- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Healthcare Workers and Infectious Diseases
Assessment of Heat Stress and Heat Stress Indices
Heat stress occurs when a person’s environment (air temperature, radiant temperature, humidity and air velocity), clothing and activity interact to produce a tendency for body temperature to rise. The body’s thermoregulatory system then responds in order to increase heat loss. This response can be powerful and effective, but it can also produce a strain on the body which leads to discomfort and eventually to heat illness and even death. It is important therefore to assess hot environments to ensure the health and safety of workers.
Heat stress indices provide tools for assessing hot environments and predicting likely thermal strain on the body. Limit values based upon heat stress indices will indicate when that strain is likely to become unacceptable.
The mechanisms of heat stress are generally understood, and work practices for hot environments are well established. These include knowledge of the warning signs of heat stress, acclimatization programmes and water replacement. There are still many casualties, however, and these lessons seem to have to be relearned.
In 1964, Leithead and Lind described an extensive survey and concluded that heat disorders occur for one or more of the following three reasons:
- the existence of factors such as dehydration or lack of acclimatization
- the lack of proper appreciation of the dangers of heat, either on the part of the supervising authority or of the individuals at risk
- accidental or unforeseeable circumstances leading to exposure to very high heat stress.
They concluded that many deaths can be attributed to neglect and lack of consideration and that even when disorders do occur, much can be done if all the requirements for the correct and prompt remedial treatment are available.
Heat Stress Indices
A heat stress index is a single number which integrates the effects of the six basic parameters in any human thermal environment such that its value will vary with the thermal strain experienced by the person exposed to a hot environment. The index value (measured or calculated) can be used in design or in work practice to establish safe limits. Much research has gone into determining the definitive heat stress index, and there is discussion about which is best. For example, Goldman (1988) presents 32 heat stress indices, and there are probably at least double that number used throughout the world. Many indices do not consider all six basic parameters, although all have to take them into conside ration in application. The use of indices will depend upon individual contexts, hence the production of so many. Some indices are inadequate theoretically but can be justified for specific applications based on experience in a particular industry.
Kerslake (1972) notes that “It is perhaps self evident that the way in which the environmental factors should be combined must depend on the properties of the subject exposed to them, but none of the heat stress indices in current use make formal allowance for this”. The recent surge in standardization (e.g., ISO 7933 (1989b) and ISO 7243 (1989a)) has led to pressure to adopt similar indices worldwide. It will be necessary, however, to gain experience with the use of any new index.
Most heat stress indices consider, directly or indirectly, that the main strain on the body is due to sweating. For example, the more sweating required to maintain heat balance and internal body temperature, the greater the strain on the body. For an index of heat stress to represent the human thermal environment and predict heat strain, a mechanism is required to estimate the capacity of a sweating person to lose heat in the hot environment.
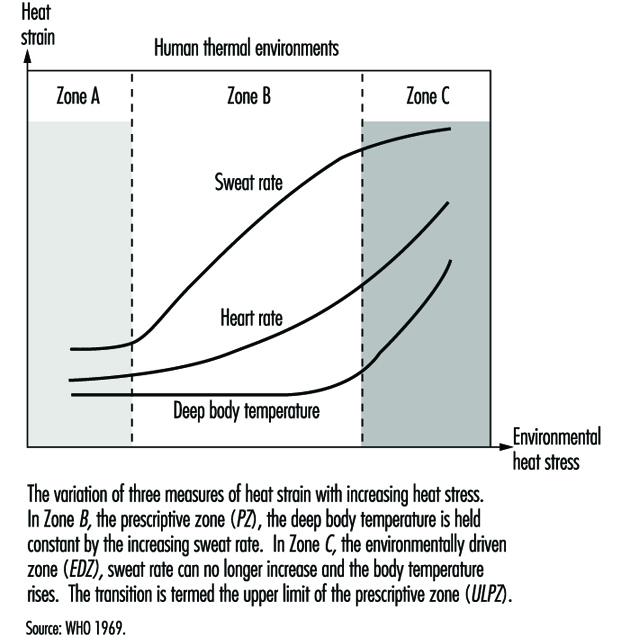
An index related to evaporation of sweat to the environment is useful where persons maintain internal body temperature essentially by sweating. These conditions are generally said to be in the prescriptive zone (WHO 1969). Hence deep body temperature remains relatively constant while heart rate and sweat rate rise with heat stress. At the upper limit of the prescriptive zone (ULPZ), thermoregulation is insufficient to maintain heat balance, and body temperature rises. This is termed the environmentally driven zone (WHO 1969). In this zone heat storage is related to internal body temperature rise and can be used as an index to determine allowable exposure times (e.g., based on a predicted safety limit for “core” temperature of 38 °C; see Figure 1).
Figure 1. Calculated distributions of water in the extracellular compartment (ECW) and intracellular compartment (ICW) before and after 2 h of exercise dehydration at 30°C room temperature.
Heat stress indices can be conveniently categorized as rational, empirical or direct. Rational indices are based upon calculations involving the heat balance equation; empirical indices are based on establishing equations from the physiological responses of human subjects (e.g., sweat loss); and direct indices are based on the measurement (usually temperature) of instruments used to simulate the response of the human body. The most influential and widely used heat stress indices are described below.
Rational indices
The Heat Stress Index (HSI)
The Heat Stress Index is the ratio of evaporation required to maintain heat balance (Ereq) to the maximum evaporation that could be achieved in the environment (Emax), expressed as a percentage (Belding and Hatch 1955). Equations are provided in table 1.
Table 1. Equations used in the calculation of the Heat Stress Index (HSI) and Allowable Exposure Times (AET)
|
|
|
|
Clothed |
Unclothed |
|
(1) Radiation loss (R)
|
|
for |
4.4 |
7.3 |
|
(2) Convection loss (C)
|
|
for |
4.6 |
7.6
|
|
(3) Maximum evaporative loss (
|
|
for |
7.0 |
11.7
|
|
(4) Required evaporation loss (
|
|
|
|
|
|
(5) Heat stress index (HSI) |
|
|
|
|
|
(6) Allowable exposure time (AET) |
|
|
|
|
where: M = metabolic power; ![]() = air temperature;
= air temperature; ![]() = radiant temperature;
= radiant temperature; ![]() = partial vapour pressure; v = air velocity
= partial vapour pressure; v = air velocity
The HSI as an index therefore is related to strain, essentially in terms of body sweating, for values between 0 and 100. At HSI = 100, evaporation required is the maximum that can be achieved, and thus represents the upper limit of the prescriptive zone. For HSI>100, there is body heat storage, and allowable exposure times are calculated based on a 1.8 ºC rise in core temperature (heat storage of 264 kJ). For HSI0 there is mild cold strain—for example, when workers recover from heat strain (see table 2).
Table 2. Interpretation of Heat Stress Index (HSI) values
|
HSI |
Effect of eight hour exposure |
|
–20 |
Mild cold strain (e.g. recovery from heat exposure). |
|
0 |
No thermal strain |
|
10-30 |
Mild to moderate heat strain. Little effect on physical work but possible effect on skilled work |
|
40-60 |
Severe heat strain, involving threat to health unless physically fit. Acclimatization required |
|
70-90 |
Very severe heat strain. Personnel should be selected by medical examination. Ensure adequate water and salt intake |
|
100 |
Maximum strain tolerated daily by fit acclimatized young men |
|
Over 100 |
Exposure time limited by rise in deep body temperature |
An upper limit of 390 W/m2 is assigned to Emax (sweat rate of 1 l/h, taken to be the maximum sweat rate maintained over 8 h). Simple assumptions are made about the effects of clothing (long-sleeved shirt and trousers), and the skin temperature is assumed to be constant at 35ºC.
The Index of Thermal Stress (ITS)
Givoni (1963, 1976) provided the Index of Thermal Stress, which was an improved version of the Heat Stress Index. An important improvement is the recognition that not all sweat evaporates. (See “I. Index of thermal stress” in Case Study: Heat indices.)
Required sweat rate
A further theoretical and practical development of the HSI and ITS was the required sweat rate (SWreq) index (Vogt et al. 1981). This index calculated sweating required for heat balance from an improved heat balance equation but, most importantly, also provided a practical method of interpretation of calculations by comparing what is required with what is physiologically possible and acceptable in humans.
Extensive discussions and laboratory and industrial evaluations (CEC 1988) of this index led to it being accepted as International Standard ISO 7933 (1989b). Differences between observed and predicted responses of workers led to the inclusion of cautionary notes concerning methods of assessing dehydration and evaporative heat transfer through clothing in its adoption as a proposed European Standard (prEN-12515). (See “II. Required sweat rate” in Case Study: Heat indices.)
Interpretation of SWreq
Reference values—in terms of what is acceptable, or what persons can achieve—are used to provide a practical interpretation of calculated values (see table 3).
Table 3. Reference values for criteria of thermal stress and strain (ISO 7933, 1989b)
|
Criteria |
Non-acclimatized subjects |
Acclimatized subjects |
|||
|
Warning |
Danger |
Warning |
Danger |
||
|
Maximum skin wettedness |
|||||
|
wmax |
0.85 |
0.85 |
1.0 |
1.0 |
|
|
Maximum sweat rate |
|||||
|
Rest (M 65 Wm–2 ) |
SWmax Wm–2 gh–1 |
100 |
150 |
200 |
300 |
|
260 |
390 |
520 |
780 |
||
|
Work (M≥65 Wm–2 ) |
SWmax Wm–2 gh–1 |
200 |
250 |
300 |
400 |
|
520 |
650 |
780 |
1,040 |
||
|
Maximum heat storage |
|||||
|
Qmax |
Whm–2 |
50 |
60 |
50 |
60 |
|
Maximum water loss |
|||||
|
Dmax |
Whm–2 g |
1,000 |
1,250 |
1,500 |
2,000 |
|
2,600 |
3,250 |
3,900 |
5,200 |
||
First, a prediction of skin wettedness (Wp), evaporation rate (Ep) and sweat rate (SWp) are made. Essentially, if what is calculated as required can be achieved, then these are predicted values (e.g., SWp = SWreq). If they cannot be achieved, the maximum values can be taken (e.g., SWp=SWmax). More detail is given in a decision flow chart (see figure 2).
Figure 2. Decision flow chart for ![]() (required sweat rate).
(required sweat rate).
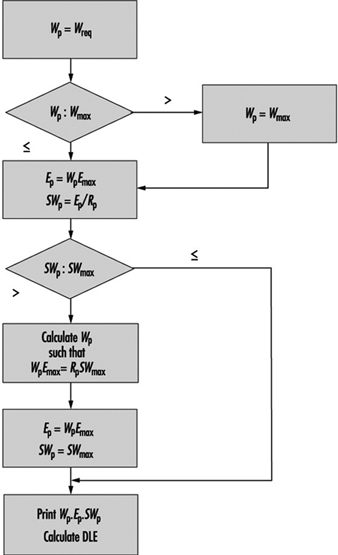
If required sweat rate can be achieved by persons and it will not cause unacceptable water loss, then there is no limit due to heat exposure over an 8-hour shift. If not, the duration-limited exposures (DLE) are calculated from the following:
When Ep = Ereq and SWp = Dmax/8, then DLE = 480 mins and SWreq can be used as a heat stress index. If the above are not satisfied, then:
DLE1 = 60Qmax/( Ereq –Ep)
DLE2 = 60Dmax/SWp
DLE is the lower of DLE1 and DLE2. Fuller details are given in ISO 7933 (1989b).
Other rational indices
The SWreq index and ISO 7933 (1989) provide the most sophisticated rational method based on the heat balance equation, and they were major advances. More developments with this approach can be made; however, an alternative approach is to use a thermal model. Essentially, the New Effective Temperature (ET*) and Standard Effective Temperature (SET) provide indices based on the two-node model of human thermoregulation (Nishi and Gagge 1977). Givoni and Goldman (1972, 1973) also provide empirical prediction models for the assessment of heat stress.
Empirical indices
Effective temperature andcorrected effective temperature
The Effective Temperature index (Houghton and Yaglou 1923) was originally established to provide a method for determining the relative effects of air temperature and humidity on comfort. Three subjects judged which of two climatic chambers was warmer by walking between the two. Using different combinations of air temperature and humidity (and later other parameters), lines of equal comfort were determined. Immediate impressions were made so the transient response was recorded. This had the effect of over-emphasizing the effect of humidity at low temperatures and underestimating it at high temperatures (when compared with steady-state responses). Although originally a comfort index, the use of the black globe temperature to replace dry bulb temperature in the ET nomograms provided the Corrected Effective Temperature (CET) (Bedford 1940). Research reported by Macpherson (1960) suggested that the CET predicted physiological effects of increasing mean radiant temperature. ET and CET are now rarely used as comfort indices but have been used as heat stress indices. Bedford (1940) proposed CET as an index of warmth, with upper limits of 34ºC for “reasonable efficiency” and 38.6ºC for tolerance. Further investigation, however, showed that ET had serious disadvantages for use as a heat stress index, which led to the Predicted Four Hour Sweat Rate (P4SR) index.
Predicted Four Hour Sweat Rate
The Predicted Four Hour Sweat Rate (P4SR) index was established in London by McArdle et al. (1947) and evaluated in Singapore in 7 years of work summarized by Macpherson (1960). It is the amount of sweat secreted by fit, acclimatized young men exposed to the environment for 4 hours while loading guns with ammunition during a naval engagement. The single number (index value) which summarizes the effects of the six basic parameters is an amount of sweat from the specific population, but it should be used as an index value and not as an indication of an amount of sweat in an individual group of interest.
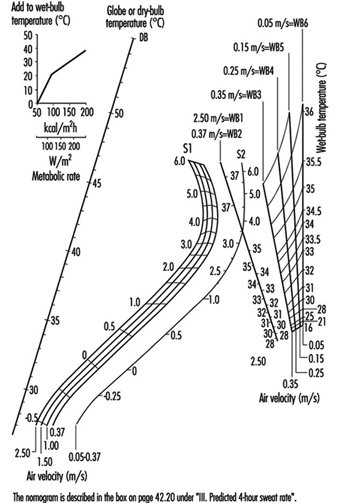
It was acknowledged that outside of the prescriptive zone (e.g., P4SR>5 l) sweat rate was not a good indicator of strain. The P4SR nomograms (figure 3) were adjusted to attempt to account for this. The P4SR appears to have been useful under the conditions for which it was derived; however, the effects of clothing are over-simplified and it is most useful as a heat storage index. McArdle et al. (1947) proposed a P4SR of 4.5 l for a limit where no incapacitation of any fit, acclimatized young men occurred.
Figure 3. Nomogram for the prediction of the "predicted 4-hour sweat rate" (P4SR).
Heart rate prediction as an index
Fuller and Brouha (1966) proposed a simple index based on the prediction of heart rate (HR) in beats per minute. The relationship as originally formulated with metabolic rate in BTU/h and partial vapour pressure in mmHg provided a simple prediction of heart rate from (T + p), hence the T + p index.
Givoni and Goldman (1973) also provide equations for changing heart rate with time and also corrections for degree of acclimatization of subjects, which are given in Case Study" Heat Indices under “IV. Heart rate”.
A method of work and recovery heart rate is described by NIOSH (1986) (from Brouha 1960 and Fuller and Smith 1980, 1981). Body temperature and pulse rates are measured during recovery following a work cycle or at specified times during the working day. At the end of a work cycle the worker sits on a stool, oral temperature is taken and the following three pulse rates are recorded:
P1—pulse rate counted from 30 seconds to 1 minute
P2—pulse rate counted from 1.5 to 2 minutes
P3—pulse rate counted from 2.5 to 3 minutes
The ultimate criterion in terms of heat strain is an oral temperature of 37.5 ºC.
If P3≤90 bpm and P3–P1 = 10 bpm, this indicates work level is high but there is little increase in body temperature. If P3>90 bpm and P3–P110 bpm, the stress (heat + work) is too high and action is needed to redesign work.
Vogt et al. (1981) and ISO 9886 (1992) provide a model (table 4) using heart rate for assessing thermal environments:
Table 4. Model using heart rate to assess heat stress
|
Total heart rate |
Activity level |
|
HR0 |
Rest (thermal neutrality) |
|
HR0 + HRM |
Work |
|
HR0 + HRS |
Static exertion |
|
HR0 + HRt |
Thermal strain |
|
HR0 + HRN |
Emotion (psychological) |
|
HR0 + HRe |
Residual |
Based on Vogt et al. (1981) and ISO 9886 (1992).
The component of thermal strain (possible heat stress index) can be calculated from:
HRt = HRr–HR0
where HRr is heart rate after recovery and HR0 is the resting heart rate in a thermally neutral environment.
Direct Heat Stress Indices
The Wet Bulb Globe Temperature index
The Wet Bulb Globe Temperature (WBGT) index is by far the most widely used throughout the world. It was developed in a US Navy investigation into heat casualties during training (Yaglou and Minard 1957) as an approximation to the more cumbersome Corrected Effective Temperature (CET), modified to account for the solar absorptivity of green military clothing.
WBGT limit values were used to indicate when military recruits could train. It was found that heat casualties and time lost due to cessation of training in the heat were both reduced by using the WBGT index instead of air temperature alone. The WBGT index was adopted by NIOSH (1972), ACGIH (1990) and ISO 7243 (1989a) and is still proposed today. ISO 7243 (1989a), based on the WBGT index, provides a method easily used in a hot environment to provide a “fast” diagnosis. The specification of the measuring instruments is provided in the standard, as are WBGT limit values for acclimatized or non- acclimatized persons (see table 5). For example, for a resting acclimatized person in 0.6 clo, the limit value is 33ºC WBGT. The limits provided in ISO 7243 (1989a) and NIOSH 1972 are almost identical. Calculation of the WBGT index is given in section V of the accompanying Case Study: Heat Indices.
Table 5. WBGT reference values from ISO 7243 (1989a)
|
Metabolic rate M (Wm–2 ) |
Reference value of WBGT |
|||
|
Person acclimatized to |
Person not acclimatized to |
|||
|
0. Resting M≤65 |
33 |
32 |
||
|
1. 65M≤130 |
30 |
29 |
||
|
2. 130M≤200 |
28 |
26 |
||
|
No sensible air movement |
Sensible air movement |
No sensible air movement |
Sensible air movement |
|
|
3. 200M260 |
25 |
26 |
22 |
23 |
|
4. M>260 |
23 |
25 |
18 |
20 |
Note: The values given have been established allowing for a maximum rectal temperature of 38°C for the persons concerned.
The simplicity of the index and its use by influential bodies has led to its widespread acceptance. Like all direct indices it has limitations when used to simulate human response, and should be used with caution in practical applications. It is possible to buy portable instruments which determine the WBGT index (e.g., Olesen 1985).
Physiological heat exposure limit (PHEL)
Dasler (1974, 1977) provides WBGT limit values based on a prediction of exceeding any two physiological limits (from experimental data) of impermissible strain. The limits are given by:
PHEL=(17.25×108–12.97M×106+18.61M2 ×103)×WBGT–5.36
This index therefore uses the WBGT direct index in the environmentally driven zone (see Figure 4), where heat storage can occur.
Wet globe temperature (WGT) index
The temperature of a wet black globe of appropriate size can be used as an index of heat stress. The principle is that it is affected by both dry and evaporative heat transfer, as is a sweating man, and the temperature can then be used, with experience, as a heat stress index. Olesen (1985) describes WGT as the temperature of a 2.5 inch (63.5 mm) diameter black globe covered with a damp black cloth. The temperature is read when equilibrium is reached after about 10 to 15 minutes of exposure. NIOSH (1986) describe the Botsball (Botsford 1971) as the simplest and most easily read instrument. It is a 3-inch (76.2 mm) copper sphere covered by a black cloth kept at 100% wettedness from a self-feeding water reservoir. The sensing element of a thermometer is located at the centre of the sphere, and the temperature is read on a (colour coded) dial.
A simple equation relating WGT to WBGT is:
WBGT = WGT + 2 ºC
for conditions of moderate radiant heat and humidity (NIOSH 1986), but of course this relationship cannot hold over a wide range of conditions.
The Oxford Index
Lind (1957) proposed a simple, direct index used for storage- limited heat exposure and based on a weighted summation of aspirated wet bulb temperature (Twb) and dry bulb temperature (Tdb):
WD = 0.85 Twb + 0.15 Tdb
Allowable exposure times for mine rescue teams were based on this index. It is widely applicable but is not appropriate where there is significant thermal radiation.
Working Practices for Hot Environments
NIOSH (1986) provides a comprehensive description of working practices for hot environments, including preventive medical practices. A proposal for medical supervision of individuals exposed to hot or cold environments is provided in ISO CD 12894 (1993). It should always be remembered that it is a basic human right, which was affirmed by the 1985 Declaration of Helsinki, that, when possible, persons can withdraw from any extreme environment without need of explanation. Where exposure does take place, defined working practices will greatly improve safety.
It is a reasonable principle in environmental ergonomics and in industrial hygiene that, where possible, the environmental stressor should be reduced at the source. NIOSH (1986) divides control methods into five types. These are presented in table 6.
Table 6. Working practices for hot environments
|
A. Engineering controls |
Example |
|
1. Reduce heat source |
Move away from workers or reduce temperature. Not always practicable. |
|
2. Convective heat control |
Modify air temperature and air movements. Spot coolers may be useful. |
|
3. Radiant heat control |
Reduce surface temperatures or place reflective shield between radiant source and workers. Change emissivity of surface. Use doors that open only when access required. |
|
4. Evaporative heat control |
Increase air movement, decrease water vapour pressure. Use fans or air conditioning. Wet clothing and blow air across person. |
|
B. Work and hygiene practices |
Example |
|
1. Limiting exposure time and/or |
Perform jobs at cooler times of day and year. Provide cool areas for rest and recovery. Extra personnel, worker freedom to interrupt work, increase water intake. |
|
2. Reduce metabolic heat load |
Mechanization. Redesign job. Reduce work time. Increase workforce. |
|
3. Enhance tolerance time |
Heat acclimatization program. Keep workers physically fit. Ensure water loss is replaced and maintain electrolyte balance if necessary. |
|
4. Health and safety training |
Supervisors trained in recognizing signs of heat illness and in first aid. Basic instruction to all personnel on personal precautions, use of protective equipment and effects of non-occupational factors (e.g. alcohol). Use of a “buddy” system. Contingency plans for treatment should be in place. |
|
5. Screening for heat intolerance |
History of previous heat illness. Physically unfit. |
|
C. Heat alert program |
Example |
|
1. In spring establish heat alert |
Arrange training course. Memos to supervisors to make checks of drinking fountains, etc. Check facilities, practices, readiness, etc. |
|
2. Declare heat alert in predicted |
Postpone non-urgent tasks. Increase workers, increase rest. Remind workers to drink. Improve working practices. |
|
D. Auxiliary body cooling and protective clothing |
|
|
Use if it is not possible to modify worker, work or environment and heat stress is still beyond limits. Individuals should be fully heat acclimatized and well trained in use and practice of wearing the protective clothing. Examples are water-cooled garments, air-cooled garments, ice-packet vests and wetted overgarments. |
|
|
E. Performance degradation |
|
|
It must be remembered that wearing protective clothing that is providing protection from toxic agents will increase heat stress. All clothing will interfere with activities and may reduce performance (e.g. reducing the ability to receive sensory information hence impairing hearing and vision for example). |
|
Source: NIOSH 1986.
There has been a great deal of military research into so-called NBC (nuclear, biological, chemical) protective clothing. In hot environments it is not possible to remove the clothing, and working practices are very important. A similar problem occurs for workers in nuclear power stations. Methods of cooling workers quickly so that they are able to perform again include sponging the outer surface of the clothing with water and blowing dry air over it. Other techniques include active cooling devices and methods for cooling local areas of the body. The transfer of military clothing technology to industrial situations is a new innovation, but much is known, and appropriate working practices can greatly reduce risk.
Table 7. Equations used in the calculation of the index and assessment method of ISO 7933 (1989b)
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]() for natural convection
for natural convection
![]()
![]()
![]()
![]()

![]()
![]()
![]()
![]()

![]()
or ![]() , for an approximation or when values are beyond limits for which the equation was derived.
, for an approximation or when values are beyond limits for which the equation was derived.
____________________________________________________________________________________
Table 8. Description of terms used in ISO 7933 (1989b)
|
Symbol |
Term |
Units |
|
|
fraction of skin surface involved in heat exchange by radiation |
ND |
|
C |
heat exchange on the skin by convection |
Wm−2 |
|
|
respiratory heat loss by convection |
Wm−2 |
|
E |
heat flow by evaporation at skin surface |
Wm−2 |
|
|
maximum evaporative rate which can be achieved with the skin completely wet |
Wm−2 |
|
|
required evaporation for thermal equilibrium |
Wm−2 |
|
|
respiratory heat loss by evaporation |
Wm−2 |
|
|
skin emissivity (0.97) |
ND |
|
|
reduction factor for sensible heat exchange due to clothing |
ND |
|
|
reduction factor for latent heat exchange |
ND |
|
|
ratio of the subject’s clothed to unclothed surface area |
ND |
|
|
convective heat transfer coefficient |
|
|
|
evaporative heat transfer coefficient |
|
|
|
radiative heat transfer coefficient |
|
|
|
basic dry thermal insulation of clothing |
|
|
K |
heat exchange on the skin by conduction |
Wm−2 |
|
M |
metabolic power |
Wm−2 |
|
|
partial vapour pressure |
kPa |
|
|
saturated vapour pressure at skin temperature |
kPa |
|
R |
heat exchange on the skin by radiation |
Wm−2 |
|
|
total evaporative resistance of limiting layer of air and clothing |
|
|
|
evaporative efficiency at required sweat rate |
ND |
|
|
required sweat rate for thermal equilibrium |
Wm−2 |
|
|
Stefan-Boltzman constant, |
|
|
|
air temperature |
|
|
|
mean radiant temperature |
|
|
|
mean skin temperature |
|
|
|
air velocity for a stationary subject |
|
|
|
relative air velocity |
|
|
W |
mechanical power |
Wm−2 |
|
|
skin wettedness |
ND |
|
|
skin wettedness required |
ND |
ND = non-dimensional.
Working Practices for Hot Environments
NIOSH (1986) provides a comprehensive description of working practices for hot environments, including preventive medical practices. A proposal for medical supervision of individuals exposed to hot or cold environments is provided in ISO CD 12894 (1993). It should always be remembered that it is a basic human right, which was affirmed by the 1985Declaration of Helsinki, that, when possible, persons can withdraw from any extreme environment without need of explanation. Where exposure does take place, defined working practices will greatly improve safety.
It is a reasonable principle in environmental ergonomics and in industrial hygiene that, where possible, the environmental stressor should be reduced at the source. NIOSH (1986) divides control methods into five types. These are presented in table 7.There has been a great deal of military research into so-called NBC (nuclear, biological, chemical) protective clothing. In hot environments it is not possible to remove the clothing, and working practices are very important. A similar problem occurs for workers in nuclear power stations. Methods of cooling workers quickly so that they are able to perform again include sponging the outer surface of the clothing with water and blowing dry air over it. Other techniques include active cooling devices and methods for cooling local areas of the body. The transfer of military clothing technology to industrial situations is a new innovation, but much is known, and appropriate working practices can greatly reduce risk.
Assessment of a Hot Environment Using ISO Standards
The following hypothetical example demonstrates how ISO standards can be used in the assessment of hot environments (Parsons 1993):
Workers in a steel mill perform work in four phases. They don clothing and perform light work for 1 hour in a hot radiant environment. They rest for 1 hour, then perform the same light work for an hour shielded from the radiant heat. They then perform work involving a moderate level of physical activity in a hot radiant environment for 30 minutes.
ISO 7243 provides a simple method for monitoring the environment using the WBGT index. If the calculated WBGT levels are less than the WBGT reference values given in the standard, then no further action is required. If the levels exceed the reference values (table 6) then the strain on the workers must be reduced. This can be achieved by engineering controls and working practices. A complementary or alternative action is to conduct an analytical assessment according to ISO 7933.
The WBGT values for the work are presented in table 9 and were measured according to the specifications given in ISO 7243 and ISO 7726. The environmental and personal factors relating to the four phases of the work are presented in table 10.
Table 9. WBGT values (°C) for four work phases
|
Work phase (minutes) |
WBGT = WBGTank + 2 WBGTabd + WBGThd |
WBGT reference |
|
0–60 |
25 |
30 |
|
60–90 |
23 |
33 |
|
90–150 |
23 |
30 |
|
150–180 |
30 |
28 |
Table 10. Basic data for the analytical assessment using ISO 7933
|
Work phase (minutes) |
ta (°C) |
tr (°C) |
Pa (Kpa) |
v (ms–1 ) |
clo (clo) |
Act (Wm–2 ) |
|
0–60 |
30 |
50 |
3 |
0.15 |
0.6 |
100 |
|
60–90 |
30 |
30 |
3 |
0.05 |
0.6 |
58 |
|
90–150 |
30 |
30 |
3 |
0.20 |
0.6 |
100 |
|
150–180 |
30 |
60 |
3 |
0.30 |
1.0 |
150 |
It can be seen that for part of the work the WBGT values exceed those of the reference values. It is concluded that a more detailed analysis is required.
The analytical assessment method presented in ISO 7933 was performed using the data presented in table 10 and the computer program listed in the annex of the standard. The results for acclimatized workers in terms of alarm level are presented in table 11.
Table 11. Analytical assessment using ISO 7933
|
Work phase |
Predicted values |
Duration |
Reason for |
||
|
tsk (°C) |
W (ND) |
SW (gh–1 ) |
|||
|
0–60 |
35.5 |
0.93 |
553 |
423 |
Water loss |
|
60–90 |
34.6 |
0.30 |
83 |
480 |
No limit |
|
90–150 |
34.6 |
0.57 |
213 |
480 |
No limit |
|
150–180 |
35.7 |
1.00 |
566 |
45 |
Body temperature |
|
Overall |
— |
0.82 |
382 |
480 |
No limit |
An overall assessment therefore predicts that unacclimatized workers suitable for the work could carry out an 8-hour shift without undergoing unacceptable (thermal) physiological strain. If greater accuracy is required, or individual workers are to be assessed, then ISO 8996 and ISO 9920 will provide detailed information concerning metabolic heat production and clothing insulation. ISO 9886 describes methods for measuring physiological strain on workers and can be used to design and assess environments for specific workforces. Mean skin temperature, internal body temperature, heart rate and mass loss will be of interest in this example. ISO CD 12894 provides guidance on medical supervision of an investigation.
The Physical Basis of Work in Heat
Thermal Exchanges
The human body exchanges heat with its environment by various pathways: conduction across the surfaces in contact with it, convection and evaporation with the ambient air, and radiation with the neighbouring surfaces.
Conduction
Conduction is the transmission of heat between two solids in contact. Such exchanges are observed between the skin and clothing, footwear, pressure points (seat, handles), tools and so on. In practice, in the mathematical calculation of thermal balance, this heat flow by conduction is approximated indirectly as a quantity equal to the heat flow by convection and radiation which would take place if these surfaces were not in contact with other materials.
Convection
Convection is the transfer of heat between the skin and the air surrounding it. If the skin temperature, tsk, in units of degrees Celsius (°C), is higher than the air temperature (ta), the air in contact with the skin is heated and consequently rises. Air circulation, known as natural convection, is thus established at the surface of the body. This exchange becomes greater if the ambient air passes over the skin at a certain speed: the convection becomes forced. The heat flow exchanged by convection, C, in units of watts per square metre (W/m2), can be estimated by:
C = hc FclC (tsk - ta)
where hc is the coefficient of convection (W/°C m2), which is a function of the difference between tsk and ta in the case of natural convection, and of the air velocity Va (in m/s) in forced convection; FclC is the factor by which clothing reduces convection heat exchange.
Radiation
Every body emits electromagnetic radiation, the intensity of which is a function of the fourth power of its absolute temperature T (in degrees Kelvin—K). The skin, whose temperature may be between 30 and 35°C (303 and 308K), emits such radiation, which is in the infrared zone. Moreover, it receives the radiation emitted by neighbouring surfaces. The thermal flow exchanged by radiation, R (in W/m2), between the body and its surroundings may be described by the following expression:
![]()
where:
s is the universal constant of radiation (5.67 × 10-8 W/m2 K4)
e is the emissivity of the skin, which, for infrared radiation, is equal to 0.97 and independent of the wavelength, and for solar radiation is about 0.5 for the skin of a White subject and 0.85 for the skin of a Black subject
AR/AD is the fraction of the body surface taking part in the ex- changes, which is of the order of 0.66, 0.70 or 0.77, depending upon whether the subject is crouching, seated or standing
FclR is the factor by which clothing reduces radiation heat exchange
Tsk (in K) is the mean skin temperature
Tr (in K) is the mean radiant temperature of the environment —that is, the uniform temperature of a black mat sphere of large diameter that would surround the subject and would exchange with it the same quantity of heat as the real environment.
This expression may be replaced by a simplified equation of the same type as that for exchanges by convection:
R = hr (AR/AD) FclR (tsk - tr)
where hr is the coefficient of exchange by radiation (W/°C m2).
Evaporation
Every wet surface has on it a layer of air saturated with water vapour. If the atmosphere itself is not saturated, the vapour diffuses from this layer towards the atmosphere. The layer then tends to be regenerated by drawing on the heat of evaporation (0.674 Watt hour per gram of water) at the wet surface, which cools. If the skin is entirely covered with sweat, evaporation is maximal (Emax) and depends only on the ambient conditions, according to the following expression:
Emax = he Fpcl (Psk,s - Pa)
where:
he is the coefficient of exchange by evaporation (W/m2kPa)
Psk,s is the saturated pressure of water vapour at the temperature of the skin (expressed in kPa)
Pa is the ambient partial pressure of water vapour (expressed in kPa)
Fpcl is the factor of reduction of exchanges by evaporation due to clothing.
Thermal insulation of clothing
A correction factor operates in the calculation of heat flow by convection, radiation and evaporation so as to take account of clothing. In the case of cotton clothing, the two reduction factors FclC and FclR may be determined by:
Fcl = 1/(1+(hc+hr)Icl)
where:
hc is the coefficient of exchange by convection
hr is the coefficient of exchange by radiation
Icl is the effective thermal isolation (m2/W) of clothing.
As regards the reduction of heat transfer by evaporation, the correction factor Fpcl is given by the following expression:
Fpcl = 1/(1+2.22hc Icl)
The thermal insulation of the clothing Icl is expressed in m2/W or in clo. An insulation of 1 clo corresponds to 0.155 m2/W and is provided, for example, by normal town wear (shirt, tie, trousers, jacket, etc.).
ISO standard 9920 (1994) gives the thermal insulation provided by different combinations of clothing. In the case of special protective clothing that reflects heat or limits permeability to vapour under conditions of heat exposure, or absorbs and insulates under conditions of cold stress, individual correction factors must be used. To date, however, the problem remains poorly understood and the mathematical predictions remain very approximate.
Evaluation of the Basic Parameters of the Work Situation
As seen above, thermal exchanges by convection, radiation and evaporation are a function of four climatic parameters—the air temperature ta in °C, the humidity of the air expressed by its partial vapour pressure Pa in kPa, the mean radiant temperature tr in °C, and the air velocity Va in m/s. The appliances and methods for measuring these physical parameters of the environment are the subject of ISO standard 7726 (1985), which describes the different types of sensor to use, specifies their range of measurement and their accuracy, and recommends certain measurement procedures. This section summarizes part of the data of that standard, with particular reference to the conditions of use of the most common appliances and apparatus.
Air temperature
The air temperature (ta) must be measured independent of any thermal radiation; the accuracy of the measurement should be ±0.2ºC within the range of 10 to 30ºC, and ±0.5 °C outside that range.
There are numerous types of thermometers on the market. Mercury thermometers are the most common. Their advantage is accuracy, provided that they have been correctly calibrated originally. Their main disadvantages are their lengthy response time and lack of automatic recording ability. Electronic thermometers, on the other hand, generally have a very short response time (5 s to 1 min) but may have calibration problems.
Whatever the type of thermometer, the sensor must be protected against radiation. This is generally ensured by a hollow cylinder of shiny aluminium surrounding the sensor. Such protection is ensured by the psychrometer, which will be mentioned in the next section.
Partial pressure of water vapour
The humidity of the air may be characterized in four different ways:
1. the dewpoint temperature: the temperature to which the air must be cooled to become saturated with humidity (td, °C)
2. the partial pressure of water vapour: the fraction of atmospheric pressure due to water vapour (Pa, kPa)
3. the relative humidity (RH), which is given by the expression:
RH = 100·Pa/PS,ta
where PS,ta is the saturated vapour pressure associated with the air temperature
4. the wet bulb temperature (tw), which is the lowest temperature attained by a wet sleeve protected against radiation and ventilated at more than 2 m/s by the ambient air.
All these values are connected mathematically.
The saturated water vapour pressure PS,t at any temperature t is given by:
![]()
while the partial pressure of water vapour is connected to the temperature by:
Pa = PS,tw - (ta - tw)/15
where PS,tw is the saturated vapour pressure at the wet bulb temperature.
The psychrometric diagram (figure 1) allows all these values to be combined. It comprises:
Figure 1. Psychrometric diagram.
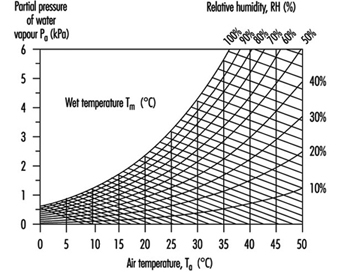
- in the y axis, the scale of partial pressure of water vapour Pa, expressed in kPa
- in the x axis, the scale of air temperature
- the curves of constant relative humidity
- the oblique straight lines of constant wet bulb temperature.
- The parameters of humidity most often used in practice are:
- the relative humidity, measured by means of hygrometers or more specialized electronic appliances
- the wet bulb temperature, measured by means of the psychrometer; from this is derived the partial pressure of water vapour, which is the parameter most used in analysing thermal balance
The range of measurement and the accuracy recommended are 0.5 to 6 kPa and ±0.15 kPa. For measurement of the wet bulb temperature, the range extends from 0 to 36ºC, with an accuracy identical with that of the air temperature. As regards hygrometers for measuring relative humidity, the range extends from 0 to 100%, with an accuracy of ±5%.
Mean radiant temperature
The mean radiant temperature (tr) has been defined previously; it can be determined in three different ways:
1. from the temperature measured by the black sphere thermometer
2. from the plane radiant temperatures measured along three perpendicular axes
3. by calculation, integrating the effects of the different sources of radiation.
Only the first technique will be reviewed here.
The black sphere thermometer consists of a thermal probe, the sensitive element of which is placed at the centre of a completely closed sphere, made of a metal that is a good conductor of heat (copper) and painted matt black so as to have a coefficient of absorption in the infrared zone close to 1.0. The sphere is positioned in the workplace and subjected to exchanges by convection and radiation. The temperature of the globe (tg) then depends on the mean radiant temperature, the air temperature and the air velocity.
For a standard black globe 15 cm in diameter, the mean temperature of radiation can be calculated from the temperature of the globe on the basis of the following expression:
![]()
In practice, the need must be stressed to maintain the emissivity of the globe close to 1.0 by carefully repainting it matt black.
The main limitation of this type of globe is its long response time (of the order of 20 to 30 min, depending on the type of globe used and the ambient conditions). The measurement is valid only if the conditions of radiation are constant during this period of time, and this is not always the case in an industrial setting; the measurement is then inaccurate. These response times apply to globes 15 cm in diameter, using ordinary mercury thermometers. They are shorter if sensors of smaller thermal capacity are used or if the diameter of the globe is reduced. The equation above must therefore be modified to take account of this difference in diameter.
The WBGT index makes direct use of the temperature of the black globe. It is then essential to use a globe 15 cm in diameter. On the other hand, other indices make use of the mean radiant temperature. A smaller globe can then be selected to reduce the response time, provided that the equation above is modified to take account of it. ISO standard 7726 (1985) allows for an accuracy of ±2ºC in the measurement of tr between 10 and 40ºC, and ±5ºC outside that range.
Air velocity
The air velocity must be measured disregarding the direction of air flow. Otherwise, the measurement must be undertaken in three perpendicular axes (x, y and z) and the global velocity calculated by vectorial summation:
![]()
The range of measurements recommended by ISO standard 7726 extends from 0.05 to 2 m/s The accuracy required is 5%. It should be measured as a 1- or 3-min average value.
There are two categories of appliances for measuring air velo-city: anemometers with vanes, and thermal anemometers.
Vane anemometers
The measurement is carried out by counting the number of turns made by the vanes during a certain period of time. In this way the mean velocity during that period of time is obtained in a discontinuous manner. These anemometers have two main disadvantages:
- They are very directional and have to be oriented strictly in the direction of the air flow. When this is vague or unknown, measurements have to be taken in three directions at right angles.
- The range of measurement extends from about 0.3 m/s to 10 m/s. This limitation to low velocities is important when, for instance, it is a question of analysing a thermal comfort situation where it is generally recommended that a velocity of 0.25 m/s should not be exceeded. Although the range of measurement can extend beyond 10 m/s, it hardly falls below 0.3 or even 0.5 m/s, which greatly limits the possibilities of use in environments near to comfort, where the maximum permitted velocities are 0.5 or even 0.25 m/s.
Hot-wire anemometers
These appliances are in fact complementary to vane anemometers in the sense that their dynamic range extends essentially from 0 to 1 m/s. They are appliances giving an instantaneous estimate of speed at one point of space: it is therefore necessary to use mean values in time and space. These appliances are also often very directional, and the remarks above also apply. Finally, the measurement is correct only from the moment when the temperature of the appliance has reached that of the environment to be evaluated.
Grinding and Polishing
Adapted from the 3rd edition, Encyclopaedia of Occupational Health and Safety.
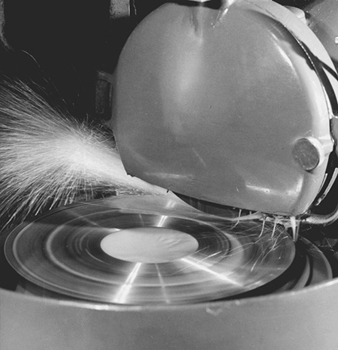
Grinding generally involves the use of a bonded abrasive to wear away parts of a workpiece. The aim is to give the work a certain shape, correct its dimensions, increase the smoothness of a surface or improve the sharpness of cutting edges. Examples include removal of sprues and rough edges from a foundry casting, removal of surface scale from metals before forging or welding and deburring of parts in sheet metal and machine shops. Polishing is used to remove surface imperfections such as tool marks. Buffing does not remove metal, but uses a soft abrasive blended in a wax or grease base to produce a high-lustre surface.
Grinding is the most comprehensive and diversified of all machining methods and is employed on many materials—predominantly iron and steel but also other metals, wood, plastics, stone, glass, pottery and so on. The term covers other methods of producing very smooth and glossy surfaces, such as polishing, honing, whetting and lapping.
The tools used are wheels of varying dimensions, grinding segments, grinding points, sharpening stones, files, polishing wheels, belts, discs and so on. In grinding wheels and the like, the abrasive material is held together by bonding agents to form a rigid, generally porous body. In the case of abrasive belts, the bonding agent holds the abrasive secured to a flexible base material. Buffing wheels are made from cotton or other textile disks sewn together.
The natural abrasives—natural corundum or emery (aluminium oxides), diamond, sandstone, flint and garnet—have been largely superseded by artificial abrasives including aluminium oxide (fused alumina), silicon carbide (carborundum) and synthetic diamonds. A number of fine-grained materials such as chalk, pumice, tripoli, tin putty and iron oxide are also used, especially for polishing and buffing.
Aluminium oxide is most widely used in grinding wheels, followed by silicon carbide. Natural and artificial diamonds are used for important special applications. Aluminium oxide, silicon carbide, emery, garnet and flint are used in grinding and polishing belts.
Both organic and inorganic bonding agents are used in grinding wheels. The main type of inorganic bonds are vitrified silicate and magnesite. Notable among organic bonding agents are phenol- or urea- formaldehyde resin, rubber and shellac. The vitrified bonding agents and phenolic resin are completely dominating within their respective groups. Diamond grinding wheels can also be metal bonded. The various bonding agents give the wheels different grinding properties, as well as different properties with regard to safety.
Abrasive and polishing belts and discs are composed of a flexible base of paper or fabric to which the abrasive is bonded by means of a natural or synthetic adhesive.
Different machines are used for different types of operations, such as surface grinding, cylindrical (including centreless) grinding, internal grinding, rough grinding and cutting. The two main types are: those where either the grinder or the work is moved by hand and machines with mechanical feeds and chucks. Common equipment types include: surface-type grinders; pedestal-type grinders, polishers and buffers; disk grinders and polishers; internal grinders; abrasive cut-off machines; belt polishers; portable grinders, polishers and buffers; and multiple polishers and buffers.
Hazards and Their Prevention
Bursting
The major injury risk in the use of grinding wheels is that the wheel may burst during grinding. Normally, grinding wheels operate at high speeds. There is a trend towards ever-increasing speeds. Most industrialized nations have regulations limiting the maximum speeds at which the various types of grinding wheels may be run.
The fundamental protective measure is to make the grinding wheel as strong as possible; the nature of the bonding agent is most important. Wheels with organic bonds, in particular phenolic resin, are tougher than those with inorganic bonds and more resistant to impacts. High peripheral speeds may be permissible for wheels with organic bonds.
Very high-speed wheels, in particular, often incorporate various types of reinforcement. For example, certain cup wheels are fitted with steel hubs to increase their strength. During rotation the major stress develops around the centre hole. To strengthen the wheel, the section around the centre hole, which takes no part in the grinding, can thus be made of an especially strong material which is not suitable for grinding. Large wheels with a centre section reinforced in this way are used particularly by the steel works for grinding slabs, billets and the like at speeds up to 80 m/s.
The most common method of reinforcing grinding wheels, however, is to include glass fibre fabric in their construction. Thin wheels, such as those used for cutting, may incorporate glass fibre fabric at the centre or at each side, while thicker wheels have a number of fabric layers depending on the thickness of the wheel.
With the exception of some grinding wheels of small dimensions, either all wheels or a statistical sampling of them must be given speed tests by the manufacturer. In tests the wheels are run over a certain period at a speed exceeding that permitted in grinding. Test regulations vary from country to country, but usually the wheel has to be tested at a speed 50% above the working speed. In some countries, regulations require special testing of wheels that are to operate at higher speeds than normal at a central testing institute. The institute may also cut specimens from the wheel and investigate their physical properties. Cutting wheels are subjected to certain impact tests, bending tests and so on. The manufacturer is also obliged to ensure that the grinding wheel is well balanced prior to delivery.
The bursting of a grinding wheel may cause fatal or very serious injuries to anyone in the vicinity and heavy damage to plant or premises. In spite of all precautions taken by the manufacturers, occasional wheel bursts or breaks may still occur unless proper care is exercised in their use. Precautionary measures include:
- Handling and storing. A wheel may become damaged or cracked during transit or handling. Moisture may attack the bonding agent in phenolic resin wheels, ultimately reducing their strength. Vitrified wheels may be sensitive to repeated temperature variations. Irregularly absorbed moisture may throw the wheel out of balance. Consequently, it is most important that wheels are carefully handled at all stages and kept in an orderly manner in a dry and protected place.
- Checking for cracks. A new wheel should be checked to ensure that it is undamaged and dry, most simply by tapping with a wooden mallet. A faultless vitrified wheel will give a clear ring, an organic bonded wheel a less ringing tone; but either can be differentiated from the cracked sound of a defective wheel. In case of doubt, the wheel should not be used and the supplier should be consulted.
- Testing. Before the new wheel is put into service, it should be tested at full speed with due precautions being observed. After wet grinding, the wheel should be run idle to eject the water; otherwise the water may collect at the bottom of the wheel and cause imbalance, which may result in bursting when the wheel is next used.
- Mounting. Accidents and breakages occur when grinding wheels are mounted on unsuitable apparatus—for example, on spindle ends of buffing machines. The spindle should be of adequate diameter but not so large as to expand the centre hole of the wheel; flanges should be not less than one-third the diameter of the wheel and made of mild steel or of similar material.
- Speed. In no circumstances should the maximum permissible operating speed specified by the makers be exceeded. A notice indicating the spindle speed should be fitted to all grinding machines, and the wheel should be marked with the maximum permissible peripheral speed and the corresponding number of revolutions for a new wheel. Special precautions are necessary with variable speed grinding machines and to ensure the fitting of wheels of appropriate permissible speeds in portable grinders.
- Work rest. Wherever practicable, rigidly mounted work rests of adequate dimensions should be provided. They should be adjustable and kept as close as possible to the wheel to prevent a trap in which the work might be forced against the wheel and break it or, more probable, catch and injure the operator’s hand.
- Guarding. Abrasive wheels should be provided with guards strong enough to contain the parts of a bursting wheel (see figure 1). Some countries have detailed regulations regarding the design of the guards and the materials to be used. In general, cast iron and cast aluminium are to be avoided. The grinding opening should be as small as possible, and an adjustable nose piece may be necessary. Exceptionally, where the nature of the work precludes the use of a guard, special protective flanges or safety chucks may be used. The spindles and tapered ends of double-ended polishing machines can cause entanglement accidents unless they are effectively guarded.
Figure 1. A well guarded, vitrified abrasive wheel mounted in a surface grinder and operating at a peripheral speed of 33 m/s
Eye injuries
Dust, abrasives, grains and splinters are a common hazard to the eyes in all dry-grinding operations. Effective eye protection by goggles or spectacles and fixed eye shields at the machine are essential; fixed eye shields are particularly useful when wheels are in intermittent use—for example, for tool grinding.
Fire
Grinding of magnesium alloys carries a high fire risk unless strict precautions are taken against accidental ignition and in the removal and drenching of dust. High standards of cleanliness and maintenance are required in all exhaust ducting to prevent risk of fire and also to keep ventilation working efficiently. Textile dust released from buffing operations is a fire hazard requiring good housekeeping and LEV.
Vibration
Portable and pedestal grinders carry a risk of hand-arm vibration syndrome (HAVS), also known as “white finger” from its most noticeable sign. Recommendations include limiting intensity and duration of exposure, redesigning tools, protective equipment and monitoring exposure and health.
Health hazards
Although modern grinding wheels do not themselves create the serious silicosis hazard associated in the past with sandstone wheels, highly dangerous silica dust may still be given off from the materials being ground—for example, sand castings. Certain resin-bonded wheels may contain fillers which create a dangerous dust. In addition, formaldehyde-based resins can emit formaldehyde during grinding. In any event, the volume of dust produced by grinding makes efficient LEV essential. It is more difficult to provide local exhaust for portable wheels, although some success in this direction has been achieved by use of low-volume, high-velocity capture systems. Prolonged work should be avoided and respiratory protective equipment provided if necessary. Exhaust ventilation is also required for most belt sanding, finishing, polishing and similar operations. With buffing in particular, combustible textile dust is a serious concern.
Protective clothing and good sanitary and washing facilities with showers should be provided, and medical supervision is desirable, especially for metal grinders.
Lathes
Adapted from the 3rd edition, Encyclopaedia of Occupational Health and Safety.
The important part lathes play in metalworking shops is best illustrated by the fact that 90 to 95% of the swarf (metal shavings) produced in the valves and fittings industry originates from lathes. About one-tenth of the accidents reported in this industry are due to lathes; this corresponds to one-third of all machine accidents. According to a study of the relative accident frequency per machine unit carried out in a plant manufacturing small precision parts and electrical equipment, lathes rank fifth after woodworking machines, metal-cutting saws, power presses and drilling machines. The need for protective measures on lathes is therefore beyond doubt.
Turning is a machine process in which the diameter of material is reduced by a tool with a special cutting edge. The cutting movement is produced by rotating the workpiece, and the feed and traverse movements are produced by the tool. By varying these three basic movements, and also by choosing the appropriate tool cutting-edge geometry and material, it is possible to influence the rate of stock removal, surface quality, shape of the chip formed and tool wear.
Structure of Lathes
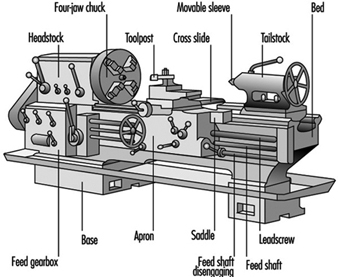
A typical lathe consists of:
- a bed or base with machined slideways for the saddle and tailstock
- a headstock mounted on the bed, with the spindle and chuck
- a feed gearbox attached to the front of the bed for transmitting the feed movement as a function of the cutting speed through the leadscrew or feed shaft and apron to the saddle
- a saddle (or carriage) carrying the cross slide which performs the traverse movement
- a toolpost mounted on the cross slide (see figure 1).
Figure 1. Lathes and similar machines
This basic model of a lathe can be infinitely varied, from the universal machine to the special automatic lathe designed for one type of work only.
The most important types of lathe are as follows:
- Centre lathe. This is the most frequently used turning machine. It corresponds to the basic model with horizontal turning axis. The work is held between centres, by a faceplate or in a chuck.
- Multiple-tool lathe. This enables several tools to be engaged at the same time.
- Turret lathe, capstan lathe. Machines of this type enable a workpiece to be machined by several tools which are engaged one after the other. The tools are held in the turret, which rotates for bringing them into cutting position. The turrets are generally of the disc or crown type, but there are also drum-type turret lathes.
- Copy-turning lathes. The desired shape is transmitted by tracer control from a template to the work.
- Automatic lathe. The various operations, including the change of the work, are automated. There are bar automatics and chucking automatics.
- Vertical lathe (boring and turning mill). The work turns about a vertical axis; it is clamped to a horizontal revolving table. This type of machine is generally used for machining large castings and forgings.
- NC and CNC lathes. All the aforementioned machines can be equipped with a numerical control (NC) or computer-assisted numerical control (CNC) system. The result is a semi-automated or fully automated machine which can be used rather universally, thanks to the great versatility and easy programmability of the control system.
The future development of the lathe will probably concentrate on control systems. Contact controls will be increasingly replaced by electronic control systems. As regards the latter, there is a trend in evolution from interpolation-programmed to memory-programmed controls. It is foreseeable in the long run that the use of increasingly efficient process computers will tend to optimize the machining process.
Accidents
Lathe accidents are generally caused by:
- disregard for safety regulations when the machines are installed in workshops (e.g., not enough space between machines, no power disconnect switch for each machine)
- missing guards or the absence of auxiliary devices (severe injuries have been caused to workers who tried to brake the spindle of their lathes by pressing one of their hands against unguarded belt pulleys and to operators who inadvertently engaged unguarded clutch levers or pedals; injuries due to flying chips because of the absence of hinged or sliding covers have also occurred)
- inadequately located control elements (e.g., a turner’s hand can be pierced by the tailstock centre if the pedal controlling the chuck is mistaken for the one controlling the hydraulic circuit of the tailstock centre movement)
- adverse conditions of work (i.e., shortcomings from the point of view of occupational physiology)
- lack of PPE or wearing unsuitable work clothing (severe and even fatal injuries have been caused to lathe operators who wore loose clothes or had long, free-hanging hair)
- insufficient instruction of personnel (an apprentice was fatally injured when he filed a short shaft which was fixed between centres and rotated by a cranked carrier on the spindle nose and a straight one on the shaft; the lathe carrier seized his left-hand sleeve, which was wrapped around the workpiece, dragging the apprentice violently into the lathe)
- poor work organization leading to the use of unsuitable equipment (e.g., a long bar was machined on a conventional production lathe; it was too long for this lathe, and it projected more than 1 m beyond the headstock; moreover, the chuck aperture was too large for the bar and was made up by inserting wooden wedges; when the lathe spindle started rotating, the free bar end bent by 45° and struck the operator’s head; the operator died during the following night)
- defective machine elements (e.g., a loose carrier pin in a clutch may cause the lathe spindle to start rotating while the operator is adjusting a workpiece in the chuck).
Accident Prevention
The prevention of lathe accidents starts at the design stage. Designers should give special attention to control and transmission elements.
Control elements
Each lathe must be equipped with a power disconnect (or isolating) switch so that maintenance and repair work may be carried out safely. This switch must disconnect the current on all poles, reliably cut the pneumatic and hydraulic power and vent the circuits. On large machines, the disconnect switch should be so designed that it can be padlocked in its out position—a safety measure against accidental reconnection.
The layout of the machine controls should be such that the operator can easily distinguish and reach them, and that their manipulation presents no hazard. This means that controls must never be arranged at points which can be reached only by passing the hand over the working zone of the machine or where they may be hit by flying chips.
Switches which monitor guards and interlock them with the machine drive should be chosen and installed in such a way that they positively open the circuit as soon as the guard is shifted from its protecting position.
Emergency stop devices must cause the immediate standstill of the dangerous movement. They must be designed and located in such a way that they can be easily operated by the threatened worker. Emergency stop buttons must be easily reached and should be in red.
The actuating elements of control gear which may trip a dangerous machine movement must be guarded so as to exclude any inadvertent operation. For instance, the clutch engaging levers on the headstock and apron should be provided with safety locking devices or screens. A push-button can be made safe by lodging it in a recess or by shrouding it with a protective collar.
Hand-operated controls should be designed and located in such a way that the hand movement corresponds to the controlled machine movement.
Controls should be identified with easily readable and understandable markings. To avoid misunderstandings and linguistic difficulties, it is advisable to use symbols.
Transmission elements
All moving transmission elements (belts, pulleys, gears) must be covered with guards. An important contribution to the prevention of lathe accidents can be made by the persons responsible for the installation of the machine. Lathes should be so installed that the operators tending them do not hinder or endanger each other. The operators should not turn their backs towards passageways. Protective screens should be installed where neighbouring workplaces or passageways are within the range of flying chips.
Passageways must be clearly marked. Enough space should be left for materials-handling equipment, for stacking workpieces and for tool boxes. Bar-stock guides must not protrude into the passageways.
The floor on which the operator stands must be insulated against cold. Care should be taken that the insulation forms no stumbling obstacle, and the flooring should not become slippery even when covered with a film of oil.
Conduit and pipework should be installed in such a way that they do not become obstacles. Temporary installations should be avoided.
Safety engineering measures on the shop floor should be directed in particular at the following points:
- work-holding fixtures (faceplates, chucks, collets) should be dynamically balanced before use
- the maximum permissible speed of a chuck should be indicated on the chuck by the manufacturer and respected by the lathe operator
- when scroll chucks are used, it should be ensured that the jaws cannot be slung out when the lathe is started
- chucks of this type should be designed in such a manner that the key cannot be taken off before the jaws have been secured. The chuck keys in general should be so designed that it is impossible to leave them in the chuck.
It is important to provide for auxiliary lifting equipment to facilitate mounting and removing of heavy chucks and faceplates. To prevent chucks from running off the spindle when the lathe is suddenly braked, they must be securely fixed. This can be achieved by putting a retaining nut with left-hand thread on the spindle nose, by using a “Camlock” quick-action coupling, by fitting the chuck with a locking key or by securing it with a two-part locking ring.
When powered work-holding fixtures are used, such as hydraulically operated chucks, collets and tailstock centres, measures must be taken which make it impossible for the hands to be introduced into the danger zone of closing fixtures. This can be achieved by limiting the travel of the clamping element to 6 mm, by choosing the location of deadman’s controls so as to exclude the introduction of the hands into the danger zone or by providing a moving guard which has to be closed before the clamping movement can be started.
If starting the lathe while the chuck jaws are open presents a danger, the machine should be equipped with a device which prevents the spindle rotation being started before the jaws are closed. The absence of power must not cause the opening or closure of a powered work-holding fixture.
If the gripping force of a power chuck diminishes, the spindle rotation must be stopped, and it must be impossible to start the spindle. Reversing the gripping direction from inside to outside (or vice versa) while the spindle rotates must not cause the chuck to be dislodged from the spindle. Removal of holding fixtures from the spindle should be possible only when the spindle has ceased rotating.
When machining bar stock, the portion projecting beyond the lathe must be enclosed by bar-stock guides. Bar feed weights must be guarded by hinged covers extending to the floor.
Carriers
To prevent serious accidents—in particular, when filing work in a lathe—unprotected carriers must not be used. A centring safety carrier should be used, or a protective collar should be fitted to a conventional carrier. It is also possible to use self-locking carriers or to provide the carrier disc with a protective cover.
Working zone of the lathe
Universal-lathe chucks should be guarded by hinged covers. If possible, protective covers should be interlocked with spindle drive circuits. Vertical boring and turning mills should be fenced with bars or plates to prevent injury from revolving parts. To enable the operator to watch the machining process safely, platforms with railings must be provided. In certain cases, TV cameras can be installed so that the operator may monitor the tool edge and tool in-feed.
The working zones of automatic lathes, NC and CNC lathes should be completely enclosed. Enclosures of fully automatic machines should only have openings through which the stock to be machined is introduced, the turned part ejected and the swarf removed from the working zone. These openings must not constitute a hazard when work passes through them, and it must be impossible to reach through them into the danger zone.
The working zones of semi-automatic, NC and CNC lathes must be enclosed during the machining process. The enclosures are generally sliding covers with limit switches and interlocking circuit.
Operations requiring access to the working zone, such as change of work or tools, gauging and so on, must not be carried out before the lathe has been safely stopped. Zeroing a variable-speed drive is not considered a safe standstill. Machines with such drives must have locked protective covers that cannot be unlocked before the machine is safely stopped (e.g., by cutting the spindle-motor power supply).
If special tool-setting operations are required, an inching control is to be provided which enables certain machine movements to be tripped while the protective cover is open. In such cases, the operator can be protected by special circuit designs (e.g., by permitting only one movement to be tripped at a time). This can be achieved by using two-hand controls.
Turning swarf
Long turning chips are dangerous because they may get entangled with arms and legs and cause serious injury. Continuous and ravelled chips can be avoided by choosing appropriate cutting speeds, feeds and chip thicknesses or by using lathe tools with chip breakers of the gullet or step type. Swarf hooks with handle and buckle should be used for removing chips.
Ergonomics
Every machine should be so designed that it enables a maximal output to be obtained with a minimum of stress on the operator. This can be achieved by adapting the machine to the worker.
Ergonomic factors must be taken into account when designing the human-machine interface of a lathe. Rational workplace design also includes providing for auxiliary handling equipment, such as loading and unloading attachments.
All controls must be located within the physiological sphere or reach of both hands. The controls must be clearly laid out and should be logical to operate. Pedal-operated controls should be avoided in machines tended by standing operators.
Experience has shown that good work is performed when the workplace is designed for both standing and sitting postures. If the operator has to work standing up, he or she should be given the possibility of changing posture. Flexible seats are in many cases a welcome relief for strained feet and legs.
Measures should be taken to create optimal thermal comfort, taking into account the air temperature, relative humidity, air movement and radiant heat. The workshop should be adequately ventilated. There should be local exhaust devices to eliminate gaseous emanations. When machining bar stock, sound-absorbent-lined guide tubes should be used.
The workplace should preferably be provided with uniform lighting, affording an adequate level of illumination.
Work Clothing and Personal Protection
Overalls should be close fitting and buttoned or zipped to the neck. They should be without breast pockets, and the sleeves must be tightly buttoned at the wrists. Belts should not be worn. No finger rings and bracelets should be worn when working on lathes. Wearing of safety spectacles should be obligatory. When heavy workpieces are machined, safety shoes with steel toe caps must be worn. Protective gloves must be worn whenever swarf is being collected.
Training
The lathe operator’s safety depends to a large extent on working methods. It is therefore important that he or she should receive thorough theoretical and practical training to acquire skills and develop a behaviour affording the best possible safeguards. Correct posture, correct movements, correct choice and handling of tools should become routine to such an extent that the operator works correctly even if his or her concentration is temporarily relaxed.
Important points in a training programme are an upright posture, the proper mounting and removal of the chuck and the accurate and secure fixing of workpieces. Correct holding of files and scrapers and safe working with abrasive cloth must be intensively practised.
Workers must be well informed about the hazards of injury which may be caused when gauging work, checking adjustments and cleaning lathes.
Maintenance
Lathes must be regularly maintained and lubricated. Faults must be corrected immediately. If safety is at stake in the event of a fault, the machine should be put out of operation until corrective action has been taken.
Repair and maintenance work must be carried out only after the machine has been isolated from the power supply
.
Prevention of Heat Stress
Although human beings possess considerable ability to compensate for naturally occurring heat stress, many occupational environments and/or physical activities expose workers to heat loads which are so excessive as to threaten their health and productivity. In this article, a variety of techniques are described which can be used to minimize the incidence of heat disorders and reduce the severity of cases when they do occur. Interventions fall into five categories: maximizing heat tolerance among exposed individuals, assuring timely replacement of lost fluid and electrolytes, altering work practices to reduce exertional heat load, engineering control of climatic conditions, and use of protective clothing.
Factors outside the worksite which may affect thermal tolerance should not be ignored in the evaluation of the extent of exposure and consequently in elaborating preventive strategies. For example, total physiological burden and the potential susceptibility to heat disorders will be much higher if heat stress continues during off-duty hours through work at second jobs, strenuous leisure activities, or living in unremittingly hot quarters. In addition, nutritional status and hydration may reflect patterns of eating and drinking, which may also change with season or religious observances.
Maximizing Individual Heat Tolerance
Candidates for hot trades should be generally healthy and possess suitable physical attributes for the work to be done. Obesity and cardiovascular disease are conditions that add to the risks, and individuals with a history of previous unexplained or repetitive heat illness should not be assigned to tasks involving severe heat stress. Various physical and physiological characteristics which may affect heat tolerance are discussed below and fall into two general categories: inherent characteristics beyond the control of the individual, such as body size, gender, ethnicity and age; and acquired characteristics, which are at least partly subject to control and include physical fitness, heat acclimatization, obesity, medical conditions and self-induced stress.
Workers should be informed of the nature of heat stress and its adverse effects as well as the protective measures provided in the workplace. They should be taught that heat tolerance depends to a large extent upon drinking enough water and eating a balanced diet. In addition, workers should be taught the signs and symptoms of heat disorders, which include dizziness, faintness, breathlessness, palpitations and extreme thirst. They should also learn the basics of first aid and where to call for help when they recognize these signs in themselves or others.
Management should implement a system for reporting heat- related incidents at work. Occurrence of heat disorders in more than one person—or repeatedly in a single individual—is often a warning of serious impending trouble and indicates the need for immediate evaluation of the working environment and review of the adequacy of preventive measures.
Human traits affecting adaptation
Body dimensions. Children and very small adults face two potential disadvantages for work in hot environments. First, externally imposed work represents a greater relative load for a body with a small muscle mass, inducing a greater rise in core body temperature and more rapid onset of fatigue. In addition, the higher surface-to-mass ratio of small people may be a disadvantage under extremely hot conditions. These factors together may explain why men weighing less than 50 kg were found to be at increased risk for heat illness in deep mining activities.
Gender. Early laboratory studies on women seemed to show that they were relatively intolerant to work in heat, compared with men. However, we now recognize that nearly all of the differences can be explained in terms of body size and acquired levels of physical fitness and heat acclimatization. However, there are minor sex differences in heat dissipation mechanisms: higher maximal sweat rates in males may enhance tolerance for extremely hot, dry environments, while females are better able to suppress excess sweating and therefore conserve body water and thus heat in hot, humid environments. Although the menstrual cycle is associated with a shift in basal body temperature and slightly alters thermoregulatory responses in women, these physiological adjustments are too subtle to influence heat tolerance and thermoregulatory efficiency in real work situations.
When allowance is made for individual physique and fitness, men and women are essentially alike in their responses to heat stress and their ability to acclimatize to work under hot conditions. For this reason, selection of workers for hot jobs should be based on individual health and physical capacity, not gender. Very small or sedentary individuals of either sex will show poor tolerance for work in heat.
The effect of pregnancy on women’s heat tolerance is not clear, but altered hormone levels and the increased circulatory demands of the foetus on the mother may increase her susceptibility to fainting. Severe maternal hyperthermia (over-heating) due to illness appears to increase the incidence of foetal malformation, but there is no evidence of a similar effect from occupational heat stress.
Ethnicity. Although various ethnic groups have originated in differing climates, there is little evidence of inherent or genetic differences in response to heat stress. All humans appear to function as tropical animals; their ability to live and work in a range of thermal conditions reflects adaptation through complex behaviour and development of technology. Seeming ethnic differences in response to heat stress probably relate to body size, individual life history and nutritional status rather than to inherent traits.
Age. Industrial populations generally show a gradual decline in heat tolerance after age 50. There is some evidence of an obligatory, age-associated reduction in cutaneous vasodilatation (widening of the cavity of blood vessels of the skin) and maximal sweat rate, but most of the change can be attributed to alterations in lifestyle which reduce physical activity and increase the accumulation of body fat. Age does not appear to impair heat tolerance or ability to acclimatize if the individual maintains a high level of aerobic conditioning. However, ageing populations are subject to increasing incidence of cardiovascular disease or other pathologies which may impair individual heat tolerance.
Physical fitness. Maximal aerobic capacity (VO2 max) is probably the strongest single determinant of an individual’s ability to carry out sustained physical work under hot conditions. As noted above, early findings of group differences in heat tolerance which were attributed to gender, race or age are now viewed as manifestations of aerobic capacity and heat acclimatization.
Induction and maintenance of high work capacity require repetitive challenges to the body’s oxygen transport system through vigorous exercise for at least 30 to 40 min, 3 to 4 days per week. In some cases activity on the job may provide the necessary physical training, but most industrial jobs are less strenuous and require supplementation through a regular exercise programme for optimal fitness.
Loss of aerobic capacity (detraining) is relatively slow, so that weekends or vacations of 1 to 2 weeks cause only minimal changes. Serious declines in aerobic capacity are more likely to occur over weeks to months when injury, chronic illness or other stress causes the individual to change lifestyle.
Heat acclimatization. Acclimatization to work in heat can greatly expand human tolerance for such stress, so that a task which is initially beyond the capability of the unacclimatized person may become easier work after a period of gradual adjustment. Individuals with a high level of physical fitness generally display partial heat acclimatization and are able to complete the process more quickly and with less stress than sedentary persons. Season may also affect the time which must be allowed for acclimatization; workers recruited in summer may already be partly heat acclimatized, while winter hires will require a longer period of adjustment.
In most situations, acclimatization can be induced through gradual introduction of the worker to the hot task. For instance, the new recruit may be assigned to hot work only in the morning or for gradually increasing time periods during the first few days. Such acclimatization on the job should take place under close supervision by experienced personnel; the new worker should have standing permission to withdraw to cooler conditions any time symptoms of intolerance occur. Extreme conditions may warrant a formal protocol of progressive heat exposure such as that used for workers in the South African gold mines.
Maintenance of full heat acclimatization requires exposure to work in heat three to four times per week; lower frequency or passive exposure to heat have a much weaker effect and may allow gradual decay of heat tolerance. However, weekends off work have no measurable effect on acclimatization. Discontinuing exposure for 2 to 3 weeks will cause loss of most acclimatization, although some will be retained in persons exposed to hot weather and/or regular aerobic exercise.
Obesity. High body fat content has little direct effect on thermoregulation, as heat dissipation at the skin involves capillaries and sweat glands which lie closer to the skin surface than the subcutaneous fat layer of skin. However, obese persons are handicapped by their excess body weight because every movement requires greater muscular effort and therefore generates more heat than in a lean person. In addition, obesity often reflects an inactive lifestyle with resulting lower aerobic capacity and absence of heat acclimatization.
Medical conditions and other stresses. A worker’s heat tolerance on a given day may be impaired by a variety of conditions. Examples include febrile illness (higher than normal body temperature), recent immunization, or gastroenteritis with associated disturbance of fluid and electrolyte balance. Skin conditions such as sunburn and rashes may limit ability to secrete sweat. In addition, susceptibility to heat illness may be increased by prescription medications, including sympathomimetics, anticholinergics, diuretics, phenothiazines, cyclic antidepressants, and monoamine-oxidase inhibitors.
Alcohol is a common and serious problem among those who work in heat. Alcohol not only impairs intake of food and water, but also acts as a diuretic (increase in urination) as well as disturbing judgement. The adverse effects of alcohol extend many hours beyond the time of intake. Alcoholics who suffer heat stroke have a far higher mortality rate than non-alcoholic patients.
Oral Replacement of Water and Electrolytes
Hydration. Evaporation of sweat is the main path for dissipating body heat and becomes the only possible cooling mechanism when air temperature exceeds body temperature. Water requirements cannot be reduced by training, but only by lowering the heat load on the worker. Human water loss and rehydration have been extensively studied in recent years, and more information is now available.
A human weighing 70 kg can sweat at a rate of 1.5 to 2.0 l/h indefinitely, and it is possible for a worker to lose several litres or up to 10% of body weight during a day in an extremely hot environment. Such loss would be incapacitating unless at least part of the water were replaced during the work shift. However, since water absorption from the gut peaks at about 1.5 l/h during work, higher sweat rates will produce cumulative dehydration through the day.
Drinking to satisfy thirst is not enough to keep a person well hydrated. Most people do not become aware of thirst until they have lost 1 to 2 l of body water, and persons highly motivated to perform hard work may incur losses of 3 to 4 l before clamorous thirst forces them to stop and drink. Paradoxically, dehydration reduces the capacity to absorb water from the gut. Therefore, workers in hot trades must be educated regarding the importance of drinking enough water during work and continuing generous rehydration during off-duty hours. They should also be taught the value of “prehydration”—consuming a large drink of water immediately before the start of severe heat stress—as heat and exercise prevent the body from eliminating excess water in the urine.
Management must provide ready access to water or other appropriate drinks which encourage rehydration. Any physical or procedural obstacle to drinking will encourage “voluntary” dehydration which predisposes to heat illness. The following details are a vital part of any programme for hydration maintenance:
- Safe, palatable water must be located within a few steps of each worker or brought to the worker every hour—more frequently under the most stressful conditions.
- Sanitary drinking cups should be provided, as it is nearly impossible to rehydrate from a water fountain.
- Water containers must be shaded or cooled to 15 to 20ºC (iced drinks are not ideal because they tend to inhibit intake).
Flavourings may be used to improve the acceptance of water. However, drinks that are popular because they “cut” thirst are not recommended, since they inhibit intake before rehydration is complete. For this reason it is better to offer water or dilute, flavoured beverages and to avoid carbonation, caffeine and drinks with heavy concentrations of sugar or salt.
Nutrition. Although sweat is hypotonic (lower salt content) compared to blood serum, high sweat rates involve a continuous loss of sodium chloride and small amounts of potassium, which must be replaced on a daily basis. In addition, work in heat accelerates the turnover of trace elements including magnesium and zinc. All of these essential elements should normally be obtained from food, so workers in hot trades should be encouraged to eat well-balanced meals and avoid substituting candy bars or snack foods, which lack important nutritional components. Some diets in industrialized nations include high levels of sodium chloride, and workers on such diets are unlikely to develop salt deficits; but other, more traditional diets may not contain adequate salt. Under some conditions it may be necessary for the employer to provide salty snacks or other supplementary foods during the work shift.
Industrialized nations are seeing increased availability of “sports drinks” or “thirst quenchers” which contain sodium chloride, potassium and carbohydrates. The vital component of any beverage is water, but electrolyte drinks may be useful in persons who have already developed significant dehydration (water loss) combined with electrolyte depletion (salt loss). These drinks are generally high in salt content and should be mixed with equal or greater volumes of water before consumption. A much more economical mixture for oral rehydration can be made according to the following recipe: to one litre of water, suitable for drinking, add 40 g of sugar (sucrose) and 6 g of salt (sodium chloride). Workers should not be given salt tablets, as they are easily abused, and overdoses lead to gastro-intestinal problems, increased urine output and greater susceptibility to heat illness.
Modified Work Practices
The common goal of modification to work practices is to lower time-averaged heat stress exposure and to bring it within acceptable limits. This can be accomplished by reducing the physical workload imposed on an individual worker or by scheduling appropriate breaks for thermal recovery. In practice, maximum time-averaged metabolic heat production is effectively limited to about 350 W (5 kcal/min) because harder work induces physical fatigue and a need for commensurate rest breaks.
Individual effort levels can be lowered by reducing external work such as lifting, and by limiting required locomotion and static muscle tension such as that associated with awkward posture. These goals may be reached by optimizing task design according to ergonomic principles, providing mechanical aids or dividing the physical effort among more workers.
The simplest form of schedule modification is to allow individual self-pacing. Industrial workers performing a familiar task in a mild climate will pace themselves at a rate which produces a rectal temperature of about 38°C; imposition of heat stress causes them to voluntarily slow the work rate or take breaks. This ability to voluntarily adjust work rate probably depends on awareness of cardiovascular stress and fatigue. Human beings cannot consciously detect elevations in core body temperature; rather, they rely on skin temperature and skin wettedness to assess thermal discomfort.
An alternative approach to schedule modification is the adoption of prescribed work-rest cycles, where management specifies the duration of each work bout, the length of rest breaks and the number of repetitions expected. Thermal recovery takes much longer than the period required to lower respiratory rate and work-induced heart rate: Lowering core temperature to resting levels requires 30 to 40 min in a cool, dry environment, and takes longer if the person must rest under hot conditions or while wearing protective clothing. If a constant level of production is required, then alternating teams of workers must be assigned sequentially to hot work followed by recovery, the latter involving either rest or sedentary tasks performed in a cool place.
Climate Control
If cost were no object, all heat stress problems could be solved by application of engineering techniques to convert hostile working environments to hospitable ones. A wide variety of techniques may be used depending on the specific conditions of the workplace and available resources. Traditionally, hot industries can be divided into two categories: In hot-dry processes, such as metal smelting and glass production, workers are exposed to very hot air combined with strong radiant heat load, but such processes add little humidity to the air. In contrast, warm-moist industries such as textile mills, paper production and mining involve less extreme heating but create very high humidities due to wet processes and escaped steam.
The most economical techniques of environmental control usually involve reduction of heat transfer from the source to the environment. Hot air may be vented outside the work area and replaced with fresh air. Hot surfaces can be covered with insulation or given reflective coatings to reduce heat emissions, simultaneously conserving heat which is needed for the industrial process. A second line of defence is large-scale ventilation of the work area to provide a strong flow of outside air. The most expensive option is air conditioning to cool and dry the atmosphere in the workplace. Although lowering air temperature does not affect transmission of radiant heat, it does help to reduce the temperature of the walls and other surfaces which may be secondary sources of convective and radiative heating.
When overall environmental control proves impractical or uneconomical, it may be possible to ameliorate thermal conditions in local work areas. Air conditioned enclosures may be provided within the larger work space, or a specific work station may be provided with a flow of cool air (“spot cooling” or “air shower”). Local or even portable reflective shielding may be interposed between the worker and a radiant heat source. Alternatively, modern engineering techniques may allow construction of remote systems to control hot processes so that workers need not suffer routine exposure to highly stressful heat environments.
Where the workplace is ventilated with outside air or there is limited air-conditioning capacity, thermal conditions will reflect climatic changes, and sudden increases in outdoor air temperature and humidity may elevate heat stress to levels which overwhelm workers’ heat tolerance. For instance, a spring heat wave can precipitate an epidemic of heat illness among workers who are not yet heat acclimatized as they would be in summer. Management should therefore implement a system for predicting weather-related changes in heat stress so that timely precautions can be taken.
Protective Clothing
Work in extreme thermal conditions may require personal thermal protection in the form of specialized clothing. Passive protection is provided by insulative and reflective garments; insulation alone can buffer the skin from thermal transients. Reflective aprons may be used to protect personnel who work facing a limited radiant source. Fire-fighters who must deal with extremely hot fuel fires wear suits called “bunkers”, which combine heavy insulation against hot air with an aluminized surface to reflect radiant heat.
Another form of passive protection is the ice vest, which is loaded with slush or frozen packets of ice (or dry ice) and is worn over an undershirt to prevent uncomfortable chilling of the skin. The phase change of the melting ice absorbs part of the metabolic and environmental heat load from the covered area, but the ice must be replaced at regular intervals; the greater the heat load, the more frequently the ice must be replaced. Ice vests have proven most useful in deep mines, ship engine rooms, and other very hot, humid environments where access to freezers can be arranged.
Active thermal protection is provided by air- or liquid-cooled garments which cover the entire body or some portion of it, usually the torso and sometimes the head.
Air cooling. The simplest systems are ventilated with the surrounding, ambient air or with compressed air cooled by expansion or passage through a vortex device. High volumes of air are required; the minimum ventilation rate for a sealed suit is about 450 l/min. Air cooling can theoretically take place through convection (temperature change) or evaporation of sweat (phase change). However, the effectiveness of convection is limited by the low specific heat of air and the difficulty in delivering it at low temperatures in hot surroundings. Most air-cooled garments therefore operate through evaporative cooling. The worker experiences moderate heat stress and attendant dehydration, but is able to thermoregulate through natural control of the sweat rate. Air cooling also enhances comfort through its tendency to dry the underclothing. Disadvantages include (1) the need to connect the subject to the air source, (2) the bulk of air distribution garments and (3) the difficulty of delivering air to the limbs.
Liquid cooling. These systems circulate a water-antifreeze mixture through a network of channels or small tubes and then return the warmed liquid to a heat sink which removes the heat added during passage over the body. Liquid circulation rates are usually on the order of 1 l/min. The heat sink may dissipate thermal energy to the environment through evaporation, melting, refrigeration or thermoelectric processes. Liquid-cooled garments offer far greater cooling potential than air systems. A full-coverage suit linked to an adequate heat sink can remove all metabolic heat and maintain thermal comfort without the need to sweat; such a system is used by astronauts working outside their spacecraft. However, such a powerful cooling mechanism requires some type of comfort control system which usually involves manual setting of a valve which shunts part of the circulating liquid past the heat sink. Liquid-cooled systems can be configured as a back pack to provide continuous cooling during work.
Any cooling device which adds weight and bulk to the human body, of course, may interfere with the work at hand. For instance, the weight of an ice vest significantly increases the metabolic cost of locomotion, and is therefore most useful for light physical work such as watch-standing in hot compartments. Systems which tether the worker to a heat sink are impractical for many types of work. Intermittent cooling may be useful where workers must wear heavy protective clothing (such as chemical protective suits) and cannot carry a heat sink or be tethered while they work. Removing the suit for each rest break is time consuming and involves possible toxic exposure; under these conditions, it is simpler to have the workers wear a cooling garment which is attached to a heat sink only during rest, allowing thermal recovery under otherwise unacceptable conditions.
Heat Disorders
High environmental temperature, high humidity, strenuous exercise or impaired heat dissipation may cause a variety of heat disorders. They include heat syncope, heat oedema, heat cramps, heat exhaustion and heat stroke as systemic disorders, and skin lesions as local disorders.
Systemic Disorders
Heat cramps, heat exhaustion and heat stroke are of clinical importance. The mechanisms underlying the development of these systemic disorders are circulatory insufficiency, water and electrolyte imbalance and/or hyperthermia (high body temperature). The most severe of all is heat stroke, which may lead to death unless promptly and properly treated.
Two distinct populations are at risk of developing heat disorders, excluding infants. The first and the larger population is the elderly, especially the poor and those with chronic conditions, such as diabetes mellitus, obesity, malnutrition, congestive heart failure, chronic alcoholism, dementia and the need to use medications that interfere with thermoregulation. The second population at risk of suffering heat disorders comprises healthy individuals who attempt prolonged physical exertion or are exposed to excessive heat stress. Factors predisposing active young people to heat disorders, other than congenital and acquired sweat gland dysfunction, include poor physical fitness, lack of acclimatization, low work efficiency and a reduced ratio of skin area to body mass.
Heat syncope
Syncope is a transient loss of consciousness resulting from a reduction of cerebral blood flow, preceded frequently by pallor, blurring of vision, dizziness and nausea. It may occur in persons suffering from heat stress. The term heat collapse has been used synonymously with heat syncope. The symptoms have been attributed to cutaneous vasodilatation, postural pooling of blood with consequently diminished venous return to the heart, and reduced cardiac output. Mild dehydration, which develops in most persons exposed to heat, contributes to the probability of heat syncope. Individuals who suffer from cardiovascular diseases or who are unacclimatized are predisposed to heat collapse. The victims usually recover consciousness rapidly after they are laid supine.
Heat oedema
Mild dependent oedema—that is, swelling of the hands and feet—may develop in unacclimatized individuals exposed to a hot environment. It typically occurs in women and resolves with acclimatization. It subsides in several hours after the patient has been laid in a cooler place.
Heat cramps
Heat cramps may occur after heavy sweating brought about by prolonged physical work. Painful spasms develop in limb and abdominal muscles subjected to intensive work and fatigue, while body temperature hardly rises. These cramps are caused by the salt depletion that results when the loss of water due to prolonged heavy sweating is replenished with plain water containing no supplementary salt and when the sodium concentration in the blood has fallen below a critical level. Heat cramps themselves are a relatively innocuous condition. The attacks are usually seen in physically fit individuals who are capable of sustained physical exertion, and once were called “miner’s cramps” or “cane-cutter’s cramps” because they would often occur in such labourers.
The treatment of heat cramps consists of cessation of activity, rest in a cool place and replacement of fluid and electrolytes. Heat exposure should be avoided for at least 24 to 48 hours.
Heat exhaustion
Heat exhaustion is the most common heat disorder encountered clinically. It results from severe dehydration after a huge amount of sweat has been lost. It occurs typically in otherwise healthy young individuals who undertake prolonged physical exertion (exertion-induced heat exhaustion), such as marathon runners, outdoor sports players, military recruits, coal miners and construction workers. The basic feature of this disorder is circulatory deficiency due to water and/or salt depletion. It may be considered an incipient stage of heat stroke, and if left untreated, it may eventually progress to heat stroke. It has been conventionally divided into two types: heat exhaustion by water depletion and that by salt depletion; but many cases are a mixture of both types.
Heat exhaustion by water depletion develops as a result of prolonged heavy sweating and insufficient water intake. Since sweat contains sodium ions in a concentration ranging from 30 to 100 milliequivalents per litre, which is lower than that in plasma, a great loss of sweat brings about hypohydration (reduction in body water content) and hypernatraemia (increased sodium concentration in plasma). Heat exhaustion is characterized by thirst, weakness, fatigue, dizziness, anxiety, oliguria (scanty urination), tachycardia (rapid heartbeat) and moderate hyperthermia (39ºC or above). Dehydration also leads to a decline in sweating activity, a rise in skin temperature, and increases in plasma protein and plasma sodium levels and in the haematocrit value (the ratio of blood cell volume to blood volume).
Treatment consists of allowing the victim to rest in a recumbent posture with the knees raised, in a cool environment, wiping the body with a cool towel or sponge and replacing fluid loss by drinking or, if oral ingestion is impossible, by intravenous infusion. The amounts of water and salt replenishment, body temperature and body weight should be monitored carefully. Water ingestion should not be regulated according to the victim’s subjective feeling of thirst, especially when fluid loss is replenished with plain water, because dilution of the blood readily induces disappearance of thirst and dilution diuresis, thus delaying the recovery of body fluid balance. This phenomenon of insufficient water ingestion is called voluntary dehydration. Furthermore, a salt-free water supply may complicate heat disorders, as described below. Dehydration of over 3% of body weight should always be treated by water and electrolyte replacement.
Heat exhaustion by salt depletion results from prolonged heavy sweating and replacement of water and insufficient salt. Its occurrence is promoted by incomplete acclimatization, vomiting and diarrhoea, and so on. This type of heat exhaustion usually develops a few days after the development of water depletion. It is most commonly encountered in sedentary elderly individuals exposed to heat who have drunk a large amount of water in order to quench their thirst. Headache, dizziness, weakness, fatigue, nausea, vomiting, diarrhoea, anorexia, muscle spasms and mental confusion are common symptoms. In blood examinations, decrease in plasma volume, increases in the haematocrit and in plasma protein levels, and hypercalcaemia (excess blood calcium) are noted.
Early detection and prompt management are essential, the latter consisting of letting the patient rest in a recumbent posture in a cool room and providing for replacement of water and electrolytes. The osmolarity or specific gravity of the urine should be monitored, as should urea, sodium and chloride levels in the plasma, and body temperature, body weight, and water and salt intake should also be recorded. If the condition is adequately treated, victims generally feel well within a few hours and recover without sequelae. If not, it may readily proceed to heat stroke.
Heat stroke
Heat stroke is a serious medical emergency which may result in death. It is a complex clinical condition in which uncontrollable hyperthermia causes tissue damage. Such an elevation of body temperature is caused initially by severe heat congestion due to excessive heat load, and the resultant hyperthermia induces dysfunction of the central nervous system, including failure of the normal thermoregulatory mechanism, thus accelerating elevation of the body temperature. Heat stroke occurs basically in two forms: classical heat stroke and exertion-induced heat stroke. The former develops in very young, elderly, obese or unfit individuals undertaking normal activities during prolonged exposure to high environmental temperatures, whereas the latter occurs particularly in young, active adults during physical exertion. In addition, there is a mixed form of heat stoke presenting features consistent with both of the above forms.
Elderly individuals, particularly those who have underlying chronic illness, such as cardiovascular diseases, diabetes mellitus and alcoholism, and those taking certain medications, especially psychotropic drugs, are at a high risk of classical heat stroke. During sustained heat waves, for example, the mortality rate for the population older than 60 years has been recorded as more than ten times greater than that for the population aged 60 and under. A similarly high mortality in the elderly population has also been reported among Muslims during the Mecca pilgrimage, where the mixed form of heat stroke has been found to be prevalent. Factors predisposing the elderly to heat stroke, other than chronic diseases as mentioned above, include reduced thermal perception, sluggish vasomotor and sudomotor (sweating reflex) responses to changes in thermal load, and reduced capacity for acclimatization to heat.
Individuals who work or exercise vigorously in hot, humid environments are at a high risk of exertion-induced heat illness, whether heat exhaustion or heat stroke. Athletes undergoing high physical stress can fall victim to hyperthermia by producing metabolic heat at a high rate, even when the environment is not very hot, and have often suffered heat stress illness as a result. Relatively unfit non-athletes are at a lesser risk in this regard as long as they realize their own capacity and limit their exertions accordingly. However, when they play sports for fun and are highly motivated and enthusiastic, they often try to exert themselves at an intensity beyond that for which they have been trained, and may succumb to heat illness (usually heat exhaustion). Poor acclimatization, inadequate hydration, unsuitable dress, alcohol consumption and skin illness causing anhidrosis (reduction in or lack of sweating), notably prickly heat (see below), all aggravate the symptoms.
Children are more susceptible to heat exhaustion or heat stroke than adults. They produce more metabolic heat per unit mass, and are less able to dissipate heat because of a relatively low capacity to produce sweat.
Clinical features of heat stroke
Heat stroke is defined by three criteria:
- severe hyperthermia with a core (deep body) temperature usually exceeding 42ºC
- disturbances of the central nervous system
- hot, dry skin with cessation of sweating.
The diagnosis of heat stroke is easy to establish when this triad of criteria is met. However, it may be missed when one of those criteria is absent, obscure or overlooked. For example, unless core temperature is measured properly and without delay, severe hyperthermia may not be recognized; or, in a very early stage of exertion-induced heat stroke, sweating may still persist or may even be profuse and the skin may be wet.
The onset of heat stroke is usually abrupt and without precursory symptoms, but some patients with impending heat stroke may have symptoms and signs of disturbances of the central nervous system. They include headache, nausea, dizziness, weakness, drowsiness, confusion, anxiety, disorientation, apathy, aggressiveness and irrational behaviour, tremor, twitching and convulsion. Once heat stroke occurs, disturbances of the central nervous system are present in all cases. The level of consciousness is often depressed, deep coma being most common. Seizures occur in the majority of cases, especially in physically fit individuals. Signs of cerebellar dysfunction are prominent and may persist. Pin-pointed pupils are frequently seen. Cerebellar ataxia (lack of muscular coordination), hemiplegia (paralysis of one side of the body), aphasia and emotional instability may persist in some of survivors.
Vomiting and diarrhoea often occur. Tachypnoea (rapid breathing) is usually present initially and the pulse may be weak and rapid. Hypotension, one of the most common complications, results from marked dehydration, extensive peripheral vasodilatation and eventual depression of cardiac muscle. Acute renal failure may be seen in severe cases, especially in exertion-induced heat stroke.
Haemorrhages occur in all parenchymal organs, in the skin (where they are called petechiae) and in the gastro-intestinal tract in severe cases. Clinical haemorrhagic manifestations include melaena (dark-coloured, tarry faeces), haematemesis (blood vomiting), haematuria (bloody urine), haemoptysis (spitting blood), epistaxis (nosebleed), purpura (purple spots), ecchymosis (black and blue marks) and conjunctival haemorrhage. Intravascular coagulation occurs commonly. Haemorrhagic diathesis (bleeding tendency) is usually associated with disseminated intra-vascular coagulation (DIC). DIC occurs predominantly in exertion-induced heat stroke, where the fibrinolytic (clot-dissolving) activity of plasma is increased. On the other hand, a decrease in platelet count, prolongation of prothrombin time, depletion of coagulation factors and increased level of fibrin degradation products (FDP) are provoked by whole-body hyperthermia. Patients with evidence of DIC and bleeding have higher core temperature, lower blood pressure, lower arterial blood pH and pO2, a higher incidence of oliguria or anuria and of shock, and a higher mortality rate.
Shock is also a common complication. It is attributable to peripheral circulatory failure and is aggravated by DIC, which causes dissemination of clots in the microcirculatory system.
Treatment of heat stroke
Heat stroke is a medical emergency that requires prompt diagnosis and rapid and aggressive treatment to save the patient’s life. Proper measurement of core temperature is mandatory: rectal or oesophageal temperature should be measured by using a thermo-meter which can read up to 45ºC. Measurement of oral and axillary temperatures should be avoided because they can vary significantly from real core temperature.
The objective of treatment measures is to lower body temperature by reducing heat load and promoting heat dissipation from the skin. The treatment includes moving the patient to a safe, cool, shady and well-ventilated place, removing unnecessary clothing, and fanning. Cooling the face and head may promote beneficial brain cooling.
The efficiency of some cooling techniques has been questioned. It has been argued that placing cold packs over major blood vessels in the neck, groin and axillae and immersion of the body in cold water or covering it with iced towels may promote shivering and cutaneous vasoconstriction, thus actually impeding cooling efficiency. Traditionally, immersion in an ice-water bath, combined with vigorous skin massage to minimize cutaneous vasoconstriction, has been recommended as the treatment of choice, once the patient is brought to a medical facility. This method of cooling has several disadvantages: there are the nursing difficulties posed by the need to administer oxygen and fluids and to monitor blood pressure and the electrocardiogram continuously, and there are the hygienic problems of contamination of the bath with the vomitus and diarrhoea of comatose patients. An alternative approach is to spray a cool mist over the patient’s body while fanning to promote evaporation from the skin. This method of cooling can reduce the core temperature by 0.03 to 0.06ºC/min.
Measures to prevent convulsions, seizures and shivering should also be initiated at once. Continuous cardiac monitoring and determination of serum electrolyte levels and arterial and venous blood-gas analysis are essential, and intravenous infusion of electrolyte solutions at a relatively low temperature of approximately 10ºC, together with controlled oxygen therapy, should be commenced in a timely fashion. Tracheal intubation to protect the airway, insertion of a cardiac catheter to estimate central venous pressure, placement of a gastric tube and insertion of a urinary catheter may also be included among additional recommended measures.
Prevention of heat stroke
For the prevention of heat stroke, a wide variety of human factors should be taken into account, such as acclimatization, age, build, general health, water and salt intake, clothing, peculiarities of religious devotion and ignorance of, or liability to neglect, regulations intended to promote public health.
Prior to physical exertion in a hot environment, workers, athletes or pilgrims should be informed of the work load and the level of heat stress they may encounter, and of the risks of heat stroke. A period of acclimatization is recommended before vigorous physical activity and/or severe exposure is risked. The level of activity should be matched to the ambient temperature, and physical exertion should be avoided or at least minimized during the hottest hours of the day. During physical exertion, free access to water is mandatory. Since electrolytes are lost in sweat and the opportunity for voluntary ingestion of water may be limited, thus delaying restitution from thermal dehydration, electrolytes should also be replaced in case of profuse sweating. Proper clothing is also an important measure. Clothes made of fabrics which are both water-absorbent and permeable to air and water vapour facilitate heat dissipation.
Skin Disorders
Miliaria is the most common skin disorder associated with heat load. It occurs when the delivery of sweat onto the skin surface is prevented due to obstruction of the sweat ducts. Sweat retention syndrome ensues when anhidrosis (inability to release sweat) is widespread over the body surface and predisposes the patient to heat stroke.
Miliaria is commonly induced by physical exertion in a hot, humid environment; by febrile diseases; by the application of wet compresses, bandages, plaster casts or adhesive plaster; and by wearing poorly permeable clothes. Miliaria can be classified into three types, according to the depth of sweat retention: miliaria crystallina, miliaria rubra and miliaria profunda.
Miliaria crystallina is caused by retention of sweat within or just beneath the horny layer of the skin, where tiny, clear, non-inflammatory blisters can be seen. They typically appear in “crops” after severe sunburn or during a febrile illness. This type of miliaria is otherwise symptomless, the least distressing, and heals spontaneously in a few days, when the blisters break out to leave scales.
Miliaria rubra occurs when intense heat load causes prolonged and profuse sweating. It is the most common type of miliaria, in which sweat accumulates in the epidermis. Red papules, vesicles or pustules are formed, accompanied by burning and itching sensations (prickly heat). The sweat duct is plugged at the terminal portion. The production of the plug is attributable to the action of resident aerobic bacteria, notably cocci, which increase in population greatly in the horny layer when it is hydrated with sweat. They secrete a toxin which injures the horny epithelial cells of the sweat duct and provokes an inflammatory reaction, precipitating a cast within the lumen of the sweat duct. Infiltration by leukocytes creates an impaction which completely obstructs the passage of sweat for several weeks.
In miliaria profunda, sweat is retained in the dermis, and produces flat, inflammatory papules, nodules and abscesses, with less itching than in miliaria rubra. The occurrence of this type of miliaria is commonly confined to the tropics. It may develop in a progressive sequence from miliaria rubra after repeated bouts of profuse sweating, as the inflammatory reaction extends downwards from the upper skin layers.
Tropical anhidrotic asthenia. The term achieved currency during the Second World War, when troops deployed to tropical theatres suffered from heat rash and heat intolerance. It is a modality of sweat retention syndrome encountered in hot, humid tropical environments. It is characterized by anhidrosis and miliaria-like rashes, accompanied by symptoms of heat congestion, such as palpitation, rapid pulsation, hyperthermia, headache, weakness and gradually to rapidly progressing inability to tolerate physical activity in the heat. It is usually preceded by widespread miliaria rubra.
Treatment. The initial and essential treatment of miliaria and sweat retention syndrome is to transfer the affected person to a cool environment. Cool showers and gentle drying of the skin and the application of calamine lotion may attenuate the patient’s distress. Application of chemical bacteriostats is effective in preventing the expansion of microflora, and is preferable to the use of antibiotics, which may lead these micro-organisms to acquire resistance.
The impactions in the sweat duct slough off after about 3 weeks as a result of epidermal renewal.
Welding and Thermal Cutting
This article is a revision of the 3rd edition of the Encyclopaedia of Occupational Health and Safety article “Welding and thermal cutting” by G.S. Lyndon.
Process Overview
Welding is a generic term referring to the union of pieces of metal at joint faces rendered plastic or liquid by heat or pressure, or both. The three common direct sources of heat are:
- flame produced by the combustion of fuel gas with air or oxygen
- electrical arc, struck between an electrode and a workpiece or between two electrodes
- electrical resistance offered to passage of current between two or more workpieces.
Other sources of heat for welding are discussed below (see table 1).
Table 1. Process materials inputs and pollution outputs for lead smelting and refining
|
Process |
Material input |
Air emissions |
Process wastes |
Other wastes |
|
Lead sintering |
Lead ore, iron, silica, limestone flux, coke, soda, ash, pyrite, zinc, caustic, baghouse dust |
Sulphur dioxide, particulate matter contain-ing cadmium and lead |
||
|
Lead smelting |
Lead sinter, coke |
Sulphur dioxide, particulate matter contain-ing cadmium and lead |
Plant washdown wastewater, slag granulation water |
Slag containing impurities such as zinc, iron, silica and lime, surface impoundment solids |
|
Lead drossing |
Lead bullion, soda ash, sulphur, baghouse dust, coke |
Slag containing such impurities as copper, surface impoundment solids |
||
|
Lead refining |
Lead drossing bullion |
In gas welding and cutting, oxygen or air and a fuel gas are fed to a blowpipe (torch) in which they are mixed prior to combustion at the nozzle. The blowpipe is usually hand held (see figure 1). The heat melts the metal faces of the parts to be joined, causing them to flow together. A filler metal or alloy is frequently added. The alloy often has a lower melting point than the parts to be joined. In this case, the two pieces are generally not brought to fusion temperature (brazing, soldering). Chemical fluxes may be used to prevent oxidation and facilitate the joining.
Figure 1. Gas welding with a torch & rod of filter metal. The welder is protected by a leather apron, gauntlets and goggles

In arc welding, the arc is struck between an electrode and the workpieces. The electrode can be connected to either an alternating current (AC) or direct current (DC) electric supply. The temperature of this operation is about 4,000°C when the workpieces fuse together. Usually it is necessary to add molten metal to the joint either by melting the electrode itself (consumable electrode processes) or by melting a separate filler rod which is not carrying current (non-consumable electrode processes).
Most conventional arc welding is done manually by means of a covered (coated) consumable electrode in a hand-held electrode holder. Welding is also accomplished by many semi or fully automatic electric welding processes such as resistance welding or continuous electrode feed.
During the welding process, the welding area must be shielded from the atmosphere in order to prevent oxidation and contamination. There are two types of protection: flux coatings and inert gas shielding. In flux-shielded arc welding, the consumable electrode consists of a metal core surrounded by a flux coating material, which is usually a complex mixture of mineral and other components. The flux melts as welding progresses, covering the molten metal with slag and enveloping the welding area with a protective atmosphere of gases (e.g., carbon dioxide) generated by the heated flux. After welding, the slag must be removed, often by chipping.
In gas-shielded arc welding, a blanket of inert gas seals off the atmosphere and prevents oxidation and contamination during the welding process. Argon, helium, nitrogen or carbon dioxide are commonly used as the inert gases. The gas selected depends upon the nature of the materials to be welded. The two most popular types of gas-shielded arc welding are metal- and tungsten inert gas (MIG and TIG).
Resistance welding involves using the electrical resistance to the passage of a high current at low voltage through components to be welded to generate heat for melting the metal. The heat generated at the interface between the components brings them to welding temperatures.
Hazards and Their Prevention
All welding involves hazards of fire, burns, radiant heat (infrared radiation) and inhalation of metal fumes and other contaminants. Other hazards associated with specific welding processes include electrical hazards, noise, ultraviolet radiation, ozone, nitrogen dioxide, carbon monoxide, fluorides, compressed gas cylinders and explosions. See table 2 for additional detail.
Table 2. Description and hazards of welding processes
|
Welding Process |
Description |
Hazards |
|
Gas welding and cutting |
||
|
Welding |
The torch melts the metal surface and filler rod, causing a joint to be formed. |
Metal fumes, nitrogen dioxide, carbon monoxide, noise, burns, infrared radiation, fire, explosions |
|
Brazing |
The two metal surfaces are bonded without melting the metal. The melting temperature of the filler metal is above 450 °C. Heating is done by flame heating, resistance heating and induction heating. |
Metal fumes (especially cadmium), fluorides, fire, explosion, burns |
|
Soldering |
Similar to brazing, except the melting temperature of the filler metal is below 450 °C. Heating is also done using a soldering iron. |
Fluxes, lead fumes, burns |
|
Metal cutting and flame gouging |
In one variation, the metal is heated by a flame, and a jet of pure oxygen is directed onto the point of cutting and moved along the line to be cut. In flame gouging, a strip of surface metal is removed but the metal is not cut through. |
Metal fumes, nitrogen dioxide, carbon monoxide, noise, burns, infrared radiation, fire, explosions |
|
Gas pressure welding |
The parts are heated by gas jets while under pressure, and become forged together. |
Metal fumes, nitrogen dioxide, carbon monoxide, noise, burns, infrared radiation, fire, explosions |
|
Flux-shielded arc welding |
||
|
Shielded metal arc welding (SMAC); “stick” arc welding; manual metal arc welding (MMA); open arc welding |
Uses a consumable electrode consisting of a metal core surrounded by a flux coating |
Metal fumes, fluorides (especially with low-hydrogen electrodes), infrared and ultraviolet radiation, burns, electrical, fire; also noise, ozone, nitrogen dioxide |
|
Submerged arc welding (SAW) |
A blanket of granulated flux is deposited on the workpiece, followed by a consumable bare metal wire electrode. The arc melts the flux to produce a protective molten shield in the welding zone. |
Fluorides, fire, burns, infrared radiation, electrical; also metal fumes, noise, ultraviolet radiation, ozone, and nitrogen dioxide |
|
Gas-shielded arc welding |
||
|
Metal inert gas (MIG); gas metal arc welding (GMAC) |
The electrode is normally a bare consumable wire of similar composition to the weld metal and is fed continuously to the arc. |
Ultraviolet radiation, metal fumes, ozone, carbon monoxide (with CO2 gas), nitrogen dioxide, fire, burns, infrared radiation, electrical, fluorides, noise |
|
Tungsten inert gas (TIG); gas tungsten arc welding (GTAW); heliarc |
The tungsten electrode is non-consumable, and filler metal is introduced as a consumable into the arc manually. |
Ultraviolet radiation, metal fumes, ozone, nitrogen dioxide, fire, burns, infrared radiation, electrical, noise, fluorides, carbon monoxide |
Plasma arc welding (PAW) and plasma arc spraying; tungsten arc cutting |
Similar to TIG welding, except that the arc and stream of inert gases pass through a small orifice before reaching the workpiece, creating a “plasma” of highly ionized gas which can achieve temperatures of over 33,400°C.This is also used for metallizing. |
Metal fumes, ozone, nitrogen dioxide, ultraviolet and infrared radiation, noise; fire, burns, electrical, fluorides, carbon monoxide, possible x rays |
|
Flux core arc welding (FCAW); metal active gas welding (MAG) |
Uses a flux-cored consumable electrode; may have carbon dioxide shield (MAG) |
Ultraviolet radiation, metal fumes, ozone, carbon monoxide (with CO2 gas), nitrogen dioxide, fire, burns, infrared radiation, electrical, fluorides, noise |
|
Electric resistance welding |
||
|
Resistance welding (spot, seam, projection or butt welding) |
A high current at low voltage flows through the two components from electrodes. The heat generated at the interface between the components brings them to welding temperatures. During the passage of the current, pressure by the electrodes produces a forge weld. No flux or filler metal is used. |
Ozone, noise (sometimes), machinery hazards, fire, burns, electrical, metal fumes |
|
Electro-slag welding |
Used for vertical butt welding. The workpieces are set vertically, with a gap between them, and copper plates or shoes are placed on one or both sides of the joint to form a bath. An arc is established under a flux layer between one or more continuously fed electrode wires and a metal plate. A pool of molten metal is formed, protected by molten flux or slag, which is kept molten by resistance to the current passing between the electrode and the workpieces. This resistance-generated heat melts the sides of the joint and the electrode wire, filling the joint and making a weld. As welding progresses, the molten metal and slag are retained in position by shifting the copper plates. |
Burns, fire, infrared radiation, electrical, metal fumes |
|
Flash welding |
The two metal parts to be welded are connected to a low-voltage, high-current source. When the ends of the components are brought into contact, a large current flows, causing “flashing” to occur and bringing the ends of the components to welding temperatures. A forge weld is obtained by pressure. |
Electrical, burns, fire, metal fumes |
Other welding processes |
||
|
Electron beam welding |
A workpiece in an vacuum chamber is bombarded by a beam of electrons from an electron gun at high voltages. The energy of the electrons is transformed into heat upon striking the workpiece, thus melting the metal and fusing the workpiece. |
X rays at high voltages, electrical, burns, metal dusts, confined spaces |
|
Arcair cutting |
An arc is struck between the end of a carbon electrode (in a manual electrode holder with its own supply of compressed air) and the workpiece. The molten metal produced is blown away by jets of compressed air. |
Metal fumes, carbon monoxide, nitrogen dioxide, ozone, fire, burns, infrared radiation, electrical |
|
Friction welding |
A purely mechanical welding technique in which one component remains stationary while the other is rotated against it under pressure. Heat is generated by friction, and at forging temperature the rotation ceases. A forging pressure then effects the weld. |
Heat, burns, machinery hazards |
|
Laser welding and drilling |
Laser beams can be used in industrial applications requiring exceptionally high precision, such as miniature assemblies and micro techniques in the electronics industry or spinnerets for the artificial fibre industry. The laser beam melts and joins the workpieces. |
Electrical, laser radiation, ultraviolet radiation, fire, burns, metal fumes, decomposition products of workpiece coatings |
|
Stud welding |
An arc is struck between a metal stud (acting as the electrode) held in a stud welding gun and the metal plate to be joined, and raises the temperature of the ends of the components to melting point. The gun forces the stud against the plate and welds it. Shielding is provided by a ceramic ferrule surrounding the stud. |
Metal fumes, infrared and ultraviolet radiation, burns, electrical, fire, noise, ozone, nitrogen dioxide |
|
Thermite welding |
A mixture of aluminium powder and a metal oxide powder (iron, copper, etc.) is ignited in a crucible, producing molten metal with the evolution of intense heat. The crucible is tapped and the molten metal flows into the cavity to be welded (which is surrounded by a sand mould). This is often used to repair castings or forgings. |
Fire, explosion, infrared radiation, burns |
Much welding is not done in shops where conditions can generally be controlled, but in the field in the construction or repair of large structures and machinery (e.g., frameworks of buildings, bridges and towers, ships, railroad engines and cars, heavy equipment and so on). The welder may have to carry all his or her equipment to the site, set it up and work in confined spaces or on scaffolds. Physical strain, inordinate fatigue and musculoskeletal injuries may follow being required to reach, kneel or work in other uncomfortable and awkward positions. Heat stress may result from working in warm weather and the occlusive effects of the personal protective equipment, even without the heat generated by the welding process.
Compressed gas cylinders
In high-pressure gas welding installations, oxygen and the fuel gas (acetylene, hydrogen, town gas, propane) are supplied to the torch from cylinders. The gases are stored in these cylinders at high pressure. The special fire and explosion hazards and precautions for the safe use and storage of the fuel gases are also discussed elsewhere in this Encyclopaedia. The following precautions should be observed:
- Only pressure regulators designed for the gas in use should be fitted to cylinders. For example, an acetylene regulator should not be used with coal gas or hydrogen (although it may be used with propane).
- Blowpipes must be kept in good order and cleaned at regular intervals. A hardwood stick or soft brass wire should be used for cleaning the tips. They should be connected to regulators with special canvas-reinforced hoses placed in such a way that they are unlikely to be damaged.
- Oxygen and acetylene cylinders must be stored separately and only on fire-resistant premises devoid of flammable material and must be so located that they may be readily removed in case of fire. Local building and fire protection codes must be consulted.
- The colour coding in force or recommended for identification of cylinders and accessories should be scrupulously observed. In many countries, the internationally accepted colour codes used for the transport of dangerous materials are applied in this field. The case for enforcement of uniform international standards in this respect is strengthened by safety considerations bound up with the increasing international migration of industrial workers.
Acetylene generators
In the low-pressure gas welding process, acetylene is generally produced in generators by reaction of calcium carbide and water. The gas is then piped to the welding or cutting torch into which oxygen is fed.
Stationary generating plants should be installed either in the open air or in a well-ventilated building away from the main workshops. The ventilation of the generator house should be such as to prevent the formation of an explosive or toxic atmosphere. Adequate lighting should be provided; switches, other electrical gear and electrical lamps should either be located outside the building or be explosion-proof. Smoking, flames, torches, welding plant or flammable materials must be excluded from the house or from the vicinity of an open-air generator. Many of these precautions also apply to portable generators. Portable generators should be used, cleaned and recharged only in the open air or in a well-ventilated shop, away from any flammable material.
Calcium carbide is supplied in sealed drums. The material should be stored and kept dry, on a platform raised above the floor level. Stores must be situated under cover, and if they adjoin another building the party wall must be fireproof. The storeroom should be suitably ventilated through the roof. Drums should be opened only immediately before the generator is charged. A special opener should be provided and used; a hammer and chisel should never be used to open drums. It is dangerous to leave calcium carbide drums exposed to any source of water.
Before a generator is dismantled, all calcium carbide must be removed and the plant filled with water. The water should remain in the plant for at least half an hour to ensure that every part is free from gas. The dismantling and servicing should be carried out only by the manufacturer of the equipment or by a specialist. When a generator is being recharged or cleaned, none of the old charge must be used again.
Pieces of calcium carbide wedged in the feed mechanism or adhering to parts of the plant should be carefully removed, using non-sparking tools made of bronze or another suitable non-ferrous alloy.
All concerned should be fully conversant with the manufacturer’s instructions, which should be conspicuously displayed. The following precautions should also be observed:
- A properly designed back-pressure valve must be fitted between the generator and each blowpipe to prevent backfire or reverse flow of gas. The valve should be regularly inspected after backfire, and the water level checked daily.
- Only blowpipes of the injector type designed for low-pressure operation should be used. For heating and cutting, town gas or hydrogen at low pressure are sometimes employed. In these cases, a non-return valve should be placed between each blowpipe and the supply main or pipeline.
- An explosion may be caused by “flash-back”, which results from dipping the nozzle-tip into the molten metal pool, mud or paint, or from any other stoppage. Particles of slag or metal that become attached to the tip should be removed. The tip should also be cooled frequently.
- Local building and fire codes should be consulted.
Fire and explosion prevention
In locating welding operations, consideration should be given to surrounding walls, floors, nearby objects and waste material. The following procedures should be followed:
- All combustible material must be removed or adequately protected by sheet metal or other suitable materials; tarpaulins should never be used.
- Wood structures should be discouraged or similarly protected. Wood floors should be avoided.
- Precautionary measures should be taken in the case of openings or cracks in walls and floors; flammable material in adjoining rooms or on the floor below should be removed to a safe position. Local building and fire codes should be consulted.
- Suitable fire-extinguishing apparatus should always be at hand. In the case of low-pressure plant using an acetylene generator, buckets of dry sand should also be kept available; fire extinguishers of dry powder or carbon dioxide types are satisfactory. Water must never be used.
- Fire brigades may be necessary. A responsible person should be assigned to keep the site under observation for at least half an hour after completion of the work, in order to deal with any outbreak of fire.
- Since explosions can occur when acetylene gas is present in air in any proportion between 2 and 80%, adequate ventilation and monitoring are required to ensure freedom from gas leaks. Only soapy water should be used to search for gas leaks.
- Oxygen must be carefully controlled. For example, it should never be released into the air in a confined space; many metals, clothing and other materials become actively combustible in the presence of oxygen. In gas cutting, any oxygen which may not be consumed will be released into the atmosphere; gas cutting should never be undertaken in a confined space without proper ventilation arrangements.
- Alloys rich in magnesium or other combustible metals should be kept away from welding flames or arcs.
- Welding of containers can be extremely hazardous. If the previous contents are unknown, a vessel should always be treated as if it had contained a flammable substance. Explosions may be prevented either by removing any flammable material or by making it non-explosive and non-flammable.
- The mixture of aluminium and iron oxide used in thermite welding is stable under normal conditions. However, in view of the ease with which aluminium powder will ignite, and the quasi-explosive nature of the reaction, appropriate precautions should be taken in handling and storage (avoidance of exposure to high heat and possible ignition sources).
- A written hot-work permit programme is required for welding in some jurisdictions. This programme outlines the precautions and procedures to be followed during welding, cutting, burning and so on. This programme should include the specific operations conducted along with the safety precautions to be implemented. It must be plant specific and may include an internal permit system that must be completed with each individual operation.
Protection from heat and burn hazards
Burns of the eyes and exposed parts of the body may occur due to contact with hot metal and spattering of incandescent metal particles or molten metal. In arc welding, a high-frequency spark used to initiate the arc can cause small, deep burns if concentrated at a point on the skin. Intense infrared and visible radiation from a gas welding or cutting flame and incandescent metal in the weld pool can cause discomfort to the operator and persons in the vicinity of the operation. Each operation should be considered in advance, and necessary precautions designed and implemented. Goggles made specifically for gas welding and cutting should be worn to protect the eyes from heat and light radiated from the work. Protective covers over filter glass should be cleaned as required and replaced when scratched or damaged. Where molten metal or hot particles are emitted, the protective clothing being worn should deflect spatter. The type and thickness of fire-resistant clothing worn should be chosen according to the degree of hazard. In cutting and arc welding operations, leather shoe coverings or other suitable spats should be worn to prevent hot particles from falling into boots or shoes. For protecting the hands and forearms against heat, spatter, slag and so on, the leather gauntlet type of glove with canvas or leather cuffs is sufficient. Other types of protective clothing include leather aprons, jackets, sleeves, leggings and head covering. In overhead welding, a protective cape and cap are necessary. All protective clothing should be free from oil or grease, and seams should be inside, so as not to trap globules of molten metal. Clothing should not have pockets or cuffs that could trap sparks, and it should be worn so sleeves overlap gloves, leggings overlap shoes and so on. Protective clothing should be inspected for burst seams or holes through which molten metal or slag may enter. Heavy articles left hot on completion of welding should always be marked “hot” as a warning to other workers. With resistance welding, the heat produced may not be visible, and burns can result from handling of hot assemblies. Particles of hot or molten metal should not fly out of spot, seam or projection welds if conditions are correct, but non-flammable screens should be used and precautions taken. Screens also protect passers-by from eye burns. Loose parts should not be left in the throat of the machine because they are liable to be projected with some velocity.
Electrical safety
Although no-load voltages in manual arc welding are relatively low (about 80 V or less), welding currents are high, and transformer primary circuits present the usual hazards of equipment operated at power supply line voltage. The risk of electric shock should therefore not be ignored, especially in cramped spaces or in insecure positions.
Before welding commences, the grounding installation on arc welding equipment should always be checked. Cables and connections should be sound and of adequate capacity. A proper grounding clamp or bolted terminal should always be used. Where two or more welding machines are grounded to the same structure, or where other portable electric tools are also in use, grounding should be supervised by a competent person. The working position should be dry, secure and free from dangerous obstructions. A well-arranged, well-lighted, properly ventilated and tidy workplace is important. For work in confined spaces or dangerous positions, additional electrical protection (no-load, low-voltage devices) can be installed in the welding circuit, ensuring that only extremely low-voltage current is available at the electrode holder when welding is not taking place. (See discussion of confined spaces below.) Electrode holders in which the electrodes are held by a spring grip or screw thread are recommended. Discomfort due to heating can be reduced by effective heat insulation on that part of the electrode holder which is held in the hand. Jaws and connections of electrode holders should be cleaned and tightened periodically to prevent overheating. Provision should be made to accommodate the electrode holder safely when not in use by means of an insulated hook or a fully insulated holder. The cable connection should be designed so that continued flexing of the cable will not cause wear and failure of the insulation. Dragging of cables and plastic gas supply tubes (gas-shielded processes) across hot plates or welds must be avoided. The electrode lead should not come in contact with the job or any other earthed object (ground). Rubber tubes and rubber-covered cables must not be used anywhere near the high-frequency discharge, because the ozone produced will rot the rubber. Plastic tubes and polyvinyl chloride (PVC) covered cables should be used for all supplies from the transformer to the electrode holder. Vulcanized or tough rubber-sheathed cables are satisfactory on the primary side. Dirt and metallic or other conducting dust can cause a breakdown in the high-frequency discharge unit. To avoid this condition, the unit should be cleaned regularly by blowing-out with compressed air. Hearing protection should be worn when using compressed air for more than a few seconds. For electron-beam welding, the safety of the equipment used must be checked prior to each operation. To protect against electric shock, a system of interlocks must be fitted to the various cabinets. A reliable system of grounding of all units and control cabinets is necessary. For plasma welding equipment used for cutting heavy thicknesses, the voltages may be as high as 400 V and danger should be anticipated. The technique of firing the arc by a high-frequency pulse exposes the operator to the dangers of an unpleasant shock and a painful, penetrating high-frequency burn.
Ultraviolet radiation
The brilliant light emitted by an electric arc contains a high proportion of ultraviolet radiation. Even momentary exposure to bursts of arc flash, including stray flashes from other workers’ arcs, may produce a painful conjunctivitis (photo-ophthalmia) known as “arc eye” or “eye flash”. If any person is exposed to arc flash, immediate medical attention must be sought. Excessive exposure to ultraviolet radiation may also cause overheating and burning of the skin (sunburn effect). Precautions include:
- A shield or helmet fitted with correct grade of filter should be used (see the article “Eye and face protection” elsewhere in this Encyclopaedia). For the gas-shielded arc welding processes and carbon-arc cutting, flat handshields provide insufficient protection from reflected radiation; helmets should be used. Filtered goggles or eyeglasses with sideshields should be worn under the helmet to avoid exposure when the helmet is lifted up for inspection of the work. Helmets will also provide protection from spatter and hot slag. Helmets and handshields are provided with a filter glass and a protective cover glass on the outside. This should be regularly inspected, cleaned and replaced when scratched or damaged.
- The face, nape of the neck and other exposed parts of the body should be properly protected, especially when working close to other welders.
- Assistants should wear suitable goggles at a minimum and other PPE as the risk requires.
- All arc welding operations should be screened to protect other persons working nearby. Where the work is carried out at fixed benches or in welding shops, permanent screens should be erected where possible; otherwise, temporary screens should be used. All screens should be opaque, of sturdy construction and of a flame-resistant material.
- The use of black paints for the inside of welding booths has become an accepted practice, but the paint should produce a matte finish. Adequate ambient lighting should be provided to prevent eye strain leading to headaches and accidents.
- Welding booths and portable screens should be checked regularly to ensure that there is no damage which might result in the arc affecting persons working nearby.
Chemical hazards
Airborne contaminants from welding and flame cutting, including fumes and gases, arise from a variety of sources:
- the metal being welded, the metal in the filler rod or constituents of various types of steel such as nickel or chromium)
- any metallic coating on the article being welded or on the filler rod (e.g., zinc and cadmium from plating, zinc from galvanizing and copper as a thin coating on continuous mild steel filler rods)
- any paint, grease, debris and the like on the article being welded (e.g., carbon monoxide, carbon dioxide, smoke and other irritant breakdown products)
- flux coating on the filler rod (e.g., inorganic fluoride)
- the action of heat or ultraviolet light on the surrounding air (e.g., nitrogen dioxide, ozone) or on chlorinated hydrocarbons (e.g., phosgene)
- inert gas used as a shield (e.g., carbon dioxide, helium, argon).
Fumes and gases should be removed at the source by LEV. This can be provided by partial enclosure of the process or by the installation of hoods which supply sufficiently high air velocity across the weld position so as to ensure capture of the fumes.
Special attention should be paid to ventilation in the welding of non-ferrous metals and certain alloy steels, as well as to protection from the hazard of ozone, carbon monoxide and nitrogen dioxide which may be formed. Portable as well as fixed ventilation systems are readily available. In general, the exhausted air should not be recirculated. It should be recirculated only if there are not hazardous levels of ozone or other toxic gases and the exhaust air is filtered through a high-efficiency filter.
With electron-beam welding and if materials being welded are of a toxic nature (e.g., beryllium, plutonium and so on), care must be taken to protect the operator from any dust cloud when opening the chamber.
When there is a risk to health from toxic fumes (e.g., lead) and LEV is not practicable—for example, when lead-painted structures are being demolished by flame cutting—the use of respiratory protective equipment is necessary. In such circumstances, an approved, high-efficiency full-facepiece respirator or ahigh-efficiency positive pressure powered air-purified respirator (PAPR) should be worn. A high standard of maintenance of the motor and the battery is necessary, especially with the original high-efficiency positive pressure power respirator. The use of positive pressure compressed air line respirators should be encouraged where a suitable supply of breathing-quality compressed air is available. Whenever respiratory protective equipment is to be worn, the safety of the workplace should be reviewed to determine whether extra precautions are necessary, bearing in mind the restricted vision, entanglement possibilities and so on of persons wearing respiratory protective equipment.
Metal fume fever
Metal fume fever is commonly seen in workers exposed to the fumes of zinc in the galvanizing or tinning process, in brass founding, in the welding of galvanized metal and in metallizing or metal spraying, as well as from exposure to other metals such as copper, manganese and iron. It occurs in new workers and those returning to work after a weekend or holiday hiatus. It is an acute condition that occurs several hours after the initial inhalation of particles of a metal or its oxides. It starts with a bad taste in the mouth followed by dryness and irritation of the respiratory mucosa resulting in cough and occasionally dyspnoea and “tightness” of the chest. These may be accompanied by nausea and headache and, some 10 to 12 hours after the exposure, chills and fever which may be quite severe. These last several hours and are followed by sweating, sleep and often by polyuria and diarrhoea. There is no particular treatment, and recovery is usually complete in about 24 hours with no residua. It can be prevented by keeping exposure to the offending metallic fumes well within the recommended levels through the use of efficient LEV.
Confined spaces
For entry into confined spaces, there may be a risk of the atmosphere being explosive, toxic, oxygen deficient or combinations of the above. Any such confined space must be certified by a responsible person as safe for entry and for work with an arc or flame. A confined-space entry programme, including an entry permit system, may be required and is highly recommended for work that must be carried out in spaces that are typically not constructed for continuous occupancy. Examples include, but are not limited to, manholes, vaults, ship holds and the like. Ventilation of confined spaces is crucial, since gas welding not only produces airborne contaminants but also uses up oxygen. Gas-shielded arc welding processes can decrease the oxygen content of the air. (See figure 2.)
Figure 2. Welding in an enclosed space

S. F. Gilman
Noise
Noise is a hazard in several welding processes, including plasma welding, some types of resistance welding machines and gas welding. In plasma welding, the plasma jet is ejected at very high speeds, producing intense noise (up to 90 dBA), particularly in the higher frequency bands. The use of compressed air to blow off dust also creates high noise levels. To prevent hearing damage, ear plugs or muffs must be worn and a hearing conservation programme should be instituted, including audiometric (hearing capacity) examinations and employee training.
Ionizing radiation
In welding shops where welds are inspected radiographically with x-ray or gamma-ray equipment, the customary warning notices and instructions must be strictly observed. Workers must be kept at a safe distance from such equipment. Radioactive sources must be handled only with the required special tools and subject to special precautions.
Local and governmental regulations must be followed. See the chapter Radiation, ionizing elsewhere in this Encyclopaedia.
Sufficient shielding must be provided with electron-beam welding to prevent x rays from penetrating the walls and windows of the chamber. Any parts of the machine providing shields against x-ray radiation should be interlocked so that the machine cannot be energized unless they are in position. Machines should be checked at the time of installation for leaks of x-ray radiation, and regularly thereafter.
Other hazards
Resistance welding machines have at least one electrode, which moves with considerable force. If a machine is operated while a finger or hand is lying between the electrodes, severe crushing will result. Where possible, a suitable means of guarding must be devised to safeguard the operator. Cuts and lacerations can be minimized by first deburring components and by wearing protective gloves or gauntlets.
Lockout/tagout procedures should be used when machinery with electrical, mechanical or other energy sources is being maintained or repaired.
When slag is being removed from welds by chipping and so on, the eyes should be protected by goggles or other means.
Effect of Heat Stress and Work in the Heat
When a person is exposed to warm environmental conditions the physiological heat loss mechanisms are activated in order to maintain normal body temperature. Heat fluxes between the body and the environment depend on the temperature difference between:
- the surrounding air and objects like walls, windows, the sky, and so on
- the surface temperature of the person
The surface temperature of the person is regulated by physiological mechanisms, such as variations in the blood flow to the skin, and by evaporation of sweat secreted by the sweat glands. Also, the person can change clothing to vary the heat exchange with the environment. The warmer the environmental conditions, the smaller the difference between surrounding temperatures and skin or clothing surface temperature. This means that the “dry heat exchange” by convection and radiation is reduced in warm compared to cool conditions. At environmental temperatures above the surface temperature, heat is gained from the surroundings. In this case this extra heat together with that liberated by the metabolic processes must be lost through evaporation of sweat for the maintenance of body temperature. Thus evaporation of sweat becomes more and more critical with increasing environmental temperature. Given the importance of sweat evaporation it is not surprising that wind velocity and air humidity (water vapour pressure) are critical environmental factors in hot conditions. If the humidity is high, sweat is still produced but evaporation is reduced. Sweat which cannot evaporate has no cooling effect; it drips off and is wasted from a thermoregulatory point of view.
The human body contains approximately 60% water, about 35 to 40 l in an adult person. About one-third of the water in the body, the extracellular fluid, is distributed between the cells and in the vascular system (the blood plasma). The remaining two-thirds of the body water, the intracellular fluid, is located inside the cells. The composition and the volume of the body water compartments is very precisely controlled by hormonal and neural mechanisms. Sweat is secreted from the millions of sweat glands on the skin surface when the thermoregulatory centre is activated by an increase in body temperature. The sweat contains salt (NaCl, sodium chloride) but to a lesser extent than the extracellular fluid. Thus, both water and salt are lost and must be replaced after sweating.
Effects of Sweat Loss
In neutral, comfortable, environmental conditions, small amounts of water are lost by diffusion through the skin. However, during hard work and in hot conditions, large quantities of sweat can be produced by active sweat glands, up to more than 2 l/h for several hours. Even a sweat loss of only 1% of body weight (» 600 to 700 ml) has a measurable effect on the ability to perform work. This is seen by a rise in heart rate (HR) (HR increases about five beats per minute for each per cent loss of body water) and a rise in body core temperature. If work is continued there is a gradual increase in body temperature, which can rise to a value around 40ºC; at this temperature, heat illness may result. This is partly due to the loss of fluid from the vascular system (figure 1). A loss of water from the blood plasma reduces the amount of blood which fills the central veins and the heart. Each heart beat will therefore pump a smaller stroke volume. As a consequence the cardiac output (the amount of blood which is expelled by the heart per minute) tends to fall, and the heart rate must increase in order to maintain the circulation and the blood pressure.
Figure 1. Calculated distributions of water in the extracellular compartment (ECW) and intracellular compartment (ICW) before and after 2 h of exercise dehydration at 30°C room temperature.
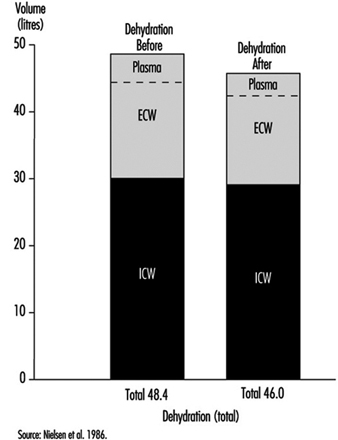
A physiological control system called the baroreceptor reflex system maintains the cardiac output and blood pressure close to normal under all conditions. The reflexes involve receptors, sensors in the heart and in the arterial system (aorta and carotid arteries), which monitor the degree of stretching of the heart and vessels by the blood which fills them. Impulses from these travel through nerves to the central nervous system, from which adjustments, in case of dehydration, cause a constriction in the blood vessels and a reduction in blood flow to splanchnic organs (liver, gut, kidneys) and to the skin. In this way the available blood flow is redistributed to favour circulation to the working muscles and to the brain (Rowell 1986).
Severe dehydration may lead to heat exhaustion and circulatory collapse; in this case the person cannot maintain the blood pressure, and fainting is the consequence. In heat exhaustion, symptoms are physical exhaustion, often together with headache, dizziness and nausea. The main cause of heat exhaustion is the circulatory strain induced by water loss from the vascular system. The decline in blood volume leads to reflexes which reduce circulation to the intestines and the skin. The reduction in skin blood flow aggravates the situation, since heat loss from the surface decreases, so the core temperature increases further. The subject may faint due to a fall in blood pressure and the resulting low blood flow to the brain. The lying position improves the blood supply to the heart and brain, and after cooling and having some water to drink the person regains his or her well-being almost immediately.
If the processes causing the heat exhaustion “run wild”, it develops into heat stroke. The gradual reduction in skin circulation makes the temperature rise more and more, and this leads to a reduction, even a stop in sweating and an even faster rise in core temperature, which causes circulatory collapse and may result in death, or irreversible damage to the brain. Changes in the blood (such as high osmolality, low pH, hypoxia, cell adherence of the red blood cells, intravascular coagulation) and damage to the nervous system are findings in heat stroke patients. The reduced blood supply to the gut during heat stress can provoke tissue damage, and substances (endotoxins) may be liberated which induce fever in connection with heat stroke (Hales and Richards 1987). Heat stroke is an acute, life-threatening emergency further discussed in the section on “heat disorders”.
Together with water loss, sweating produces a loss of electrolytes, mainly sodium (Na+) and chloride (Cl–), but also to a lesser degree magnesium (Mg++), potassium (K+) and so on (see table 1). The sweat contains less salt than the body fluid compartments. This means that they become more salty after sweat loss. The increased saltiness seems to have a specific effect on the circulation via effects on vascular smooth muscle, which controls the degree to which the vessels are open. However, it is shown by several investigators to interfere with the ability to sweat, in such a way that it takes a higher body temperature to stimulate the sweat glands—the sensitivity of the sweat glands becomes reduced (Nielsen 1984). If the sweat loss is replaced only by water, this may lead to a situation where the body contains less sodium chloride than in the normal state (hypo-osmotic). This will cause cramps due to the malfunction of nerves and muscles, a condition known in earlier days as “miner’s cramps” or “stoker’s cramps”. It can be prevented by addition of salt to the diet (drinking beer was a suggested preventive measure in the UK in the 1920s!).
Table 1. Electrolyte concentration in blood plasma and in sweat
|
Electrolytes and other |
Blood plasma concen- |
Sweat concentrations |
|
Sodium (Na+) |
3.5 |
0.2–1.5 |
|
Potassium (K+) |
0.15 |
0.15 |
|
Calcium (Ca++) |
0.1 |
small amounts |
|
Magnesium (Mg++) |
0.02 |
small amounts |
|
Chloride (Cl–) |
3.5 |
0.2–1.5 |
|
Bicarbonate (HCO3–) |
1.5 |
small amounts |
|
Proteins |
70 |
0 |
|
Fats, glucose, small ions |
15–20 |
small amounts |
Adapted from Vellar 1969.
The decreased skin circulation and sweat gland activity both affect thermoregulation and heat loss in such a way that core temperature will increase more than in the fully hydrated state.
In many different trades, workers are exposed to external heat stress—for example, workers in steel plants, glass industries, paper mills, bakeries, mining industries. Also chimney sweeps and firefighters are exposed to external heat. People who work in confined spaces in vehicles, ships and aircraft may also suffer from heat. However, it must be noted that persons working in protective suits or doing hard work in waterproof clothes can be victims of heat exhaustion even in moderate and cool environmental temperature conditions. Adverse effects of heat stress occur in conditions where the core temperature is elevated and the sweat loss is high.
Rehydration
The effects of dehydration due to sweat loss may be reversed by drinking enough to replace the sweat. This will usually take place during recovery after work and exercise. However, during prolonged work in hot environments, performance is improved by drinking during activity. The common advice is thus to drink when thirsty.
But, there are some very important problems in this. One is that the urge to drink is not strong enough to replace the simultaneously occurring water loss; and secondly, the time needed to replace a large water deficit is very long, more than 12 hours. Lastly, there is a limit to the rate at which water can pass from the stomach (where it is stored) to the intestine (gut), where the absorption takes place. This rate is lower than observed sweat rates during exercise in hot conditions.
There have been a large number of studies on various beverages to restore body water, electrolytes and carbohydrate stores of athletes during prolonged exercise. The main findings are as follows:
- The amount of the fluid which can be utilized—that is, transported through the stomach to the intestine—is limited by the “gastric emptying rate”, which has a maximum of about 1,000 ml/h.
- If the fluid is “hyperosmotic” (contains ions/molecules in higher concentrations than the blood) the rate is slowed down. On the other hand “iso-osmotic fluids” (containing water and ions/molecules to the same concentration, osmolality, as blood) are passed at the same rate as pure water.
- Addition of small amounts of salt and sugar increases the rate of uptake of water from the gut (Maughan 1991).
With this in mind you can make your own “rehydration fluid” or choose from a large number of commercial products. Normally water and electrolyte balance is regained by drinking in connection with meals. Workers or athletes with large sweat losses should be encouraged to drink more than their urge. Sweat contains about 1 to 3 g of NaCl per litre. This means that sweat losses of above 5 l per day may cause a deficiency in sodium chloride, unless the diet is supplemented.
Workers and athletes are also counselled to control their water balance by weighing themselves regularly—for example, in the morning (at same time and condition)—and try to maintain a constant weight. However, a change in body weight does not necessarily reflect the degree of hypohydration. Water is chemically bound to glycogen, the carbohydrate store in the muscles, and liberated when glycogen is used during exercise. Weight changes of up to about 1 kg may occur, depending on the glycogen content of the body. The body weight “morning to morning” also shows changes due to “biological variations” in water contents—for example, in women in relation to the menstrual cycle up to 1 to 2 kg of water can be retained during the premenstrual phase (“premenstrual tension”).
The control of water and electrolytes
The volume of the body water compartments—that is, the extracellular and intracellular fluid volumes—and their concentrations of electrolytes is held very constant through a regulated balance between intake and loss of fluid and substances.
Water is gained from the intake of food and fluid, and some is liberated by metabolic processes, including combustion of fat and carbohydrates from food. The loss of water takes place from the lungs during breathing, where the inspired air takes up water in the lungs from moist surfaces in the airways before it is exhaled. Water also diffuses through the skin in small amount in comfortable conditions during rest. However, during sweating water can be lost at rates of more than 1 to 2 l/h for several hours. The body water content is controlled. Increased water loss by sweating is compensated for by drinking and by a reduction in urine formation, while excess water is excreted by increased urine production.
This control both of intake and output of water is exerted through the autonomic nervous system, and by hormones. Thirst will increase the water intake, and the water loss by the kidneys is regulated; both the volume and electrolyte composition of urine are under control. The sensors in the control mechanism are in the heart, responding to the “fullness” of the vascular system. If the filling of the heart is reduced—for example, after a sweat loss—the receptors will signal this message to the brain centres responsible for the sensation of thirst, and to areas which induce a liberation of anti-diuretic hormone (ADH) from the posterior pituitary. This hormone acts to reduce the urine volume.
Similarly, physiological mechanisms control the electrolyte composition of the body fluids via processes in the kidneys. The food contains nutrients, minerals, vitamins and electrolytes. In the present context, the intake of sodium chloride is the important issue. The dietary sodium intake varies with eating habits, between 10 and 20 to 30 g per day. This is normally much more than is needed, so the excess is excreted by the kidneys, controlled by the action of multiple hormonal mechanisms (angiotensin, aldosterone, ANF, etc.) which are controlled by stimuli from osmoreceptors in the brain and in the kidneys, responding to the osmolality of primarily Na+ and Cl– in the blood and in the fluid in the kidneys, respectively.
Interindividual and Ethnic Differences
Differences between male and female as well as younger and older persons in reaction to heat might be expected. They differ in certain characteristics which might influence heat transfer, such as surface area, height/weight ratio, thickness of insulating skin fat layers, and in physical ability to produce work and heat (aerobic capacity » maximal oxygen consumption rate). Available data suggest that heat tolerance is reduced in older persons. They start to sweat later than do young individuals, and older people react with a higher blood flow in their skin during heat exposure.
Comparing the sexes it has been observed that women tolerate humid heat better than men do. In this environment the evaporation of sweat is reduced, so the slightly greater surface/mass area in women could be to their advantage. However, aerobic capacity is an important factor to be considered when comparing individuals exposed to heat. In laboratory conditions the physiological responses to heat are similar, if groups of subjects with the same physical work capacity (“maximal oxygen uptake”—VO2 max) are tested—for instance, younger and older males, or males versus females (Pandolf et al. 1988). In this case a certain work task (exercise on a bicycle ergometer) will result in the same load on the circulatory system—that is, the same heart rate and the same rise in core temperature—independent of age and sex.
The same considerations are valid for comparison between ethnic groups. When differences in size and aerobic capacity are taken into account, no significant differences due to race can be pointed out. But in daily life in general, older persons do have, on average, a lower VO2 max than younger persons, and females a lower VO2 max than males in the same age group.
Therefore, when performing a specific task which consists of a certain absolute work rate (measured, e.g., in Watts), the person with a lower aerobic capacity will have a higher heart rate and body temperature and be less able to cope with the extra strain of external heat, than one with a higher VO2 max.
For occupational health and safety purposes a number of heat stress indices have been developed. In these the large interindividual variation in response to heat and work are taken into account, as well as the specific hot environments for which the index is constructed. These are treated elsewhere in this chapter.
Persons exposed repeatedly to heat will tolerate the heat better after even a few days. They become acclimatized. Sweating rate is increased and the resulting increased cooling of the skin leads to a lower core temperature and heart rate during work under the same conditions.
Therefore, artificial acclimation of personnel who are expected to be exposed to extreme heat (firefighters, rescue personnel, military personnel) will probably be of benefit to reduce the strain.
Summing up, the more heat a person produces, the more must be dissipated. In a hot environment the evaporation of sweat is the limiting factor for heat loss. Interindividual differences in the capacity for sweating are considerable. While some persons have no sweat glands at all, in most cases, with physical training and repeated exposure to heat, the amount of sweat produced in a standard heat stress test is increased. Heat stress results in an increase in heart rate and core temperature. Maximal heart rate and/or a core temperature of about 40ºC sets the absolute physiological limit for work performance in a hot environment (Nielsen 1994).
Physiological Responses to the Thermal Environment
Humans live their entire lives within a very small, fiercely protected range of internal body temperatures. The maximal tolerance limits for living cells range from about 0ºC (ice crystal formation) to about 45ºC (thermal coagulation of intracellular proteins); however, humans can tolerate internal temperatures below 35ºC or above 41ºC for only very brief periods of time. To maintain internal temperature within these limits, people have developed very effective and in some instances specialized physiological responses to acute thermal stresses. These responses—designed to facilitate the conservation, production or elimination of body heat—involve the finely controlled coordination of several body systems.
Human Thermal Balance
By far, the largest source of heat imparted to the body results from metabolic heat production (M). Even at peak mechanical efficiency, 75 to 80% of the energy involved in muscular work is liberated as heat. At rest, a metabolic rate of 300 ml O2 per minute creates a heat load of approximately 100 Watts. During steady-state work at an oxygen consumption of 1 l/min, approximately 350 W of heat are generated—less any energy associated with external work (W). Even at such a mild to moderate work intensity, body core temperature would rise approximately one degree centigrade every 15 min were it not for an efficient means of heat dissipation. In fact, very fit individuals can produce heat in excess of 1,200 W for 1 to 3 hours without heat injury (Gisolfi and Wenger 1984).
Heat can also be gained from the environment via radiation (R) and convection (C) if the globe temperature (a measure of radiant heat) and air (dry-bulb) temperature, respectively, exceed skin temperature. These avenues of heat gain are typically small relative to M, and actually become avenues of heat loss when the skin-to-air thermal gradient is reversed. The final avenue for heat loss—evaporation (E)—is also typically the most important, since the latent heat of vaporization of sweat is high—approximately 680 W-h/l of sweat evaporated. These relations are discussed elsewhere in this chapter.
Under cool to thermoneutral conditions, heat gain is balanced by heat loss, no heat is stored, and body temperature equilibrates; that is:
M–W ± R ± C–E = 0
However, in more severe exposure to heat:
M–W ± R ± C >E
and heat is stored. In particular, heavy work (high energy expenditure which increases M–W), excessively high air temperatures (which increase R+C), high humidity (which limits E) and the wearing of thick or relatively impermeable clothing (which creates a barrier to effective evaporation of sweat) create such a scenario. Finally, if exercise is prolonged or hydration inadequate, E may be outstripped by the limited ability of the body to secrete sweat (1 to 2 l/h for short periods).
Body Temperature and Its Control
For purposes of describing physiological responses to heat and cold, the body is divided into two components—the “core” and the “shell”. Core temperature (Tc) represents internal or deep body temperature, and can be measured orally, rectally or, in laboratory settings, in the oesophagus or on the tympanic membrane (eardrum). The temperature of the shell is represented by mean skin temperature (Tsk). The average temperature of the body (Tb) at any time is a weighted balance between these temperatures, that is
Tb = k Tc + (1– k) Tsk
where the weighting factor k varies from about 0.67 to 0.90.
When confronted with challenges to thermal neutrality (heat or cold stresses), the body strives to control Tc through physiological adjustments, and Tc provides the major feedback to the brain to coordinate this control. While the local and mean skin temperature are important for providing sensory input, Tsk varies greatly with ambient temperature, averaging about 33 ºC at thermoneutrality and reaching 36 to 37 ºC under conditions of heavy work in the heat. It can drop considerably during whole-body and local exposure to cold; tactile sensitivity occurs between 15 and 20 ºC, whereas the critical temperature for manual dexterity is between 12 and 16 ºC. The upper and lower pain threshold values for Tsk are approximately 43 ºC and 10 ºC, respectively.
Precise mapping studies have localized the site of greatest thermoregulatory control in an area of the brain known as the pre- optic/anterior hypothalamus (POAH). In this region are nerve cells which respond to both heating (warm-sensitive neurons) and cooling (cold-sensitive neurons). This area dominates control of body temperature by receiving afferent sensory information about body temperature and sending efferent signals to the skin, the muscles and other organs involved in temperature regulation, via the autonomic nervous system. Other areas of the central nervous system (posterior hypothalamus, reticular formation, pons, medulla and spinal cord) form ascending and descending connections with the POAH, and serve a variety of facilitory functions.
The body’s control system is analogous to thermostatic control of temperature in a house with both heating and cooling capabilities. When body temperature rises above some theoretical “set point” temperature, effector responses associated with cooling (sweating, increasing skin blood flow) are turned on. When body temperature falls below the set point, heat gain responses (decreasing skin blood flow, shivering) are initiated. Unlike home heating/cooling systems however, the human thermoregulatory control system does not operate as a simple on-off system, but also has proportional control and rate-of-change control characteristics. It should be appreciated that a “set point temperature” exists in theory only, and thus is useful in visualizing these concepts. Much work is yet to be done toward a full understanding of the mechanisms associated with the thermoregulatory set point.
Whatever its basis, the set point is relatively stable and is unaffected by work or ambient temperature. In fact, the only acute perturbation known to shift the set point is the group of endogenous pyrogens involved in the febrile response. The effector responses employed by the body to maintain thermal balance are initiated and controlled in response to a “load error”, that is, a body temperature which is transiently above or below the set point (figure 1). A core temperature below the set point creates a negative load error, resulting in heat gain (shivering, vasoconstriction of the skin) being initiated. A core temperature above the set point creates a positive load error, leading to heat loss effectors (skin vasodilatation, sweating) being turned on. In each case, the resultant heat transfer decreases the load error and helps return the body temperature to a steady state.
Figure 1. A model of thermoregulation in the human body.
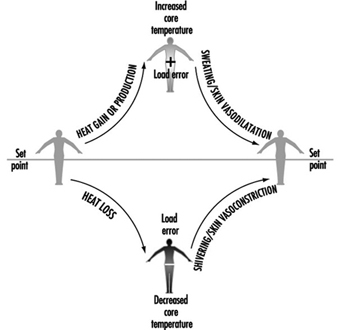
Temperature Regulation in the Heat
As mentioned above, humans lose heat to the environment primarily through a combination of dry (radiation and convection) and evaporative means. To facilitate this exchange, two primary effector systems are turned on and regulated—skin vasodilatation and sweating. While skin vasodilatation often results in small increases in dry (radiative and convective) heat loss, it functions primarily to transfer heat from the core to the skin (internal heat transfer), while evaporation of sweat provides an extremely effective means of cooling the blood prior to its return to deep body tissues (external heat transfer).
Skin vasodilatation
The amount of heat transferred from the core to the skin is a function of the skin blood flow (SkBF), the temperature gradient between core and skin, and the specific heat of blood (a little less than 4 kJ/°C per litre of blood). At rest in a thermoneutral environment, the skin gets approximately 200 to 500 ml/min of blood flow, representing only 5 to 10% of the total blood pumped by the heart (cardiac output). Because of the 4ºC gradient between Tc (about 37ºC) and Tsk (about 33ºC under such conditions), the metabolic heat produced by the body to sustain life is constantly convected to the skin for dissipation. By contrast, under conditions of severe hyperthermia such as high-intensity work in hot conditions, the core-to-skin thermal gradient is smaller, and the necessary heat transfer is accomplished by large increases in SkBF. Under maximal heat stress, SkBF can reach 7 to 8 l/min, about one-third of cardiac output (Rowell 1983). This high blood flow is achieved through a poorly understood mechanism unique to humans which has been called the “active vasodilator system”. Active vasodilatation involves sympathetic nerve signals from the hypothalamus to the skin arterioles, but the neurotransmitter has not been determined.
As mentioned above, SkBF is primarily responsive to increases in Tc and, to a lesser extent, Tsk. Tc rises as muscular work is initiated and metabolic heat production begins, and once some threshold Tc is reached, SkBF also begins to increase dramatically. This basic thermoregulatory relationship is also acted upon by non-thermal factors. This second level of control is critical in that it modifies SkBF when overall cardiovascular stability is threatened. The veins in the skin are very compliant, and a significant portion of the circulating volume pools in these vessels. This aids in heat exchange by slowing the capillary circulation to increase transit time; however, this pooling, coupled with fluid losses from sweating, may also decrease the rate of blood return to the heart. Among the non-thermal factors which have been shown to influence SkBF during work are upright posture, dehydration and positive-pressure breathing (respirator use). These act through reflexes which are turned on when cardiac filling pressure is decreased and stretch receptors located in the large veins and right atrium are unloaded, and are therefore most evident during prolonged aerobic work in an upright posture. These reflexes function to maintain arterial pressure and, in the case of work, to maintain adequate blood flow to active muscles. Thus, the level of SkBF at any given point in time represents the aggregate effects of thermoregulatory and non-thermoregulatory reflex responses.
The need to increase blood flow to the skin to aid in temperature regulation greatly impacts on the ability of the cardiovascular system to regulate blood pressure. For this reason, a coordinated response of the entire cardiovascular system to heat stress is necessary. What cardiovascular adjustments occur that allow for this increase in cutaneous flow and volume? During work in cool or thermoneutral conditions, the needed increase in cardiac output is well supported by increasing heart rate (HR), since further increases in stroke volume (SV) are minimal beyond exercise intensities of 40% of maximum. In the heat, HR is higher at any given work intensity as compensation for the reduced central blood volume (CBV) and SV. At higher levels of work, maximal heart rate is reached, and this tachycardia is therefore incapable of sustaining the necessary cardiac output. The second way in which the body supplies a high SkBF is by distributing blood flow away from such areas as the liver, kidneys and intestines (Rowell 1983). This redirection of flow can provide an additional 800 to 1,000 ml of blood flow to the skin, and helps offset the detrimental effects of peripheral pooling of blood.
Sweating
Thermoregulatory sweat in humans is secreted from 2 to 4 million eccrine sweat glands scattered non-uniformly over the body surface. Unlike apocrine sweat glands, which tend to be clustered (on the face and hands and in the axial and genital regions) and which secrete sweat into hair follicles, eccrine glands secrete sweat directly onto the skin surface. This sweat is odourless, colourless and relatively dilute, since it is an ultrafiltrate of plasma. Thus it has a high latent heat of vaporization and is ideally suited for its cooling purpose.
As an example of the effectiveness of this cooling system, a man working at an oxygen cost of 2.3 l/min produces a net metabolic heat (M–W) of about 640 W. Without sweating, body temperature would increase at a rate of about 1°C every 6 to 7 min. With efficient evaporation of about 16 g of sweat per minute (a reasonable rate), the rate of heat loss can match the rate of heat production, and body core temperature can be maintained at a steady state; that is,
M–W±R±C–E = 0
Eccrine glands are simple in structure, consisting of a coiled secretory portion, a duct and a skin pore. The volume of sweat produced by each gland is dependent upon both the structure and the function of the gland, and total sweating rate in turn depends on both the recruitment of glands (active sweat gland density) and sweat gland output. The fact that some people sweat more heavily than others is attributable mainly to differences in sweat gland size (Sato and Sato 1983). Heat acclimation is another major determinant of sweat production. With ageing, lower sweating rates are attributable not to fewer activated eccrine glands, but to a decreased sweat output per gland (Kenney and Fowler 1988). This decline probably relates to a combination of structural and functional alterations which accompany the ageing process.
Like vasomotor signals, nerve impulses to the sweat glands originate in the POAH and descend through the brainstem. The fibres which innervate the glands are sympathetic cholinergic fibres, a rare combination in the human body. While acetylcholine is the primary neurotransmitter, adrenergic transmitters (catecholamines) also stimulate eccrine glands.
In many ways, control of sweating is analogous to control of skin blood flow. Both have similar onset characteristics (threshold) and linear relationships to increasing Tc. The back and chest tend to have earlier onsets of sweating, and the slopes for the relationship of local sweat rate to Tc are steepest for these sites. Like SkBF, sweating is modified by non-thermal factors such as hypohydration and hyperosmolality. Also worth noting is a phenomenon called “hidromeiosis”, which occurs in very humid environments or on skin areas constantly covered with wet clothing. Such areas of skin, due to their continuously wet state, decrease sweat output. This serves as a protective mechanism against continued dehydration, since sweat which stays on the skin rather than evaporating serves no cooling function.
If sweating rate is adequate, evaporative cooling is determined ultimately by the water vapour pressure gradient between the wet skin and the air surrounding it. Thus, high humidity and heavy or impermeable clothing limit evaporative cooling, while dry air, air movement about the body and minimal, porous clothing facilitate evaporation. On the other hand, if work is heavy and sweating profuse, evaporative cooling can likewise be limited by the body’s ability to produce sweat (maximally about 1 to 2 l/h).
Temperature Regulation in the Cold
One important difference in the way humans respond to cold compared to heat is that behaviour plays a much greater role in thermoregulatory response to cold. For example, wearing appropriate clothing and assuming postures which minimize surface area available for heat loss (“huddling”) are far more important in cold ambient conditions than in the heat. A second difference is the greater role played by hormones during cold stress, including the increased secretion of catecholamines (norepinephrine and epinephrine) and thyroid hormones.
Skin vasoconstriction
An effective strategy against heat loss from the body through radiation and convection is to increase the effective insulation provided by the shell. In humans this is accomplished by decreasing blood flow to the skin—that is, by skin vasoconstriction. Constriction of the cutaneous vessels is more pronounced in the extremities than on the trunk. Like active vasodilatation, skin vasoconstriction is also controlled by the sympathetic nervous system, and is influenced by Tc, Tsk and local temperatures.
The effect of skin cooling on the heart rate and blood pressure response varies with the area of the body which is cooled, and whether the cold is severe enough to cause pain. For example, when the hands are immersed in cold water, HR, systolic blood pressure (SBP) and diastolic blood pressure (DBP) all increase. When the face is cooled, SBP and DBP increase due to the generalized sympathetic response; however, HR goes down due to a parasympathetic reflex (LeBlanc 1975). To further confound the complexity of the overall response to cold, there is a wide range of variability in responses from one person to another. If the cold stress is of sufficient magnitude to decrease body core temperature, HR may either increase (due to sympathetic activation) or decrease (due to the increased central blood volume).
A specific case of interest is termed cold-induced vasodilatation (CIVD). When the hands are placed in cold water, SkBF initially decreases to conserve heat. As tissue temperatures drop, SkBF paradoxically increases, decreases again, and repeats this cyclical pattern. It has been suggested that CIVD is beneficial in preventing tissue damage from freezing, but this is unproven. Mechanistically, the transient dilation probably occurs when the direct effects of the cold are severe enough to decrease nerve transmission, which transiently overrides the effect of the cold on the blood vessel sympathetic receptors (mediating the constrictor effect).
Shivering
As body cooling progresses, the second line of defence is shivering. Shivering is the random involuntary contraction of superficial muscle fibres, which does not limit heat loss but rather increases heat production. Since such contractions do not produce any work, heat is generated. A resting person can increase his or her metabolic heat production about three- to fourfold during intense shivering, and can increase Tc by 0.5ºC. The signals to initiate shivering arise principally from the skin, and, in addition to the POAH region of the brain, the posterior hypothalamus is also involved to a large extent.
Although many individual factors contribute to shivering (and cold tolerance in general), one important factor is body fatness. A man with very little subcutaneous fat (2 to 3 mm thickness) starts shivering after 40 min at 15ºC and 20 min at 10ºC, while a man who has more insulating fat (11 mm) may not shiver at all at 15ºC and after 60 min at 10ºC (LeBlanc 1975).
Forging and Stamping
Process Overview
Forming metal parts by application of high compressive and tensile forces is common throughout industrial manufacturing. In stamping operations, metal, most often in the form of sheets, strips or coils, is formed into specific shapes at ambient temperatures by shearing, pressing and stretching between dies, usually in a series of one or more discrete impact steps. Cold-rolled steel is the starting material in many stamping operations creating sheet metal parts in the automotive and appliance and other industries. Approximately 15% of workers in the automotive industry work in stamping operations or plants.
In forging, compressive force is applied to pre-formed blocks (blanks) of metal, usually heated to high temperatures, also in one or more discrete pressing steps. The shape of the final piece is determined by the shape of the cavities in the metal die or dies used. With open impression dies, as in drop hammer forging, the blank is compressed between one die attached to the bottom anvil and the vertical ram. With closed impression dies, as in press forging, the blank is compressed between the bottom die and an upper die attached to the ram.
Drop hammer forges use a steam or air cylinder to raise the hammer, which is then dropped by gravity or is driven by steam or air. The number and force of the hammer blows are manually controlled by the operator. The operator often holds the cold end of the stock while operating the drop hammer. Drop hammer forging once comprised about two-thirds of all forging done in the United States, but is less common today.
Press forges use a mechanical or hydraulic ram to shape the piece with a single, slow, controlled stroke (see figure 1). Press forging is usually controlled automatically. It can be done hot or at normal temperatures (cold-forging, extruding). A variation on normal forging is rolling, where continuous applications of force are used and the operator turns the part.
Figure 1. Press forging

Die lubricants are sprayed or otherwise applied to die faces and blank surfaces before and between hammer or press strokes.
High-strength machine parts such as shafts, ring gears, bolts and vehicle suspension components are common steel forging products. High-strength aircraft components such as wing spars, turbine disks and landing gear are forged from aluminium, titanium or nickel and steel alloys. Approximately 3% of automotive workers are in forging operations or plants.
Working Conditions
Many hazards common in heavy industry are present in stamping and forging operations. These include repetitive strain injuries (RSIs) from repeated handling and processing of parts and operation of machine controls such as palm buttons. Heavy parts place workers at risk for back and shoulder problems as well as upper extremity musculoskeletal disorders. Press operators in automotive stamping plants have rates of RSIs that are comparable to those of assembly plant workers in high-risk jobs. High-impulse vibration and noise are present in most stamping and some forging (e.g., steam or air hammer) operations, causing hearing loss and possible cardiovascular illness; these are among the highest-noise industrial environments (over 100 dBA). As in other forms of automation-driven systems, worker energy loads can be high, depending on the parts handled and machine cycling rates.
Catastrophic injuries resulting from unanticipated machine movements are common in stamping and forging. These can be due to: (1) mechanical failure of machine control systems, such as clutch mechanisms in situations where workers are routinely expected to be within the machine operating envelope (an unacceptable process design); (2) deficiencies in machine design or performance that invite unprogrammed worker interventions such as moving jammed or misaligned parts; or (3) improper, high-risk maintenance procedures performed without adequate lockout of the entire machine network involved, including parts transfer automation and the functions of other connected machines. Most automated machine networks are not configured for quick, efficient and effective lockout or safe trouble-shooting.
Mists from machine lubricating oils generated during normal operation are another generic health hazard in stamping and forging press operations powered by compressed air, potentially putting workers at risk for respiratory, dermatological and digestive diseases.
Health and Safety Problems
Stamping
Stamping operations have high risk of severe laceration due to the required handling of parts with sharp edges. Possibly worse is the handling of the scrap resulting from cut-off perimeters and punched out sections of parts. Scrap is typically collected by gravity-fed chutes and conveyors. Clearing occasional jams is a high-risk activity.
Chemical hazards specific to stamping typically arise from two main sources: drawing compounds (i.e., die lubricants) in actual press operations and welding emissions from assembly of the stamped parts. Drawing compounds (DCs) are required for most stamping. The material is sprayed or rolled onto sheet metal and further mists are generated by the stamping event itself. Like other metalworking fluids, drawing compounds may be straight oils or oil emulsions (soluble oils). Components include petroleum oil fractions, special lubricity agents (e.g., animal and vegetable fatty acid derivatives, chlorinated oils and waxes), alkanolamines, petroleum sulphonates, borates, cellulose-derived thickeners, corrosion inhibitors and biocides. Air concentrations of mist in stamping operations may reach those of typical machining operations, although these levels tend to be lower on average (0.05 to 2.0 mg/m3). However, visible fog and accumulated oil film on building surfaces are often present, and skin contact may be higher due to extensive handling of parts. Exposures most likely to present hazards are chlorinated oils (possible cancer, liver disease, skin disorders), rosin or tall oil fatty acid derivatives (sensitizers), petroleum fractions (digestive cancers) and, possibly, formaldehyde (from biocides) and nitrosamines (from alkanolamines and sodium nitrite, either as DC ingredients or in surface coatings on incoming steel). Elevated digestive cancer has been observed in two automotive stamping plants. Microbiological blooms in systems that apply DCs by rolling it onto sheet metal from an open reservoir can pose risks to workers for respiratory and dermatological problems analogous to those in machining operations.
Welding of stamped parts is often performed in stamping plants, usually without intermediate washing. This produces emissions that include metal fumes and pyrolysis and combustion products from drawing compound and other surface residues. Typical (primarily resistance) welding operations in stamping plants generate total particulate air concentrations in the range 0.05 to 4.0 mg/m3. Metal content (as fumes and oxides) usually makes up less than half of that particulate matter, indicating that up to 2.0 mg/m3 is poorly characterized chemical debris. The result is haze visible in many stamping plant welding areas. The presence of chlorinated derivatives and other organic ingredients raises serious concerns over the composition of welding smoke in these settings and strongly argues for ventilation controls. Application of other materials prior to welding (such as primer, paint and epoxy-like adhesives), some of which are then welded over, adds further concern. Welding production repair activities, usually done manually, often pose higher exposures to these same air contaminants. Excess rates of lung cancer have been observed among welders in an automotive stamping plant.
Forging
Like stamping, forging operations can pose high laceration risks when workers handle forged parts or trim the flash or unwanted edges off parts. High impact forging can also eject fragments, scale or tools, causing injury. In some forging activities, the worker grasps the working piece with tongs during the pressing or impact steps, increasing the risk for musculoskeletal injuries. In forging, unlike stamping, furnaces for heating parts (for forging and annealing) as well as bins of hot forgings are usually nearby. These create potential for high heat stress conditions. Additional factors in heat stress are the worker’s metabolic load during manual handling of materials and, in some cases, heat from combustion products of oil-based die lubricants.
Die lubrication is required in most forging and has the added feature that the lubricant comes in contact with high-temperature parts. This causes immediate pyrolysis and aerosolization not only in the dies but also subsequently from smoking parts in cooling bins. Forging die lubricant ingredients can include graphite slurries, polymeric thickeners, sulphonate emulsifiers, petroleum fractions, sodium nitrate, sodium nitrite, sodium carbonate, sodium silicate, silicone oils and biocides. These are applied as sprays or, in some applications, by swab. Furnaces used for heating metal to be forged are usually fired by oil or gas, or they are induction furnaces. Emissions can result from fuel-fired furnaces with inadequate draft and from non-ventilated induction furnaces when incoming metal stock has surface contaminants, such as oil or corrosion inhibitors, or if, prior to forging, it was lubricated for shearing or sawing (as in the case of bar stock). In the US, total particulate air concentrations in forging operations typically range from 0.1 to 5.0 mg/m3 and vary widely within forging operations due to thermal convection currents. An elevated lung cancer rate was observed among forging and heat treatment workers from two ball-bearing manufacturing plants.
Health and Safety Practices
Few studies have evaluated actual health effects in workers with stamping or forging exposures. Comprehensive characterization of the toxicity potential of most routine operations, including identification and measurement of priority toxic agents, has not been done. Evaluating the long-term health effects of die lubrication technology developed in the 1960s and 1970s has only recently become feasible. As a result, regulation of these exposures defaults to generic dust or total particulate standards such as 5.0 mg/m3 in the US. While probably adequate in some circumstances, this standard is not demonstrably adequate for many stamping and forging applications.
Some reduction in die lubricant mist concentrations is possible with careful management of the application procedure in both stamping and forging. Roll application in stamping is preferred when feasible, and using minimal air pressure in sprays is beneficial. Possible elimination of priority hazardous ingredients should be investigated. Enclosures with negative pressure and mist collectors can be highly effective but may be incompatible with parts handling. Filtering air released from high-pressure air systems in presses would reduce press oil mist (and noise). Skin contact in stamping operations can be reduced with automation and good personal protective wear, providing protection against both laceration and liquid saturation. For stamping plant welding, washing parts prior to welding is highly desirable, and partial enclosures with LEV would reduce smoke levels substantially.
Controls to reduce heat stress in stamping and hot forging include minimizing the amount of manual material handling in high-heat areas, shielding of furnaces to reduce radiation of heat, minimizing the height of furnace doors and slots and using cooling fans. The location of cooling fans should be an integral part of the design of air movement to control mist exposures and heat stress; otherwise, cooling may be obtained only at the expense of higher exposures.
Mechanization of material handling, switching from hammer to press forging when possible and adjusting the work rate to ergonomically practical levels can reduce the number of musculoskeletal injuries.
Noise levels can be reduced through a combination of switching from hammer to press forges when possible, well-designed enclosures and quieting of furnace blowers, air clutches, air leads and parts handling. A hearing conservation programme should be instituted.
PPE needed includes head protection, foot protection, goggles, hearing protectors (around are as with excessive noise), heat- and oil-proof aprons and leggings (with heavy use of oil-based die lubricants) and infrared eye and face protection (around furnaces).
Environmental Health Hazards
The environmental hazards arising from stamping plants, relatively minor compared to those from some other types of plants, include disposal of waste drawing compound and washing solutions and the exhausting of welding smoke without adequate cleaning. Some forging plants historically have caused acute degradation of local air quality with forging smoke and scale dust. However, with appropriate air cleaning capacity, this need not occur. Disposition of stamping scrap and forging scale containing die lubricants is another potential issue.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."