international comparisons.
Table 13. International scale of nuclear incidents
|
Level |
Offsite |
Onsite |
Protective structure |
|
7—Major accident |
Major emission, |
||
|
6—Serious accident |
Significant emission, |
||
|
5—Accident |
Limited emission, |
Serious damage to |
|
|
4—Accident |
Low emission, public |
Damage to reactors |
|
|
3—Serious incident |
Very low emission, |
Serious |
Accident barely avoided |
|
2—Incident |
Serious contamination |
Serious failures of safety measures |
|
|
1—Abnormality |
Abnormality beyond |
||
|
0—Disparity |
No significance from |
Principles of the protection of the general public from exposure to radiation
In cases involving the potential exposure of the general public, it may be necessary to apply protective measures designed to prevent or limit exposure to ionizing radiation; this is particularly important if deterministic effects are to be avoided. The first measures which should be applied in emergency are evacuation, sheltering and administration of stable iodine. Stable iodine should be distributed to exposed populations, since this will saturate the thyroid and inhibit its uptake of radioactive iodine. To be effective, however, thyroid saturation must occur before or soon after the start of exposure. Finally, temporary or permanent resettlement, decontamination, and control of agriculture and food may eventually be necessary.
Each of these countermeasures has its own “action level” (table 14), not to be confused with the ICRP dose limits for workers and the general public, developed to ensure adequate protection in cases of non-accidental exposure (ICRP 1991).
Table 14. Examples of generic intervention levels for protective measures for general population
|
Protective measure |
Intervention level (averted dose) |
|
Emergency |
|
|
Containment |
10 mSv |
|
Evacuation |
50 mSv |
|
Distribution of stable iodine |
100 mGy |
|
Delayed |
|
|
Temporary resettlement |
30 mSv in 30 days; 10 mSv in the next 30 days |
|
Permanent resettlement |
1 Sv lifetime |
Source: IAEA 1994.
Research Needs and Future Trends
Current safety research concentrates on improving the design of nuclear power-generating reactors—more specifically, on the reduction of the risk and effects of core meltdown.
The experience gained from previous accidents should lead to improvements in the therapeutic management of seriously irradiated individuals. Currently, the use of bone marrow cell growth factors (haematopoietic growth factors) in the treatment of radiation-induced medullary aplasia (developmental failure) is being investigated (Thierry et al. 1995).
The effects of low doses and dose rates of ionizing radiation remains unclear and needs to be clarified, both from a purely scientific point of view and for the purposes of establishing dose limits for the general public and for workers. Biological research is necessary to elucidate the carcinogenic mechanisms involved. The results of large-scale epidemiological studies, especially those currently under way on workers at nuclear power plants, should prove useful in improving the accuracy of cancer risk estimates for populations exposed to low doses or dose rates. Studies on populations which are or have been exposed to ionizing radiation due to accidents should help further our understanding of the effects of higher doses, often delivered at low dose rates.
The infrastructure (organization, equipment and tools) necessary for the timely collection of data essential for the evaluation of the health effects of radiation accidents must be in place well in advance of the accident.
Finally, extensive research is necessary to clarify the psychological and social effects of radiation accidents (e.g., the nature and frequency of, and risk factors for, pathological and non-pathological post-traumatic psychological reactions). This research is essential if the management of both occupationally and non-occupationally exposed populations is to be improved.