- You are here:
-
Home

- Part VI. General Hazards

Children categories

36. Barometric Pressure Increased (2)

36. Barometric Pressure Increased
Chapter Editor: T.J.R. Francis
Table of Contents
Working under Increased Barometric Pressure
Eric Kindwall
Dees F. Gorman
Tables
Click a link below to view table in article context.
1. Instructions for compressed-air workers
2. Decompression illness: Revised classification
37. Barometric Pressure Reduced (4)
37. Barometric Pressure Reduced
Chapter Editor: Walter Dümmer
Table of Contents
Figures and Tables
Ventilatory Acclimatization to High Altitude
John T. Reeves and John V. Weil
Physiological Effects of Reduced Barometric Pressure
Kenneth I. Berger and William N. Rom
Health Considerations for Managing Work at High Altitudes
John B. West
Prevention of Occupational Hazards at High Altitudes
Walter Dümmer
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.







38. Biological Hazards (4)
38. Biological Hazards
Chapter Editor: Zuheir Ibrahim Fakhri
Table of Contents
Tables
Workplace Biohazards
Zuheir I. Fakhri
Aquatic Animals
D. Zannini
Terrestrial Venomous Animals
J.A. Rioux and B. Juminer
Clinical Features of Snakebite
David A. Warrell
Tables
Click a link below to view table in article context.
1. Occupational settings with biological agents
2. Viruses, bacteria, fungi & plants in the workplace
3. Animals as a source of occupational hazards
39. Disasters, Natural and Technological (12)
39. Disasters, Natural and Technological
Chapter Editor: Pier Alberto Bertazzi
Table of Contents
Tables and Figures
Disasters and Major Accidents
Pier Alberto Bertazzi
ILO Convention concerning the Prevention of Major Industrial Accidents, 1993 (No. 174)
Disaster Preparedness
Peter J. Baxter
Post-Disaster Activities
Benedetto Terracini and Ursula Ackermann-Liebrich
Weather-Related Problems
Jean French
Avalanches: Hazards and Protective Measures
Gustav Poinstingl
Transportation of Hazardous Material: Chemical and Radioactive
Donald M. Campbell
Radiation Accidents
Pierre Verger and Denis Winter
Case Study: What does dose mean?
Occupational Health and Safety Measures in Agricultural Areas Contaminated by Radionuclides: The Chernobyl Experience
Yuri Kundiev, Leonard Dobrovolsky and V.I. Chernyuk
Case Study: The Kader Toy Factory Fire
Casey Cavanaugh Grant
Impacts of Disasters: Lessons from a Medical Perspective
José Luis Zeballos
Tables
Click a link below to view table in article context.
1. Definitions of disaster types
2. 25-yr average # victims by type & region-natural trigger
3. 25-yr average # victims by type & region-non-natural trigger
4. 25-yr average # victims by type-natural trigger (1969-1993)
5. 25-yr average # victims by type-non-natural trigger (1969-1993)
6. Natural trigger from 1969 to 1993: Events over 25 years
7. Non-natural trigger from 1969 to 1993: Events over 25 years
8. Natural trigger: Number by global region & type in 1994
9. Non-natural trigger: Number by global region & type in 1994
10. Examples of industrial explosions
11. Examples of major fires
12. Examples of major toxic releases
13. Role of major hazard installations management in hazard control
14. Working methods for hazard assessment
15. EC Directive criteria for major hazard installations
16. Priority chemicals used in identifying major hazard installations
17. Weather-related occupational risks
18. Typical radionuclides, with their radioactive half-lives
19. Comparison of different nuclear accidents
20. Contamination in Ukraine, Byelorussia & Russia after Chernobyl
21. Contamination strontium-90 after the Khyshtym accident (Urals 1957)
22. Radioactive sources that involved the general public
23. Main accidents involving industrial irradiators
24. Oak Ridge (US) radiation accident registry (worldwide, 1944-88)
25. Pattern of occupational exposure to ionizing radiation worldwide
26. Deterministic effects: thresholds for selected organs
27. Patients with acute irradiation syndrome (AIS) after Chernobyl
28. Epidemiological cancer studies of high dose external irradiation
29. Thyroid cancers in children in Belarus, Ukraine & Russia, 1981-94
30. International scale of nuclear incidents
31. Generic protective measures for general population
32. Criteria for contamination zones
33. Major disasters in Latin America & the Caribbean, 1970-93
34. Losses due to six natural disasters
35. Hospitals & hospital beds damaged/ destroyed by 3 major disasters
36. Victims in 2 hospitals collapsed by the 1985 earthquake in Mexico
37. Hospital beds lost resulting from the March 1985 Chilean earthquake
38. Risk factors for earthquake damage to hospital infrastructure
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|














Click to return to top of page
40. Electricity (3)
40. Electricity
Chapter Editor: Dominique Folliot
Table of Contents
Figures and Tables
Electricity—Physiological Effects
Dominique Folliot
Static Electricity
Claude Menguy
Prevention And Standards
Renzo Comini
Tables
Click a link below to view table in article context.
1. Estimates of the rate of electrocution-1988
2. Basic relationships in electrostatics-Collection of equations
3. Electron affinities of selected polymers
4. Typical lower flammability limits
5. Specific charge associated with selected industrial operations
6. Examples of equipment sensitive to electrostatic discharges
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.



41. Fire (6)
41. Fire
Chapter Editor: Casey C. Grant
Table of Contents
Figures and Tables
Basic Concepts
Dougal Drysdale
Sources of Fire Hazards
Tamás Bánky
Fire Prevention Measures
Peter F. Johnson
Passive Fire Protection Measures
Yngve Anderberg
Active Fire Protection Measures
Gary Taylor
Organizing for Fire Protection
S. Dheri
Tables
Click a link below to view table in article context.
1. Lower & upper flammability limits in air
2. Flashpoints & firepoints of liquid & solid fuels
3. Ignition sources
4. Comparison of concentrations of different gases required for inerting
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.











42. Heat and Cold (12)
42. Heat and Cold
Chapter Editor: Jean-Jacques Vogt
Table of Contents
Figures and Tables
Physiological Responses to the Thermal Environment
W. Larry Kenney
Effects of Heat Stress and Work in the Heat
Bodil Nielsen
Heat Disorders
Tokuo Ogawa
Prevention of Heat Stress
Sarah A. Nunneley
The Physical Basis of Work in Heat
Jacques Malchaire
Assessment of Heat Stress and Heat Stress Indices
Kenneth C. Parsons
Case Study: Heat Indices: Formulae and Definitions
Heat Exchange through Clothing
Wouter A. Lotens
Cold Environments and Cold Work
Ingvar Holmér, Per-Ola Granberg and Goran Dahlstrom
Prevention of Cold Stress in Extreme Outdoor Conditions
Jacques Bittel and Gustave Savourey
Cold Indices and Standards
Ingvar Holmér
Tables
Click a link below to view table in article context.
1. Electrolyte concentration in blood plasma & sweat
2. Heat Stress Index & Allowable Exposure Times: calculations
3. Interpretation of Heat Stress Index values
4. Reference values for criteria of thermal stress & strain
5. Model using heart rate to assess heat stress
6. WBGT reference values
7. Working practices for hot environments
8. Calculation of the SWreq index & assessment method: equations
9. Description of terms used in ISO 7933 (1989b)
10. WBGT values for four work phases
11. Basic data for the analytical assessment using ISO 7933
12. Analytical assessment using ISO 7933
13. Air temperatures of various cold occupational environments
14. Duration of uncompensated cold stress & associated reactions
15. Indication of anticipated effects of mild & severe cold exposure
16. Body tissue temperature & human physical performance
17. Human responses to cooling: Indicative reactions to hypothermia
18. Health recommendations for personnel exposed to cold stress
19. Conditioning programmes for workers exposed to cold
20. Prevention & alleviation of cold stress: strategies
21. Strategies & measures related to specific factors & equipment
22. General adaptational mechanisms to cold
23. Number of days when water temperature is below 15 ºC
24. Air temperatures of various cold occupational environments
25. Schematic classification of cold work
26. Classification of levels of metabolic rate
27. Examples of basic insulation values of clothing
28. Classification of thermal resistance to cooling of handwear
29. Classification of contact thermal resistance of handwear
30. Wind Chill Index, temperature & freezing time of exposed flesh
31. Cooling power of wind on exposed flesh
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|


























43. Hours of Work (1)
43. Hours of Work
Chapter Editor: Peter Knauth
Table of Contents
Hours of Work
Peter Knauth
Tables
Click a link below to view table in article context.
1. Time intervals from beginning shiftwork until three illnesses
2. Shiftwork & incidence of cardiovascular disorders
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.









44. Indoor Air Quality (8)
44. Indoor Air Quality
Chapter Editor: Xavier Guardino Solá
Table of Contents
Figures and Tables
Indoor Air Quality: Introduction
Xavier Guardino Solá
Nature and Sources of Indoor Chemical Contaminants
Derrick Crump
Radon
María José Berenguer
Tobacco Smoke
Dietrich Hoffmann and Ernst L. Wynder
Smoking Regulations
Xavier Guardino Solá
Measuring and Assessing Chemical Pollutants
M. Gracia Rosell Farrás
Biological Contamination
Brian Flannigan
Regulations, Recommendations, Guidelines and Standards
María José Berenguer
Tables
Click a link below to view table in article context.
1. Classification of indoor organic pollutants
2. Formaldehyde emission from a variety of materials
3. Ttl. volatile organic comp’ds concs, wall/floor coverings
4. Consumer prods & other sources of volatile organic comp’ds
5. Major types & concentrations in the urban United Kingdom
6. Field measurements of nitrogen oxides & carbon monoxide
7. Toxic & tumorigenic agents in cigarette sidestream smoke
8. Toxic & tumorigenic agents from tobacco smoke
9. Urinary cotinine in non-smokers
10. Methodology for taking samples
11. Detection methods for gases in indoor air
12. Methods used for the analysis of chemical pollutants
13. Lower detection limits for some gases
14. Types of fungus which can cause rhinitis and/or asthma
15. Micro-organisms and extrinsic allergic alveolitis
16. Micro-organisms in nonindustrial indoor air & dust
17. Standards of air quality established by the US EPA
18. WHO guidelines for non-cancer and non-odour annoyance
19. WHO guideline values based on sensory effects or annoyance
20. Reference values for radon of three organizations
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|





45. Indoor Environmental Control (6)
45. Indoor Environmental Control
Chapter Editor: Juan Guasch Farrás
Table of Contents
Figures and Tables
Control of Indoor Environments: General Principles
A. Hernández Calleja
Indoor Air: Methods for Control and Cleaning
E. Adán Liébana and A. Hernández Calleja
Aims and Principles of General and Dilution Ventilation
Emilio Castejón
Ventilation Criteria for Nonindustrial Buildings
A. Hernández Calleja
Heating and Air-Conditioning Systems
F. Ramos Pérez and J. Guasch Farrás
Indoor Air: Ionization
E. Adán Liébana and J. Guasch Farrás
Tables
Click a link below to view table in article context.
1. Most common indoor pollutants & their sources
2. Basic requirements-dilution ventilation system
3. Control measures & their effects
4. Adjustments to working environment & effects
5. Effectiveness of filters (ASHRAE standard 52-76)
6. Reagents used as absorbents for contaminents
7. Levels of quality of indoor air
8. Contamination due to the occupants of a building
9. Degree of occupancy of different buildings
10. Contamination due to the building
11. Quality levels of outside air
12. Proposed norms for environmental factors
13. Temperatures of thermal comfort (based on Fanger)
14. Characteristics of ions
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|













46. Lighting (3)
46. Lighting
Chapter Editor: Juan Guasch Farrás
Table of Contents
Figures and Tables
Types of Lamps and Lighting
Richard Forster
Conditions Required for Visual
Fernando Ramos Pérez and Ana Hernández Calleja
General Lighting Conditions
N. Alan Smith
Tables
Click a link below to view table in article context.
1. Improved output & wattage of some 1,500 mm fluorescent tube lamps
2. Typical lamp efficacies
3. International Lamp Coding System (ILCOS) for some lamp types
4. Common colours & shapes of incandescent lamps & ILCOS codes
5. Types of high-pressure sodium lamp
6. Colour contrasts
7. Reflection factors of different colours & materials
8. Recommended levels of maintained illuminance for locations/tasks
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|





























47. Noise (5)
47. Noise
Chapter Editor: Alice H. Suter
Table of Contents
Figures and Tables
The Nature and Effects of Noise
Alice H. Suter
Noise Measurement and Exposure Evaluation
Eduard I. Denisov and German A. Suvorov
Engineering Noise Control
Dennis P. Driscoll
Hearing Conservation Programmes
Larry H. Royster and Julia Doswell Royster
Standards and Regulations
Alice H. Suter
Tables
Click a link below to view table in article context.
1. Permissible exposure limits (PEL)for noise exposure, by nation
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.









48. Radiation: Ionizing (6)
48. Radiation: Ionizing
Chapter Editor: Robert N. Cherry, Jr.
Table of Contents
Introduction
Robert N. Cherry, Jr.
Radiation Biology and Biological Effects
Arthur C. Upton
Sources of Ionizing Radiation
Robert N. Cherry, Jr.
Workplace Design for Radiation Safety
Gordon M. Lodde
Radiation Safety
Robert N. Cherry, Jr.
Planning for and Management of Radiation Accidents
Sydney W. Porter, Jr.
49. Radiation, Non-Ionizing (9)
49. Radiation, Non-Ionizing
Chapter Editor: Bengt Knave
Table of Contents
Tables and Figures
Electric and Magnetic Fields and Health Outcomes
Bengt Knave
The Electromagnetic Spectrum: Basic Physical Characteristics
Kjell Hansson Mild
Ultraviolet Radiation
David H. Sliney
Infrared Radiation
R. Matthes
Light and Infrared Radiation
David H. Sliney
Lasers
David H. Sliney
Radiofrequency Fields and Microwaves
Kjell Hansson Mild
VLF and ELF Electric and Magnetic Fields
Michael H. Repacholi
Static Electric and Magnetic Fields
Martino Grandolfo
Tables
Click a link below to view table in article context.
1. Sources and exposures for IR
2. Retinal thermal hazard function
3. Exposure limits for typical lasers
4. Applications of equipment using range >0 to 30 kHz
5. Occupational sources of exposure to magnetic fields
6. Effects of currents passing through the human body
7. Biological effects of various current density ranges
8. Occupational exposure limits-electric/magnetic fields
9. Studies on animals exposed to static electric fields
10. Major technologies and large static magnetic fields
11. ICNIRP recommendations for static magnetic fields
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|








50. Vibration (4)
50. Vibration
Chapter Editor: Michael J. Griffin
Table of Contents
Table and Figures
Vibration
Michael J. Griffin
Whole-body Vibration
Helmut Seidel and Michael J. Griffin
Hand-transmitted Vibration
Massimo Bovenzi
Motion Sickness
Alan J. Benson
Tables
Click a link below to view table in article context.
1. Activities with adverse effects of whole-body vibration
2. Preventive measures for whole-body vibration
3. Hand-transmitted vibration exposures
4. Stages, Stockholm Workshop scale, hand-arm vibration syndrome
5. Raynaud’s phenomenon & hand-arm vibration syndrome
6. Threshold limit values for hand-transmitted vibration
7. European Union Council Directive: Hand-transmitted vibration (1994)
8. Vibration magnitudes for finger blanching
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|







51. Violence (1)
51. Violence
Chapter Editor: Leon J. Warshaw
Table of Contents
Violence in the Workplace
Leon J. Warshaw
Tables
Click a link below to view table in article context.
1. Highest rates of occupational homicide, US workplaces, 1980-1989
2. Highest rates of occupational homicide US occupations, 1980-1989
3. Risk factors for workplace homicides
4. Guides for programmes to prevent workplace violence
52. Visual Display Units (11)
52. Visual Display Units
Chapter Editor: Diane Berthelette
Table of Contents
Tables and Figures
Overview
Diane Berthelette
Characteristics of Visual Display Workstations
Ahmet Çakir
Ocular and Visual Problems
Paule Rey and Jean-Jacques Meyer
Reproductive Hazards - Experimental Data
Ulf Bergqvist
Reproductive Effects - Human Evidence
Claire Infante-Rivard
Case Study: A Summary of Studies of Reproductive Outcomes
Musculoskeletal Disorders
Gabriele Bammer
Skin Problems
Mats Berg and Sture Lidén
Psychosocial Aspects of VDU Work
Michael J. Smith and Pascale Carayon
Ergonomic Aspects of Human - Computer Interaction
Jean-Marc Robert
Ergonomics Standards
Tom F.M. Stewart
Tables
Click a link below to view table in article context.
1. Distribution of computers in various regions
2. Frequency & importance of elements of equipment
3. Prevalence of ocular symptoms
4. Teratological studies with rats or mice
5. Teratological studies with rats or mice
6. VDU use as a factor in adverse pregnancy outcomes
7. Analyses to study causes musculoskeletal problems
8. Factors thought to cause musculoskeletal problems
Figures
Point to a thumbnail to see figure caption, click to see figure in article context.
|
|












Working Under Increased Barometric Pressure
The atmosphere normally consists of 20.93% oxygen. The human body is naturally adapted to breathe atmospheric oxygen at a pressure of approximately 160 torr at sea level. At this pressure, haemoglobin, the molecule which carries oxygen to the tissue, is approximately 98% saturated. Higher pressures of oxygen cause little important increase in oxyhaemoglobin, since its concentration is virtually 100% to begin with. However, significant amounts of unburnt oxygen may pass into physical solution in the blood plasma as the pressure rises. Fortunately, the body can tolerate a fairly wide range of oxygen pressures without appreciable harm, at least in the short term. Longer term exposures may lead to oxygen toxicity problems.
When a job requires breathing compressed air, as in diving or caisson work, oxygen deficiency (hypoxia) is rarely a problem, as the body will be exposed to an increasing amount of oxygen as the absolute pressure rises. Doubling the pressure will double the number of molecules inhaled per breath while breathing compressed air. Thus the amount of oxygen breathed is effectively equal to 42%. In other words, a worker breathing air at a pressure of 2 atmospheres absolute (ATA), or 10 m beneath the sea, will breathe an amount of oxygen equal to breathing 42% oxygen by mask on the surface.
Oxygen toxicity
On the earth’s surface, human beings can safely continuously breathe 100% oxygen for between 24 and 36 hours. After that, pulmonary oxygen toxicity ensues (the Lorrain-Smith effect). The symptoms of lung toxicity consist of substernal chest pain; dry, non-productive cough; a drop in the vital capacity; loss of surfactant production. A condition known as patchy atelectasis is seen on x-ray examination, and with continued exposure microhaemorrhages and ultimately production of permanent fibrosis in the lung will develop. All stages of oxygen toxicity through the microhaemorrhage state are reversible, but once fibrosis sets in, the scarring process becomes irreversible. When 100% oxygen is breathed at 2 ATA, (a pressure of 10 m of sea water), the early symptoms of oxygen toxicity become manifest after about six hours. It should be noted that interspersing short, five-minute periods of air breathing every 20 to 25 minutes can double the length of time required for symptoms of oxygen toxicity to appear.
Oxygen can be breathed at pressures below 0.6 ATA without ill effect. For example, a worker can tolerate 0.6 atmosphere oxygen breathed continuously for two weeks without any loss of vital capacity. The measurement of vital capacity appears to be the most sensitive indicator of early oxygen toxicity. Divers working at great depths may breathe gas mixtures containing up to 0.6 atmospheres oxygen with the rest of the breathing medium consisting of helium and/or nitrogen. Six tenths of an atmosphere corresponds to breathing 60% oxygen at 1 ATA or at sea level.
At pressures greater than 2 ATA, pulmonary oxygen toxicity no longer becomes the primary concern, as oxygen can cause seizures secondary to cerebral oxygen toxicity. Neurotoxicity was first described by Paul Bert in 1878 and is known as the Paul Bert effect. If a person were to breathe 100% oxygen at a pressure of 3 ATA for much longer than three continuous hours, he or she will very likely suffer a grand mal seizure. Despite over 50 years of active research as to the mechanism of oxygen toxicity of the brain and lung, this response is still not completely understood. Certain factors are known, however, to enhance toxicity and to lower the seizure threshold. Exercise, CO2 retention, use of steroids, presence of fever, chilling, ingestion of amphetamines, hyperthyroidism and fear can have an oxygen tolerance effect. An experimental subject lying quietly in a dry chamber at pressure has much greater tolerance than a diver who is working actively in cold water underneath an enemy ship, for example. A military diver may experience cold, hard exercise, probable CO2 build-up using a closed-circuit oxygen rig, and fear, and may experience a seizure within 10-15 minutes working at a depth of only 12 m, whereas a patient lying quietly in a dry chamber may easily tolerate 90 minutes at a pressure of 20 m without great danger of seizure. Exercising divers may be exposed to partial pressure of oxygen up to 1.6 ATA for short periods up to 30 minutes, which corresponds to breathing 100% oxygen at a depth of 6 m. It is important to note that one should never expose anyone to 100% oxygen at a pressure greater than 3 ATA, nor for a time longer than 90 minutes at that pressure, even with a subject quietly recumbent.
There is considerable individual variation in susceptibility to seizure between individuals and, surprisingly, within the same individual, from day to day. For this reason, “oxygen tolerance” tests are essentially meaningless. Giving seizure-suppressing drugs, such as phenobarbital or phenytoin, will prevent oxygen seizures but do nothing to mitigate permanent brain or spinal cord damage if pressure or time limits are exceeded.
Carbon monoxide
Carbon monoxide can be a serious contaminant of the diver’s or caisson worker’s breathing air. The most common sources are internal combustion engines, used to power compressors, or other operating machinery in the vicinity of the compressors. Care should be taken to be sure that compressor air intakes are well clear of any sources of engine exhaust. Diesel engines usually produce little carbon monoxide but do produce large quantities of oxides of nitrogen, which can produce serious toxicity to the lung. In the United States, the current federal standard for carbon monoxide levels in inspired air is 35 parts per million (ppm) for an 8-hour working day. For example, at the surface even 50 ppm would not produce detectable harm, but at a depth of 50 m it would be compressed and produce the effect of 300 ppm. This concentration can produce a level of up to 40% carboxyhaemoglobin over a period of time. The actual analysed parts per million must be multiplied by the number of atmospheres at which it is delivered to the worker.
Divers and compressed-air workers should become aware of the early symptoms of carbon monoxide poisoning, which include headache, nausea, dizziness and weakness. It is important to ensure that the compressor intake be always located upwind from the compressor engine exhaust pipe. This relationship must be continually checked as the wind changes or the vessels position shifts.
For many years it was widely assumed that carbon monoxide would combine with the body’s haemoglobin to produce carboxyhaemoglobin, causing its lethal effect by blocking transport of oxygen to the tissues. More recent work shows that although this effect does cause tissue hypoxia, it is not in itself fatal. The most serious damage occurs at the cellular level due to direct toxicity of the carbon monoxide molecule. Lipid peroxidation of cell membranes, which can only be terminated by hyperbaric oxygen treatment, appears to be the main cause of death and long-term sequelae.
Carbon dioxide
Carbon dioxide is a normal product of metabolism and is eliminated from the lungs through the normal process of respiration. Various types of breathing apparatus, however, can impair its elimination or cause high levels to build up in the diver’s inspired air.
From a practical point of view, carbon dioxide can exert deleterious effects on the body in three ways. First, in very high concentrations (above 3%), it can cause judgmental errors, which at first may amount to inappropriate euphoria, followed by depression if the exposure is prolonged. This, of course, can have serious consequences for a diver under water who wants to maintain good judgement to remain safe. As the concentration climbs, CO2 will eventually produce unconsciousness when levels rise much above 8%. A second effect of carbon dioxide is to exacerbate or worsen nitrogen narcosis (see below). At partial pressures of above 40 mm Hg, carbon dioxide begins to have this effect (Bennett and Elliot 1993). At high PO2‘s, such as one is exposed to in diving, the respiratory drive due to high CO2 is attenuated and it is possible under certain conditions for divers who tend to retain CO2 to increase their levels of carbon dioxide sufficient to render them unconscious. The final problem with carbon dioxide under pressure is that, if the subject is breathing 100% oxygen at pressures greater than 2 ATA, the risk for seizures is greatly enhanced as carbon dioxide levels rise. Submarine crews have easily tolerated breathing 1.5% CO2 for two months at a time with no functional ill effect, a concentration that is thirty times the normal concentration found in atmospheric air. Five thousand ppm, or ten times the level found in normal fresh air, is considered safe for the purposes of industrial limits. However, even 0.5% CO2 added to 100% oxygen mix will predispose a person to seizures when breathed at increased pressure.
Nitrogen
Nitrogen is an inert gas with regard to normal human metabolism. It does not enter into any form of chemical combination with compounds or chemicals within the body. However, it is responsible for severe impairment in a diver’s mental functioning when breathed under high pressure.
Nitrogen behaves as an aliphatic anaesthetic as atmospheric pressure increases, which results in the concentration of nitrogen also increasing. Nitrogen fits well into the Meyer-Overton hypothesis which states that any aliphatic anaesthetic will exhibit anaesthetic potency in direct proportion to its oil-water solubility ratio. Nitrogen, which is five times more soluble in fat than in water, produces an anaesthetic effect precisely at the predicted ratio.
In actual practice, diving to depths of 50 m can be accomplished with compressed-air, although the effects of nitrogen narcosis first become evident between 30 and 50 m. Most divers, however, can function adequately within these parameters. Deeper than 50 m, helium/oxygen mixtures are commonly used to avoid the effects of nitrogen narcosis. Air diving has been done to depths of slightly over 90 m, but at these extreme pressures, the divers were barely able to function and could hardly remember what tasks they had been sent down to accomplish. As noted earlier, any excess CO2 build-up further worsens the effect of nitrogen. Because ventilatory mechanics are affected by the density of gas at great pressures, there is an automatic CO2 build-up in the lung because of changes in laminar flow within the bronchioles and the diminution of the respiratory drive. Thus, air diving deeper than 50 m can be extremely dangerous.
Nitrogen exerts its effect by its simple physical presence dissolved in neural tissue. It causes a slight swelling of the neuronal cell membrane, which makes it more permeable to sodium and potassium ions. It is felt that interference with the normal depolarization/repolarization process is responsible for clinical symptoms of nitrogen narcosis.
Decompression
Decompression tables
A decompression table sets out the schedule, based on depth and time of exposure, for decompressing a person who has been exposed to hyperbaric conditions. Some general statements can be made about decompression procedures. No decompression table can be guaranteed to avoid decompression illness (DCI) for everyone, and indeed as described below, many problems have been noted with some tables currently in use. It must be remembered that bubbles are produced during every normal decompression, no matter how slow. For this reason, although it can be stated that the longer the decompression the less the likelihood of DCI, at the extreme of least likelihood, DCI becomes an essentially random event.
Habituation
Habituation, or acclimatization, occurs in divers and compressed-air workers, and renders them less susceptible to DCI after repeated exposures. Acclimatization can be produced after about a week of daily exposure, but it is lost after an absence from work of between 5 days to a week or by a sudden increase in pressure. Unfortunately construction companies have relied on acclimatization to make work possible with what are viewed as grossly inadequate decompression tables. To maximize the utility of acclimatization, new workers are often started at midshift to allow them to habituate without getting DCI. For example, the present Japanese Table 1 for compressed-air workers utilizes the split shift, with a morning and afternoon exposure to compressed air with a surface interval of one hour between exposures. Decompression from the first exposure is about 30% of that required by the US Navy and the decompression from the second exposure is only 4% of that required by the Navy. Nevertheless, habituation makes this departure from physiologic decompression possible. Workers with even ordinary susceptibility to decompression illness self-select themselves out of compressed-air work.
The mechanism of habituation or acclimatization is not understood. However, even if the worker is not experiencing pain, damage to brain, bone, or tissue may be taking place. Up to four times as many changes are visible on MRIs taken of the brains of compressed-air workers compared to age-matched controls that have been studied (Fueredi, Czarnecki and Kindwall 1991). These probably reflect lacunar infarcts.
Diving decompression
Most modern decompression schedules for divers and caisson workers are based on mathematical models akin to those developed originally by J.S. Haldane in 1908 when he made some empirical observations on permissible decompression parameters. Haldane observed that a pressure reduction of one half could be tolerated in goats without producing symptoms. Using this as a starting point, he then, for mathematical convenience, conceived of five different tissues in the body loading and unloading nitrogen at varying rates based on the classical half time equation. His staged decompression tables were then designed to avoid exceeding a 2:1 ratio in any of the tissues. Over the years, Haldane’s model has been modified empirically in attempts to make it fit what divers were observed to tolerate. However, all mathematical models for the loading and elimination of gases are flawed, since there are no decompression tables which remain as safe or become safer as time and depth are increased.
Probably the most reliable decompression tables currently available for air diving are those of the Canadian Navy, known as the DCIEM tables (Defence and Civil Institute of Environmental Medicine). These tables were tested thoroughly by non-habituated divers over a wide range of conditions and produce a very low rate of decompression illness. Other decompression schedules which have been well tested in the field are the French National Standards, originally developed by Comex, the French diving company.
The US Navy Air Decompression tables are unreliable, especially when pushed to their limits. In actual use, US Navy Master Divers routinely decompress for a depth 3 m (10 ft) deeper and/or one exposure time segment longer than required for the actual dive to avoid problems. The Exceptional Exposure Air Decompression Tables are particularly unreliable, having produced decompression illness on 17% to 33% of all the test dives. In general, the US Navy’s decompression stops are probably too shallow.
Tunnelling and caisson decompression
None of the air decompression tables which call for air breathing during decompression, currently in wide use, appear to be safe for tunnel workers. In the United States, the current federal decompression schedules (US Bureau of Labor Statuties 1971), enforced by the Occupational Safety and Health Administration (OSHA), have been shown to produce DCI in one or more workers on 42% of the working days while being used at pressures between 1.29 and 2.11 bar. At pressures over 2.45 bar, they have been shown to produce a 33% incidence of aseptic necrosis of the bone (dysbaric osteonecrosis). The British Blackpool Tables are also flawed. During the building of the Hong Kong subway, 83% of the workers using these tables complained of symptoms of DCI. They have also been shown to produce an incidence of dysbaric osteonecrosis of up to 8% at relatively modest pressures.
The new German oxygen decompression tables devised by Faesecke in 1992 have been used with good success in a tunnel under the Kiel Canal. The new French oxygen tables also appear to be excellent by inspection but have not yet been used on a large project.
Using a computer which examined 15 years of data from successful and unsuccessful commercial dives, Kindwall and Edel devised compressed-air caisson decompression tables for the US National Institute for Occupational Safety and Health in 1983 (Kindwall, Edel and Melton 1983) using an empirical approach which avoided most of the pitfalls of mathematical modelling. Modelling was used only to interpolate between real data points. The research upon which these tables was based found that when air was breathed during decompression, the schedule in the tables did not produce DCI. However, the times used were prohibitively long and therefore impractical for the construction industry. When an oxygen variant of the table was computed, however, it was found that decompression time could be shortened to times similar to, or even shorter than, the current OSHA-enforced air decompression tables cited above. These new tables were subsequently tested by non-habituated subjects of varying ages at pressures ranging from 0.95 bar to 3.13 bar in 0.13 bar increments. Average work levels were simulated by weight lifting and treadmill walking during exposure. Exposure times were as long as possible, in keeping with the combined work time and decompression time fitting into an eight-hour work day. These are the only schedules which will be used in actual practice for shift work. No DCI was reported during these tests and bone scan and x ray failed to reveal any dysbaric osteonecrosis. To date, these are the only laboratory-tested decompression schedules in existence for compressed-air workers.
Decompression of hyperbaric chamber personnel
US Navy air decompression schedules were designed to produce a DCI incidence of less than 5%. This is satisfactory for operational diving, but much too high to be acceptable for hyperbaric workers who work in clinical settings. Decompression schedules for hyperbaric chamber attendants can be based on naval air decompression schedules, but since exposures are so frequent and thus are usually at the limits of the table, they must be liberally lengthened and oxygen should be substituted for compressed-air breathing during decompression. As a prudent measure, it is recommended that a two-minute stop be made while breathing oxygen, at least three metres deeper than called for by the decompression schedule chosen. For example, while the US Navy requires a three-minute decompression stop at three metres, breathing air, after a 101 minute exposure at 2.5 ATA, an acceptable decompression schedule for a hyperbaric chamber attendant undergoing the same exposure would be a two-minute stop at 6 m breathing oxygen, followed by ten minutes at 3 m breathing oxygen. When these schedules, modified as above, are used in practice, DCI in an inside attendant is an extreme rarity (Kindwall 1994a).
In addition to providing a fivefold larger “oxygen window” for nitrogen elimination, oxygen breathing offers other advantages. Raising the PO2 in venous blood has been demonstrated to lessen blood sludging, reduce the stickiness of white cells, reduce the no-reflow phenomenon, render red cells more flexible in passing through capillaries and counteract the vast decrease in deformability and filterability of white cells which have been exposed to compressed air.
Needless to say, all workers using oxygen decompression must be thoroughly trained and apprised of the fire danger. The environment of the decompression chamber must be kept free of combustibles and ignition sources, an overboard dump system must be used to convey exhaled oxygen out of the chamber and redundant oxygen monitors with a high oxygen alarm must be provided. The alarm should sound if oxygen in the chamber atmosphere exceeds 23%.
Working with compressed air or treating clinical patients under hyperbaric conditions sometimes can accomplish work or effect remission in disease that would otherwise be impossible. When rules for the safe use of these modalities are observed, workers need not be at significant risk for dysbaric injury.
Caisson Work and Tunnelling
From time to time in the construction industry it is necessary to excavate or tunnel through ground which is either fully saturated with water, lying below the local water table, or following a course completely under water, such as a river or lake bottom. A time-tested method for managing this situation has been to apply compressed air to the working area to force water out of the ground, drying it sufficiently so that it can be mined. This principle has been applied to both caissons used for bridge pier construction and soft ground tunnelling (Kindwall 1994b).
Caissons
A caisson is simply a large, inverted box, made to the dimensions of the bridge foundation, which typically is built in a dry dock and then floated into place, where it is carefully positioned. It is then flooded and lowered until it touches bottom, after which it is driven down further by adding weight as the bridge pier itself is constructed. The purpose of the caisson is to provide a method for cutting through soft ground to land the bridge pier on solid rock or a good geologic weight-bearing stratum. When all sides of the caisson have been embedded in the mud, compressed air is applied to the interior of the caisson and water is forced out, leaving a muck floor which can be excavated by men working within the caisson. The edges of the caisson consist of a wedge-shaped cutting shoe, made of steel, which continues to descend as earth is removed beneath the descending caisson and weight is applied from above as the bridge tower is constructed. When bed rock is reached, the working chamber is filled with concrete, becoming the permanent base for the bridge foundation.
Caissons have been used for nearly 150 years and have been successful in the construction of foundations as deep as 31.4 m below mean high water, as on Bridge Pier No. 3 of the Auckland, New Zealand, Harbour Bridge in 1958.
Design of the caisson usually provides for an access shaft for workers, who can descend either by ladder or by a mechanical lift and a separate shaft for buckets to remove the spoil. The shafts are provided with hermetically sealed hatches at either end which enable the caisson pressure to remain the same while workers or materials exit or enter. The top hatch of the muck shaft is provided with a pressure sealed gland through which the hoist cable for the muck bucket can slide. Before the top hatch is opened, the lower hatch is shut. Hatch interlocks may be necessary for safety, depending on design. Pressure must be equal on both sides of any hatch before it can be opened. Since the walls of the caisson are generally made of steel or concrete, there is little or no leakage from the chamber while under pressure except under the edges. The pressure is raised incrementally to a pressure just slightly greater than is necessary to balance off sea pressure at the edge of the cutting shoe.
People working in the pressurized caisson are exposed to compressed air and may experience many of the same physiologic problems that face deep-sea divers. These include decompression illness, barotrauma of the ears, sinus cavities and lungs and if decompression schedules are inadequate, the long-term risk of aseptic necrosis of the bone (dysbaric osteonecrosis).
It is important that a ventilation rate be established to carry away CO2 and gases emanating from the muck floor (especially methane) and whatever fumes may be produced from welding or cutting operations in the working chamber. A rule of thumb is that six cubic metres of free air per minute must be provided for each worker in the caisson. Allowance must also be made for air which is lost when the muck lock and man lock are used for the passage of personnel and materials. As the water is forced down to a level exactly even with the cutting shoe, ventilation air is required as the excess bubbles out under the edges. A second air supply, equal in capacity to the first, with an independent power source, should be available for emergency use in case of compressor or power failure. In many areas this is required by law.
Sometimes if the ground being mined is homogeneous and consists of sand, blow pipes can be erected to the surface. The pressure in the caisson will then extract the sand from the working chamber when the end of the blow pipe is located in a sump and the excavated sand is shovelled into the sump. If coarse gravel, rock, or boulders are encountered, these have to be broken up and removed in conventional muck buckets.
If the caisson should fail to sink despite the added weight on top, it may sometimes be necessary to withdraw the workers from the caisson and reduce the air pressure in the working chamber to allow the caisson to fall. Concrete must be placed or water admitted to the wells within the pier structure surrounding the air shafts above the caisson to reduce the stress on the diaphragm at the top of the working chamber. When just beginning a caisson operation, safety cribs or supports should be kept in the working chamber to prevent the caisson from suddenly dropping and crushing the workers. Practical considerations limit the depth to which air-filled caissons can be driven when men are used to hand mine the muck. A pressure of 3.4 kg/cm2 gauge (3.4 bar or 35 m of fresh water) is about the maximum tolerable limit because of decompression considerations for the workers.
An automated caisson excavating system has been developed by the Japanese wherein a remotely operated hydraulically powered backhoe shovel, which can reach all corners of the caisson, is used for excavation. The backhoe, under television control from the surface, drops the excavated muck into buckets which are hoisted remotely from the caisson. Using this system, the caisson can proceed down to almost unlimited pressures. The only time that workers need enter the working chamber is to repair the excavating machinery or to remove or demolish large obstacles which appear below the cutting shoe of the caisson and which cannot be removed by the remote-controlled backhoe. In such cases, workers enter for short periods much as divers and can breathe either air or mixed gas at higher pressures to avoid nitrogen narcosis.
When people have worked long shifts under compressed-air at pressures greater than 0.8 kg/cm2 (0.8 bar), they must decompress in stages. This can be accomplished either by attaching a large decompression chamber to the top of the man shaft into the caisson or, if space requirements are such at the top that this is impossible, by attaching “blister locks” to the man shaft. These are small chambers which can accommodate only a few workers at a time in a standing position. Preliminary decompression is taken in these blister locks, where the time spent is relatively short. Then, with considerable excess gas remaining in their bodies, the workers rapidly decompress to the surface and quickly move to a standard decompression chamber, sometimes located on an adjacent barge, where they are repressurized for subsequent slow decompression. In compressed-air work, this process is known as “decanting” and was fairly common in England and elsewhere, but is prohibited in the United States. The object is to return workers to pressure within five minutes, before bubbles can grow sufficiently in size to cause symptoms. However, this is inherently dangerous because of the difficulties of moving a large gang of workers from one chamber to another. If one worker has trouble clearing his ears during repressurization, the whole shift is placed in jeopardy. There is a much safer procedure, called “surface decompression”, for divers, where only one or two are decompressed at the same time. Despite every precaution on the Auckland Harbour Bridge project, as many as eight minutes occasionally elapsed before bridge workers could be put back under pressure.
Compressed air tunnelling
Tunnels are becoming increasingly important as the population grows, both for the purposes of sewage disposal and for unobstructed traffic arteries and rail service beneath large urban centres. Often, these tunnels must be driven through soft ground considerably below the local water table. Under rivers and lakes, there may be no other way to ensure the safety of the workers than to put compressed air on the tunnel. This technique, using a hydraulically driven shield at the face with compressed air to hold back the water, is known as the plenum process. Under large buildings in a crowded city, compressed air may be necessary to prevent surface subsidence. When this occurs, large buildings can develop cracks in their foundations, sidewalks and streets may drop and pipes and other utilities can be damaged.
To apply pressure to a tunnel, bulkheads are erected across the tunnel to provide the pressure boundary. On smaller tunnels, less than three metres in diameter, a single or combination lock is used to provide access for workers and materials and removal of the excavated ground. Removable track sections are provided by the doors so that they may be operated without interference from the muck-train rails. Numerous penetrations are provided in these bulkheads for the passage of high-pressure air for the tools, low-pressure air for pressurizing the tunnel, fire mains, pressure gauge lines, communications lines, electrical power lines for lighting and machinery and suction lines for ventilation and removal of water in the invert. These are often termed blow lines or “mop lines”. The low-pressure air supply pipe, which is 15-35 cm in diameter, depending on the size of the tunnel, should extend to the working face in order to ensure good ventilation for the workers. A second low-pressure air pipe of equal size should also extend through both bulkheads, terminating just inside the inner bulkhead, to provide air in the event of rupture or break in the primary air supply. These pipes should be fitted with flapper valves which will close automatically to prevent depressurization of the tunnel if the supply pipe is broken. The volume of air required to efficiently ventilate the tunnel and keep CO2 levels low will vary greatly depending on the porosity of the ground and how close the finished concrete lining has been brought to the shield. Sometimes micro-organisms in the soil produce large amounts of CO2. Obviously, under such conditions, more air will be required. Another useful property of compressed air is that it tends to force explosive gases such as methane away from the walls and out of the tunnel. This holds true when mining areas where spilled solvents such as petrol or degreasers have saturated the ground.
A rule of thumb developed by Richardson and Mayo (1960) is that the volume of air required usually can be calculated by multiplying the area of the working face in square metres by six and adding six cubic metres per man. This gives the number of cubic metres of free air required per minute. If this figure is used, it will cover most practical contingencies.
The fire main must also extend through to the face and be provided with hose connections every sixty metres for use in case of fire. Thirty metres of rotproof hose should be attached to the water-filled fire main outlets.
In very large tunnels, over about four metres in diameter, two locks should be provided, one termed the muck lock, for passing muck trains, and the man lock, usually positioned above the muck lock, for the workers. On large projects, the man lock is often made of three compartments so that engineers, electricians and others can lock in and out past a work shift undergoing decompression. These large man locks are usually built external to the main concrete bulkhead so they do not have to resist the external compressive force of the tunnel pressure when open to the outside air.
On very large subaqueous tunnels a safety screen is erected, spanning the upper half of the tunnel, to afford some protection should the tunnel suddenly flood secondary to a blow-out while tunnelling under a river or lake. The safety screen is usually placed as close as practicable to the face, avoiding the excavating machinery. A flying gangway or hanging walkway is used between the screen and the locks, the gangway dropping down to pass at least a metre below the lower edge of the screen. This will allow the workers egress to the man lock in the event of sudden flooding. The safety screen can also be used to trap light gases which may be explosive and a mop line can be attached through the screen and coupled to a suction or blow line. With the valve cracked, this will help to purge any light gases from the working environment. Because the safety screen extends nearly down to the centre of the tunnel, the smallest tunnel it can be employed on is about 3.6 m. It should be noted that workers must be warned to keep clear of the open end of the mop line, as serious accidents can be caused if clothing is sucked into the pipe.
Table 1 is a list of instructions which should be given to compressed-air workers before they first enter the compressed-air environment.
It is the responsibility of the retained physician or occupational health professional for the tunnel project to ensure that air purity standards are maintained and that all safety measures are in effect. Adherence to established decompression schedules by periodically examining the pressure recording graphs from the tunnel and man locks must also be carefully monitored.
Table 1. Instructions for compressed-air workers
- Never “short” yourself on the decompression times prescribed by your employer and the official decompression code in use. The time saved is not worth the risk of decompression illness (DCI), a potentially fatal or crippling disease.
- Do not sit in a cramped position during decompression. To do so allows nitrogen bubbles to gather and concentrate in the joints, thereby contributing to the risk of DCI. Because you are still eliminating nitrogen from your body after you go home, you should refrain from sleeping or resting in a cramped position after work, as well.
- Warm water should be used for showers and baths up to six hours after decompressing; very hot water can actually bring on or aggravate a case of decompression illness.
- Severe fatigue, lack of sleep and heavy drinking the night before can also help bring on decompression illness. Drinking alcohol and taking aspirin should never be used as a “treatment” for pains of decompression illness.
- Fever and illness, such as bad colds, increase the risk of decompression illness. Strains and sprains in muscles and joints are also “favourite” places for DCI to begin.
- When stricken by decompression illness away from the job site, immediately contact the company’s physician or one knowledgeable in treating this disease. Wear your identifying bracelet or badge at all times.
- Leave smoking materials in the changing shack. Hydraulic oil is flammable and should a fire start in the closed environment of the tunnel, it could cause extensive damage and a shutdown of the job, which would lay you off work. Also, because the air is thicker in the tunnel due to compression, heat is conducted down cigarettes so that they become too hot to hold as they get shorter.
- Do not bring thermos bottles in your lunch box unless you loosen the stopper during compression; if you do not do this, the stopper will be forced deep into the thermos bottle. During decompression, the stopper must also be loosened so that the bottle does not explode. Very fragile glass thermos bottles might implode when pressure is applied, even if the stopper is loose.
- When the air lock door has been closed and pressure is applied, you will notice that the air in the air lock gets warm. This is called the “heat of compression” and is normal. Once the pressure stops changing, the heat will dissipate and the temperature will return to normal. During compression, the first thing you will notice is a fullness of your ears. Unless you “clear your ears” by swallowing, yawning, or holding your nose and trying to “blow the air out through your ears”, you will experience ear pain during compression. If you cannot clear your ears, notify the shift foreman immediately so that compression can be halted. Otherwise you may break your eardrums or develop a severe ear squeeze. Once you have reached maximum pressure, there will be no further problems with your ears for the remainder of the shift.
- Should you experience buzzing in your ears, ringing in your ears, or deafness following compression which persists for more than a few hours, you must report to the compressed-air physician for evaluation. Under extremely severe but rare conditions, a portion of the middle ear structure other than the eardrum may be affected if you have had a great deal of difficulty clearing your ears and in that case this must be surgically corrected within two or three days to avoid permanent difficulty.
- If you have a cold or an attack of hay fever, it is best not to try compressing in the air lock until you are over it. Colds tend to make it difficult or impossible for you to equalize your ears or sinuses.
Hyperbaric chamber workers
Hyperbaric oxygen therapy is becoming more common in all areas of the world, with some 2,100 hyperbaric chamber facilities now functioning. Many of these chambers are multiplace units, which are compressed with compressed air to pressures ranging from 1 to 5 kg/cm2 gauge. Patients are given 100% oxygen to breathe, at pressures up to 2 kg/cm2 gauge. At pressures greater than that they may breathe mixed gas for treatment of decompression illness. The chamber attendants, however, typically breathe compressed air and so their exposure in the chamber is similar to that experienced by a diver or compressed-air worker.
Typically the chamber attendant working inside a multiplace chamber is a nurse, respiratory therapist, former diver, or hyperbaric technician. The physical requirements for such workers are similar to those for caisson workers. It is important to remember, however, that a number of chamber attendants working in the hyperbaric field are female. Women are no more likely to suffer ill effects from compressed-air work than men, with the exception of the question of pregnancy. Nitrogen is carried across the placenta when a pregnant woman is exposed to compressed air and this is transferred to the foetus. Whenever decompression takes place, nitrogen bubbles form in the venous system. These are silent bubbles and, when small, do no harm, as they are removed efficiently by the pulmonary filter. The wisdom, however, of having these bubbles appear in a developing foetus is doubtful. What studies have been done indicate that foetal damage may occur under such circumstances. One survey suggested that birth defects are more common in the children of women who have engaged in scuba diving while pregnant. Exposure of pregnant women to hyperbaric chamber conditions should be avoided and appropriate policies consistent with both medical and legal considerations must be developed. For this reason, female workers should be precautioned about the risks during pregnancy and appropriate personnel job assignment and health education programmes should be instituted in order that pregnant women not be exposed to hyperbaric chamber conditions.
It should be pointed out, however, that patients who are pregnant may be treated in the hyperbaric chamber, as they breathe 100% oxygen and are therefore not subject to nitrogen embolization. Previous concerns that the foetus would be at increased risk for retrolental fibroplasia or retinopathy of the newborn have proven to be unfounded in large clinical trials. Another condition, premature closure of the patent ductus arteriosus, has also not been found to be related to the exposure.
Other Hazards
Physical injuries
Divers
In general, divers are prone to the same types of physical injury that any worker is liable to sustain when working in heavy construction. Breaking cables, failing loads, crush injuries from machines, turning cranes and so on, can be commonplace. However, in the underwater environment, the diver is prone to certain types of unique injury that are not found elsewhere.
Suction/entrapment injury is something especially to be guarded against. Working in or near an opening in a ship’s hull, a caisson which has a lower water level on the side opposite the diver, or a dam can be causative of this type of mishap. Divers often refer to this type of situation as being trapped by “heavy water”.
To avoid dangerous situations where the diver’s arm, leg, or whole body may be sucked into an opening such as a tunnel or pipe, strict precautions must be taken to tag out pipe valves and flood gates on dams so that they cannot be opened while the diver is in the water near them. The same is true of pumps and piping within ships that the diver is working on.
Injury can include oedema and hypoxia of an entrapped limb sufficient to cause muscle necrosis, permanent nerve damage, or even loss of the entire limb, or it may occasion gross crushing of a portion of the body or the whole body so as to cause death from simple massive trauma. Entrapment in cold water for a long period of time may cause the diver to die of exposure. If the diver is using scuba gear, he may run out of air and drown before his release can be effected, unless additional scuba tanks can be provided.
Propeller injuries are straightforward and must be guarded against by tagging out a ship’s main propulsion machinery while the diver is in the water. It must be remembered, however, that steam turbine-powered ships, when in port, are continuously turning over their screws very slowly, using their jacking gear to avoid cooling and distortion of the turbine blades. Thus the diver, when working on such a blade (trying to clear it from entangled cables, for example), must be aware that the turning blade must be avoided as it approaches a narrow spot close to the hull.
Whole-body squeeze is a unique injury which can occur to deep sea divers using the classical copper helmet mated to the flexible rubberized suit. If there is no check valve or non-return valve where the air pipe connects to the helmet, cutting the air line at the surface will cause an immediate relative vacuum within the helmet, which can draw the entire body into the helmet. The effects of this can be instant and devastating. For example, at a depth of 10 m, about 12 tons of force is exerted on the soft part of the diver’s dress. This force will drive his body into the helmet if pressurization of the helmet is lost. A similar effect may be produced if the diver fails unexpectedly and fails to turn on compensating air. This can produce severe injury or death if it occurs near the surface, as a 10-metre fall from the surface will halve the volume of the dress. A similar fall occurring between 40 and 50 m will change the suit volume only about 17%. These volume changes are in accordance with Boyle’s Law.
Caisson and tunnel workers
Tunnel workers are subject to the usual types of accidents seen in heavy construction, with the additional problem of a higher incidence of falls and injuries from cave-ins. It must be stressed that an injured compressed-air worker who may have broken ribs should be suspected of having a pneumothorax until proven otherwise and therefore great care must be taken in decompressing such a patient. If a pneumothorax is present, it must be relieved at pressure in the working chamber before decompression is attempted.
Noise
Noise damage to compressed-air workers may be severe, as air motors, pneumatic hammers and drills are never properly equipped with silencers. Noise levels in caissons and tunnels have been measured at over 125 dB. These levels are physically painful, as well as causative of permanent damage to the inner ear. Echo within the confines of a tunnel or caisson exacerbates the problem.
Many compressed-air workers balk at wearing ear protection, saying that blocking the sound of an approaching muck train would be dangerous. There is little foundation for this belief, as hearing protection at best only attenuates sound but does not eliminate it. Furthermore, not only is a moving muck train not “silent” to a protected worker, but it also gives other cues such as moving shadows and vibration in the ground. A real concern is complete hermetic occlusion of the auditory meatus provided by a tightly fitting ear muff or protector. If air is not admitted to the external auditory canal during compression, external ear squeeze may result as the ear drum is forced outward by air entering the middle ear via the Eustachian tube. The usual sound protective ear muff is usually not completely air tight, however. During compression, which lasts only a tiny fraction of the total shift time, the muff can be slightly loosened should pressure equalization prove a problem. Formed fibre ear plugs which can be moulded to fit in the external canal provide some protection and are not air tight.
The goal is to avoid a time weighted average noise level of higher than 85 dBA. All compressed-air workers should have pre-employment base line audiograms so that auditory losses which may result from the high-noise environment can be monitored.
Hyperbaric chambers and decompression locks can be equipped with efficient silencers on the air supply pipe entering the chamber. It is important that this be insisted on, as otherwise the workers will be considerably bothered by the ventilation noise and may neglect to ventilate the chamber adequately. A continuous vent can be maintained with a silenced air supply producing no more than 75dB, about the noise level in an average office.
Fire
Fire is always of great concern in compressed-air tunnel work and in clinical hyperbaric chamber operations. One can be lulled into a false sense of security when working in a steel-walled caisson which has a steel roof and a floor consisting only of unburnable wet muck. However, even in these circumstances, an electrical fire can burn insulation, which will prove highly toxic and can kill or incapacitate a work crew very quickly. In tunnels which are driven using wooden lagging before the concrete is poured, the danger is even greater. In some tunnels, hydraulic oil and straw used for caulking can furnish additional fuel.
Fire under hyperbaric conditions is always more intense because there is more oxygen available to support combustion. A rise from 21% to 28% in the oxygen percentage will double the burning rate. As the pressure is increased, the amount of oxygen available to burn increases The increase is equal to the percentage of oxygen available multiplied by the number of atmospheres in absolute terms. For example, at a pressure of 4 ATA (equal to 30 m of sea water), the effective oxygen percentage would be 84% in compressed-air. However, it must be remembered that even though burning is very much accelerated under such conditions, it is not the same as the speed of burning in 84% oxygen at one atmosphere. The reason for this is that the nitrogen present in the atmosphere has a certain quenching effect. Acetylene cannot be used at pressures over one bar because of its explosive properties. However, other torch gases and oxygen can be used for cutting steel. This has been done safely at pressures up to 3 bar. Under such circumstances, however, scrupulous care must be exercised and someone must stand by with a fire hose to immediately quench any fire which might start, should an errant spark come in contact with something combustible.
Fire requires three components to be present: fuel, oxygen and an ignition source. If any one of these three factors is absent, fire will not occur. Under hyperbaric conditions, it is almost impossible to remove oxygen unless the piece of equipment in question can be inserted into the environment by filling it or surrounding it with nitrogen. If fuel cannot be removed, an ignition source must be avoided. In clinical hyperbaric work, meticulous care is taken to prevent the oxygen percentage in the multiplace chamber from rising above 23%. In addition, all electrical equipment within the chamber must be intrinsically safe, with no possibility of producing an arc. Personnel in the chamber should wear cotton clothing which has been treated with flame retardant. A water-deluge system must be in place, as well as a hand-held fire hose independently actuated. If a fire occurs in a multiplace clinical hyperbaric chamber, there is no immediate escape and so the fire must be fought with a hand-held hose and with the deluge system.
In monoplace chambers pressurized with 100% oxygen, a fire will be instantly fatal to any occupant. The human body itself supports combustion in 100% oxygen, especially at pressure. For this reason, plain cotton clothing is worn by the patient in the monoplace chamber to avoid static sparks which could be produced by synthetic materials. There is no need to fireproof this clothing, however, as if a fire should occur, the clothing would afford no protection. The only method for avoiding fires in the monoplace oxygen-filled chamber is to completely avoid any source of ignition.
When dealing with high pressure oxygen, at pressures over 10 kg/cm2 gauge, adiabatic heating must be recognized as a possible source of ignition. If oxygen at a pressure of 150 kg/cm2 is suddenly admitted to a manifold via a quick-opening ball valve, the oxygen may “diesel” if even a tiny amount of dirt is present. This can produce a violent explosion. Such accidents have occurred and for this reason, quick-opening ball valves should never be used in high pressure oxygen systems.
Decompression Disorders
A wide range of workers are subject to decompression (a reduction in ambient pressure) as part of their working routine. These include divers who themselves are drawn from a wide range of occupations, caisson workers, tunnellers, hyperbaric chamber workers (usually nurses), aviators and astronauts. Decompression of these individuals can and does precipitate a variety of decompression disorders. While most of the disorders are well understood, others are not and in some instances, and despite treatment, injured workers can become disabled. The decompression disorders are the subject of active research.
Mechanism of Decompression Injury
Principles of gas uptake and release
Decompression may injure the hyperbaric worker via one of two primary mechanisms. The first is the consequence of inert gas uptake during the hyperbaric exposure and bubble formation in tissues during and after the subsequent decompression. It is generally assumed that the metabolic gases, oxygen and carbon dioxide, do not contribute to bubble formation. This is almost certainly a false assumption, but the consequent error is small and such an assumption will be made here.
During the compression (increase in ambient pressure) of the worker and throughout their time under pressure, inspired and arterial inert gas tensions will be increased relative to those experienced at normal atmospheric pressure—the inert gas(es) will then be taken up into tissues until an equilibrium of inspired, arterial and tissue inert gas tensions is established. Equilibrium times will vary from less than 30 minutes to more than a day depending upon the type of tissue and gas involved, and, in particular, will vary according to:
- the blood supply to the tissue
- the solubility of the inert gas in blood and in the tissue
- the diffusion of the inert gas through blood and into the tissue
- the temperature of the tissue
- the local tissue work-loads
- the local tissue carbon dioxide tension.
The subsequent decompression of the hyperbaric worker to normal atmospheric pressure will clearly reverse this process, gas will be released from tissues and will eventually be expired. The rate of this release is determined by the factors listed above, except, for as yet poorly understood reasons, it appears to be slower than the uptake. Gas elimination will be slower still if bubbles form. The factors that influence the formation of bubbles are well established qualitatively, but not quantitatively. For a bubble to form the bubble energy must be sufficient to overcome ambient pressure, surface tension pressure and elastic tissue pressures. The disparity between theoretical predictions (of surface tension and critical bubble volumes for bubble growth) and actual observation of bubble formation is explained variously by arguing that bubbles form in tissue (blood vessel) surface defects and/or on the basis of small short-lived bubbles (nuclei) that are continually formed in the body (e.g., between tissue planes or in areas of cavitation). The conditions that must exist before gas comes out of solution are also poorly defined—although it is likely that bubbles form whenever tissue gas tensions exceed ambient pressure. Once formed, bubbles provoke injury (see below) and become increasingly stable as a consequence of coalescence and recruitment of surfactants to the bubble surface. It may be possible for bubbles to form without decompression by changing the inert gas that the hyperbaric worker is breathing. This effect is probably small and those workers that have had a sudden onset of a decompression illness after a change in inspired inert gas almost certainly already had “stable” bubbles in their tissues.
It follows that to introduce a safe working practice a decompression programme (schedule) should be employed to avoid bubble formation. This will require modelling of the following:
- the uptake of the inert gas(es) during the compression and the hyperbaric exposure
- the elimination of the inert gas(es) during and after the decompression
- the conditions for bubble formation.
It is reasonable to state that to date no completely satisfactory model of decompression kinetics and dynamics has been produced and that hyperbaric workers now rely on programmes that have been established essentially by trial and error.
Effect of Boyle’s Law on barotrauma
The second primary mechanism by which decompression can cause injury is the process of barotrauma. The barotraumata can arise from compression or decompression. In compression barotrauma, the air spaces in the body that are surrounded by soft tissue, and hence are subject to increasing ambient pressure (Pascal’s principle), will be reduced in volume (as reasonably predicted by Boyles’ law: doubling of ambient pressure will cause gas volumes to be halved). The compressed gas is displaced by fluid in a predictable sequence:
- The elastic tissues move (tympanic membrane, round and oval windows, mask material, clothing, rib cage, diaphragm).
- Blood is pooled in the high compliance vessels (essentially veins).
- Once the limits of compliance of blood vessels are reached, there is an extravasation of fluid (oedema) and then blood (haemorrhage) into the surrounding soft tissues.
- Once the limits of compliance of the surrounding soft tissues are reached, there is a shift of fluid and then blood into the air space itself.
This sequence can be interrupted at any time by an ingress of additional gas into the space (e.g., into the middle ear on performing a valsalva manoeuvre) and will stop when gas volume and tissue pressure are in equilibrium.
The process is reversed during decompression and gas volumes will increase, and if not vented to atmosphere will cause local trauma. In the lung this trauma may arise from either over-distension or from shearing between adjacent areas of lung that have significantly different compliance and hence expand at different rates.
Pathogenesis of Decompression Disorders
The decompression illnesses can be divided into the barotraumata, tissue bubble and intravascular bubble categories.
Barotraumata
During compression, any gas space may become involved in barotrauma and this is especially common in the ears. While damage to the external ear requires occlusion of the external ear canal (by plugs, a hood, or impacted wax), the tympanic membrane and middle ear is frequently damaged. This injury is more likely if the worker has upper respiratory tract pathology that causes eustachian tube dysfunction. The possible consequences are middle ear congestion (as described above) and/or tympanic membrane rupture. Ear pain and a conductive deafness are likely. Vertigo may result from an ingress of cold water into the middle ear through a ruptured tympanic membrane. Such vertigo is transient. More commonly, vertigo (and possibly also a sensorineural deafness) will result from inner ear barotrauma. During compression, inner ear damage often results from a forceful valsalva manoeuvre (that will cause a fluid wave to be transmitted to the inner ear via the cochlea duct). The inner ear damage is usually within the inner ear—round and oval window rupture is less common.
The paranasal sinuses often are similarly involved and usually because of a blocked ostium. In addition to local and referred pain, epistaxis is common and cranial nerves may be “compressed”. It is noteworthy that the facial nerve may be likewise affected by middle ear barotrauma in individuals with a perforate auditory nerve canal. Other areas that may be affected by compressive barotrauma, but less commonly, are the lungs, teeth, gut, diving mask, dry-suits and other equipment such as buoyancy compensating devices.
Decompressive barotraumata are less common than compressive barotraumata, but tend to have a more adverse outcome. The two areas primarily affected are the lungs and inner ear. The typical pathological lesion of pulmonary barotrauma has yet to be described. The mechanism has been variously ascribed to the over-inflation of alveoli either to “open up pores” or mechanically to disrupt the alveolus, or as the consequence of shearing of lung tissue due to local differential lung expansion. Maximum stress is likely at the base of alveoli and, given that many underwater workers often breathe with small tidal excursions at or near total lung capacity, the risk of barotrauma is increased in this group as lung compliance is lowest at these volumes. Gas release from damaged lung may track through the interstitium to the hilum of the lungs, mediastinum and perhaps into the subcutaneous tissues of the head and neck. This interstitial gas may cause dyspnoea, substernal pain and coughing which may be productive of a little bloodstained sputum. Gas in the head and neck is self-evident and may occasionally impair phonation. Cardiac compression is extremely rare. Gas from a barotraumatised lung may also escape into the pleural space (to cause a pneumothorax) or into the pulmonary veins (to eventually become arterial gas emboli). In general, such gas most commonly either escapes into the interstitium and pleural space or into the pulmonary veins. Concurrent obvious damage to the lung and arterial gas embolism are (fortunately) uncommon.
Autochthonous tissue bubbles
If, during decompression, a gas phase forms, this is usually, initially, in tissues. These tissue bubbles may induce tissue dysfunction via a variety of mechanisms—some of these are mechanical and others are biochemical.
In poorly compliant tissues, such as long bones, the spinal cord and tendons, bubbles may compress arteries, veins, lymphatics and sensory cells. Elsewhere, tissue bubbles may cause mechanical disruption of cells or, at a microscopic level, of myelin sheaths. The solubility of nitrogen in myelin may explain the frequent involvement of the nervous system in decompression illness amongst workers who have been breathing either air or an oxygen-nitrogen gas mixture. Bubbles in tissues may also induce a biochemical “foreign-body” response. This provokes an inflammatory response and may explain the observation that a common presentation of decompression illness is an influenza-like illness. The significance of the inflammatory response is demonstrated in animals such as rabbits, where inhibition of the response prevents the onset of decompression illness. The major features of the inflammatory response include a coagulopathy (this is particularly important in animals, but less so in humans) and the release of kinins. These chemicals cause pain and also an extravasation of fluid. Haemoconcentration also results from the direct effect of bubbles on blood vessels. The end result is a significant compromise of the microcirculation and, in general, measurement of the haematocrit correlates well with the severity of the illness. Correction of this haemoconcentration has a predictably significant benefit on outcome.
Intravascular bubbles
Venous bubbles may either form de-novo as gas comes out of solution or they may be released from tissues. These venous bubbles travel with blood flow to the lungs to be trapped in the pulmonary vasculature. The pulmonary circulation is a highly effective filter of bubbles because of the relatively low pulmonary artery pressure. In contrast, few bubbles are trapped for long periods in the systemic circulation because of the significantly greater systemic arterial pressure. The gas in bubbles trapped in the lung diffuses into the pulmonary air spaces from where it is exhaled. While these bubbles are trapped, however, they may cause adverse effects by either provoking an imbalance of lung perfusion and ventilation or by increasing pulmonary artery pressure and consequently right heart and central venous pressure. The increased right heart pressure can cause “right to left” shunting of blood through pulmonary shunts or intra-cardiac “anatomical defects” such that bubbles bypass the lung “filter” to become arterial gas emboli. Increases in venous pressure will impair venous return from tissues, thereby impairing the clearance of inert gas from the spinal cord; venous haemorrhagic infarction may result. Venous bubbles also react with blood vessels and blood constituents. An effect on blood vessels is to strip the surfactant lining from endothelial cells and hence to increase vascular permeability, which may be further compromised by the physical dislocation of endothelial cells. However, even in the absence of such damage, endothelial cells increase the concentration of glycoprotein receptors for polymorphonuclear leukocytes on their cell surface. This, together with a direct stimulation of white blood cells by bubbles, causes leucocyte binding to endothelial cells (reducing flow) and subsequent infiltration into and through the blood vessels (diapedesis). The infiltrating polymorphonuclear leukocytes cause future tissue injury by release of cytotoxins, oxygen free radicals and phospholipases. In blood, bubbles will not only cause the activation and accumulation of polymorphonuclear leukocytes, but also the activation of platelets, coagulation and complement, and the formation of fat emboli. While these effects have relatively minor importance in the highly compliant venous circulation, similar effects in the arteries can reduce blood flow to ischaemic levels.
Arterial bubbles (gas emboli) can arise from:
- pulmonary barotrauma causing the release of bubbles into the pulmonary veins
- bubbles being “forced” through the pulmonary arterioles (this process is enhanced by oxygen toxicity and by those bronchodilators that are also vasodilators such as aminophylline)
- bubbles bypassing the lung filter through a right to left vascular channel (e.g., patent foramen ovale).
Once in the pulmonary veins, bubbles return to the left atrium, left ventricle, and then are pumped into the aorta. Bubbles in the arterial circulation will distribute according to buoyancy and blood flow in large vessels, but elsewhere with blood flow alone. This explains the predominant embolism of the brain and, in particular, the middle cerebral artery. The majority of bubbles that enter the arterial circulation will pass through into the systemic capillaries and into the veins to return to the right side of the heart (usually to be trapped in the lungs). During this transit these bubbles may cause a temporary interruption of function. If the bubbles remain trapped in the systemic circulation or are not redistributed within five to ten minutes, then this loss of function may persist. If bubbles embolise the brain stem circulation, then the event may be lethal. Fortunately, the majority of bubbles will be redistributed within minutes of first arrival in the brain and a recovery of function is usual. However, during this transit the bubbles will cause the same vascular (blood vessels and blood) reactions as described above in venous blood and veins. Consequently, a significant and progressive decline in cerebral blood flow may occur, which may reach the levels at which normal function cannot be sustained. The hyperbaric worker will, at this time, suffer a relapse or deterioration in function. In general, about two-thirds of hyperbaric workers who suffer cerebral arterial gas embolism will spontaneously recover and about one-third of these will subsequently relapse.
Clinical Presentation of Decompression Disorders
Time of onset
Occasionally, the onset of decompression illness is during the decompression. This is most commonly seen in the barotraumata of ascent, particularly involving the lungs. However, the onset of the majority of decompression illnesses occurs after decompression is complete. Decompression illnesses due to the formation of bubbles in tissues and in blood vessels usually become evident within minutes or hours after decompression. The natural history of many of these decompression illnesses is for the spontaneous resolution of symptoms. However, some will only resolve spontaneously incompletely and there is a need for treatment. There is substantial evidence that the earlier the treatment the better the outcome. The natural history of treated decompression illnesses is variable. In some cases, residual problems are seen to resolve over the following 6-12 months, while in others symptoms appear not to resolve.
Clinical manifestations
A common presentation of decompression illness is an influenza-like condition. Other frequent complaints are various sensory disorders, local pain, particularly in the limbs; and other neurologic manifestations, which may involve higher functions, special senses and motor weariness (less commonly the skin and lymphatic systems may be involved). In some groups of hyperbaric workers, the most common presentation of decompression illness is pain. This may be a discrete pain about a specific joint or joints, back pain or referred pain (when the pain is often located in the same limb as are overt neurologic deficits), or less commonly, in an acute decompression illness, vague migratory aches and pains may be noticed. Indeed, it is reasonable to state that the manifestations of the decompression illnesses are protean. Any illness in a hyperbaric worker that occurs up to 24-48 hours after a decompression should be assumed to be related to that decompression until proven otherwise.
Classification
Until recently, the decompression illnesses were classified into:
- the barotraumata
- cerebral arterial gas embolism
- decompression sickness.
Decompression sickness was further subdivided into Type 1 (pain, itch, swelling and skin rashes), Type 2 (all other manifestations) and Type 3 (manifestations of both cerebral arterial gas embolism and decompression sickness) categories. This classification system arose from an analysis of the outcome of caisson workers using new decompression schedules. However, this system has had to be replaced both because it is neither discriminatory nor prognostic and because there is a low concordance in diagnosis between experienced physicians. The new classification of the decompression illnesses recognises the difficulty in distinguishing between cerebral arterial gas embolism and cerebral decompression sickness and similarly the difficulty in distinguishing Type 1 from Type 2 and Type 3 decompression sickness. All decompression illnesses are now classified as such—decompression illness, as described in table 1. This term is prefaced with a description of the nature of the illness, the progression of symptoms and a list of the organ systems in which the symptoms are manifest (no assumptions are made about the underlying pathology). For example, a diver may have acute progressive neurological decompression illness. The complete classification of the decompression illness includes a comment on the presence or absence of barotrauma and the likely inert gas loading. These latter terms are relevant to both treatment and likely fitness to return to work.
Table 1. Revised classification system of the decompression illnesses
|
Duration |
Evolution |
Symptoms |
|
|
Acute |
Progressive |
Musculoskeletal |
|
|
Chronic |
Spontaneously resolving |
Cutaneous |
Decompression illness + or - |
|
|
Static |
Lymphatic |
Evidence of barotrauma |
|
|
Relapsing |
Neurological |
|
|
|
|
Vestibular |
|
|
|
|
Cardiorespiratory |
|
First Aid Management
Rescue and resuscitation
Some hyperbaric workers develop a decompression illness and require to be rescued. This is particularly true for divers. This rescue may require their recovery to a stage or diving bell, or a rescue from underwater. Specific rescue techniques must be established and practised if they are to be successful. In general, divers should be rescued from the ocean in a horizontal posture (to avoid possibly lethal falls in cardiac output as the diver is re-subjected to gravity—during any dive there is a progressive loss of blood volume consequent to displacement of blood from the peripheries into the chest) and consequent diuresis and this posture should be maintained until the diver is, if necessary, in a recompression chamber.
The resuscitation of an injured diver should follow the same regimen as used in resuscitations elsewhere. Of specific note is that the resuscitation of a hypothermic individual should continue at least until the individual is rewarmed. There is no convincing evidence that resuscitation of an injured diver in the water is effective. In general, the divers’ best interests are usually served by early rescue ashore, or to a diving bell/platform.
Oxygen and fluid resuscitation
A hyperbaric worker with a decompression illness should be laid flat, to minimize the chances of bubbles distributing to the brain, but not placed in a head-down posture which probably adversely affects the outcome. The diver should be given 100% oxygen to breathe; this will require either a demand valve in a conscious diver or a sealing mask, high flow rates of oxygen and a reservoir system. If oxygen administration is to be prolonged, then airbreaks should be given to ameliorate or retard the development of pulmonary oxygen toxicity. Any diver with decompression illness should be re-hydrated. There is probably no place for oral fluids in the acute resuscitation of a severely injured worker. In general, it is difficult to administer oral fluids to someone lying flat. Oral fluids will require the administration of oxygen to be interrupted and then usually have negligible immediate effect on the blood volume. Finally, since subsequent hyperbaric oxygen treatment may cause a convulsion, it is not desirable to have any stomach contents. Ideally then, fluid resuscitation should be by the intravenous route. There is no evidence of any advantage of colloid over crystalloid solutions and the fluid of choice is probably normal saline. Solutions containing lactate should not be given to a cold diver and dextrose solutions should not be given to anyone with a brain injury (as aggravation of the injury is possible). It is essential that an accurate fluid balance be maintained as this is probably the best guide to the successful resuscitation of a hyperbaric worker with decompression illness. Bladder involvement is sufficiently common that early recourse to bladder catheterization is warranted in the absence of urinary output.
There are no drugs that are of proven benefit in the treatment of the decompression illnesses. However, there is growing support for lignocaine and this is under clinical trial. The role of lignocaine is thought to be both as a membrane stabiliser and as an inhibitor of the polymorphonuclear leukocyte accumulation and blood vessel adherence that is provoked by bubbles. It is noteworthy that one of the probable roles of hyperbaric oxygen is also to inhibit the accumulation of and adherence to blood vessels of leucocytes. Finally, there is no evidence that any benefit is derived from the use of platelet inhibitors such as aspirin or other anticoagulants. Indeed, as haemorrhage into the central nervous system is associated with severe neurological decompression illness, such medication may be contra-indicated.
Retrieval
Retrieval of a hyperbaric worker with decompression illness to a therapeutic recompression facility should occur as soon as is possible, but must not involve any further decompression. The maximum altitude to which such a worker should be decompressed during aeromedical evacuation is 300 m above sea level. During this retrieval, the first aid and adjuvant care described above should be provided.
Recompression Treatment
Applications
The definitive treatment of most of the decompression illnesses is recompression in a chamber. The exception to this statement are the barotraumata that do not cause arterial gas embolism. The majority of aural barotrauma victims require serial audiology, nasal decongestants, analgesics and, if inner ear barotrauma is suspected, strict bed rest. It is possible however that hyperbaric oxygen (plus stellate ganglion blockade) may be an effective treatment of this latter group of patients. The other barotraumata that often require treatment are those of the lung—most of those respond well to 100% oxygen at atmospheric pressure. Occasionally, chest cannulation may be needed for a pneumothorax. For other patients, early recompression is indicated.
Mechanisms
An increase in ambient pressure will make bubbles smaller and hence less stable (by increasing surface tension pressure). These smaller bubbles will also have a greater surface area to volume for resolution by diffusion and their mechanical disruptive and compressive effects on tissue will be reduced. It is also possible that there is a threshold bubble volume that will stimulate a “foreign-body” reaction. By reducing bubble size, this effect may be reduced. Finally, reducing the volume (length) of columns of gas that are trapped in the systemic circulation will promote their redistribution to the veins. The other outcome of most recompressions is an increase in the inspired (PiO2) and arterial oxygen tension (PaO2). This will relieve hypoxia, lower interstitial fluid pressure, inhibit the activation and accumulation of polymorphonuclear leukocytes that is usually provoked by bubbles, and lower the haematocrit and hence blood viscosity.
Pressure
The ideal pressure at which to treat decompression illness is not established, although the conventional first choice is 2.8 bar absolute (60 fsw; 282 kPa), with further compression to 4 and 6 bar absolute pressure if the response of symptoms and signs is poor. Experiments in animals suggest that 2 bars absolute pressure is as effective a treatment pressure as greater compressions.
Gas(es)
Similarly, the ideal gas to be breathed during the therapeutic recompression of these injured workers is not established. Oxygen-helium mixtures may be more effective in the shrinkage of air bubbles than either air or 100% oxygen and are the subject of ongoing research. The ideal PiO2 is thought, from in vivo research, to be about 2 bar absolute pressure although it is well established, in head injured patients, that the ideal tension is lower at 1.5 bars absolute. The dose relationship with regard to oxygen and inhibition of bubble-provoked polymorphonuclear leukocyte accumulation has not yet been established.
Adjuvant care
The treatment of an injured hyperbaric worker in a recompression chamber must not be allowed to compromise his/her need for adjuvant care such as ventilation, rehydration and monitoring. To be a definitive treatment facility, a recompression chamber must have a working interface with the equipment routinely used in critical care medical units.
Follow-up treatment and investigations
Persistent and relapsing symptoms and signs of decompression illness are common and most injured workers will require repeated recompressions. These should continue until the injury is and remains corrected or at least until two successive treatments have failed to produce any sustained benefit. The basis of ongoing investigation is careful clinical neurological examination (including mental status), as available imaging or provocative investigative techniques have either an associated excessive false positive rate (EEG, bone radio-isotope scans, SPECT scans) or an associated excessive false negative rate (CT, MRI, PET, evoked response studies). One year after an episode of decompression illness, the worker should be x-rayed to determine if there is any dysbaric osteonecrosis (aseptic necrosis) of their long bones.
Outcome
The outcome after recompression therapy of decompression illness depends entirely upon the group being studied. Most hyperbaric workers (e.g., military and oil-field divers) respond well to treatment and significant residual deficits are uncommon. In contrast, many recreational divers treated for decompression illness have a subsequent poor outcome. The reasons for this difference in outcome are not established. Common sequelae of decompression illness are in order of decreasing frequency: depressed mood; problems in short-term memory; sensory symptoms such as numbness; difficulties with micturition and sexual dysfunction; and vague aches and pains.
Return to hyperbaric work
Fortunately, most hyperbaric workers are able to return to hyperbaric work after an episode of decompression illness. This should be delayed for at least a month (to allow a return to normal of the disordered physiology) and must be discouraged if the worker suffered pulmonary barotrauma or has a history of recurrent or severe inner ear barotrauma. A return to work should also be contingent upon:
- the severity of the decompression illness being commensurate with the extent of the hyperbaric exposure/decompression stress
- a good response to treatment
- no evidence of sequelae.
Ventilatory Acclimatization to High Altitude
People are increasingly working at high altitudes. Mining operations, recreational facilities, modes of transportation, agricultural pursuits and military campaigns are often at high altitude, and all of these require human physical and mental activity. All such activity involves increased requirements for oxygen. A problem is that as one ascends higher and higher above sea level, both the total air pressure (the barometric pressure, PB) and the amount of oxygen in the ambient air (that portion of total pressure due to oxygen, PO2) progressively fall. As a result, the amount of work we can accomplish progressively decreases. These principles affect the workplace. For example, a tunnel in Colorado was found to require 25% more time to complete at an altitude of 11,000 ft than comparable work at sea level, and altitude effects were implicated in the delay. Not only is there increased muscular fatigue, but also, deterioration of mental function. Memory, computation, decision making and judgement all become impaired. Scientists doing calculations at the Mona Loa Observatory at an altitude above 4,000 m on the island of Hawaii have found they require more time to perform their calculations and they make more mistakes than at sea level. Because of the increasing scope, magnitude, variety and distribution of human activities on this planet, more people are working at high altitude, and effects of altitude become an occupational issue.
Fundamentally important to occupational performance at altitude is maintaining the oxygen supply to the tissues. We (and other animals) have defences against low oxygen states (hypoxia). Chief among these is an increase in breathing (ventilation), which begins when the oxygen pressure in the arterial blood (PaO2) decreases (hypoxemia), is present for all altitudes above sea level, is progressive with altitude and is our most effective defence against low oxygen in the environment. The process whereby breathing increases at high altitude is called ventilatory acclimatization. The importance of the process can be seen in figure 1, which shows that the oxygen pressure in the arterial blood is higher in acclimatized subjects than in unacclimatized subjects. Further, the importance of acclimatization in maintaining the arterial oxygen pressure increases progressively with increasing altitude. Indeed, the unacclimatized person is unlikely to survive above an altitude of 20,000 ft, whereas acclimatized persons have been able to climb to the summit of Mount Everest (29,029 ft, 8,848 m) without artificial sources of oxygen.
Figure 1. Ventilatory acclimatization
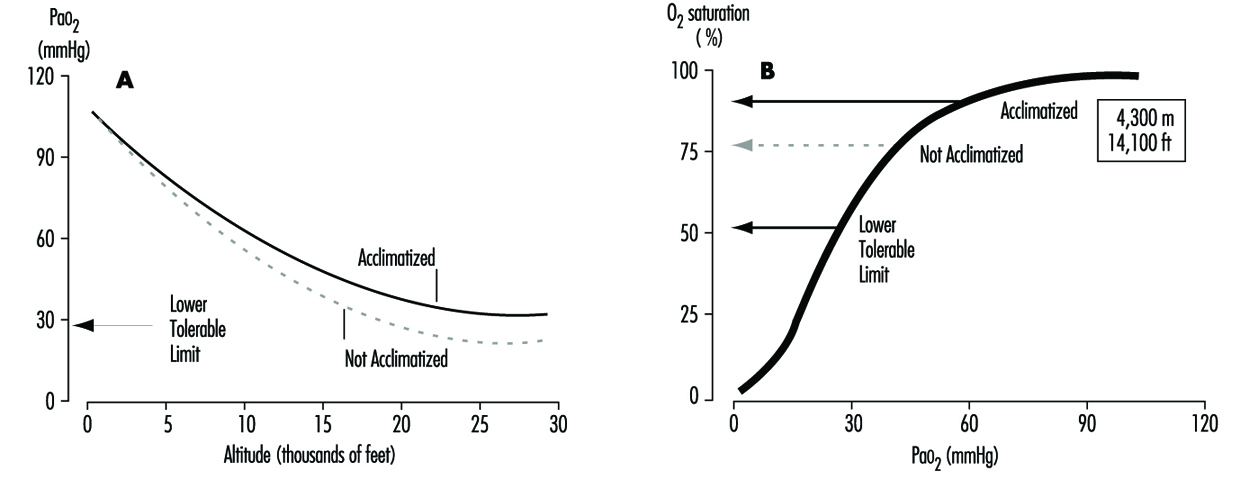
Mechanism
The stimulus for the increase in ventilation at high altitude largely and almost exclusively arises in a tissue which monitors the oxygen pressure in the arterial blood and is contained within an organ called the carotid body, about the size of a pinhead, located at a branch point in each of the two carotid arteries, at the level of the angle of the jaw. When the arterial oxygen pressure falls, nerve-like cells (chemoreceptor cells) in the carotid body sense this decrease and increase their firing rate along the 9th cranial nerve, which carries the impulses directly to the respiratory control centre in the brain stem. When the respiratory centre receives increased numbers of impulses, it stimulates an increase in the frequency and depth of breathing via complex nerve pathways, which activate the diaphragm and the muscles of the chest wall. The result is an increased amount of air ventilated by the lungs, figure 2, which in turn acts to restore the arterial oxygen pressure. If a subject breathes oxygen or air enriched with oxygen, the reverse happens. That is, the chemoreceptor cells decrease their firing rate, which decreases the nerve traffic to the respiratory centre, and breathing decreases. These small organs on each side of the neck are very sensitive to small changes in oxygen pressure in the blood. Also, they are almost entirely responsible for maintaining the body’s oxygen level, for when both of them are damaged or removed, ventilation no longer increases when blood oxygen levels fall. Thus an important factor controlling breathing is the arterial oxygen pressure; a decrease in oxygen level leads to an increase in breathing, and an increase in oxygen level leads to a decrease in breathing. In each case the result is, in effect, the body’s effort to maintain blood oxygen levels constant.
Figure 2. Sequence of events in acclimatization
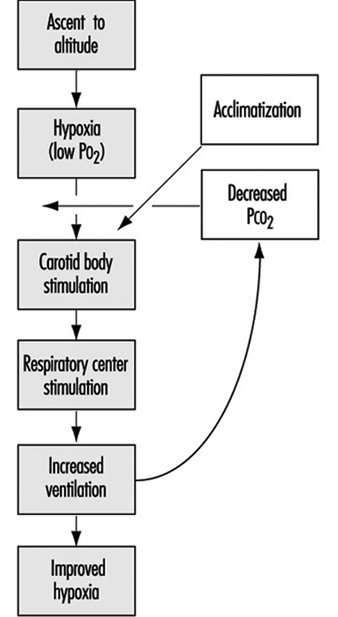
Time course (factors opposing the increase in ventilation at altitude)
Oxygen is required for the sustained production of energy, and when oxygen supply to tissues is reduced (hypoxia), tissue function may become depressed. Of all organs, the brain is most sensitive to lack of oxygen, and, as noted above, centres within the central nervous system are important in the control of breathing. When we breathe a low-oxygen mixture, the initial response is an increase in ventilation, but after 10 minutes or so the increase is blunted to some extent. While the cause for this blunting is not known, its suggested cause is depression of some central neural function related to the ventilation pathway, and has been called hypoxic ventilatory depression. Such depression has been observed shortly after ascent to high altitude. The depression is transient, lasting only a few hours, possibly because there is some tissue adaptation within the central nervous system.
Nevertheless, some increase in ventilation usually begins immediately on going to high altitude, although time is required before maximum ventilation is achieved. On arrival at altitude, increased carotid body activity attempts to increase ventilation, and thereby to raise the arterial oxygen pressure back to the sea level value. However, this presents the body with a dilemma. An increase in breathing causes an increased excretion of carbon dioxide (CO2) in the exhaled air. When CO2 is in body tissues, it creates an acid aqueous solution, and when it is lost in exhaled air, the body fluids, including blood, become more alkaline, thus altering the acid-base balance in the body. The dilemma is that ventilation is regulated not only to keep oxygen pressure constant, but also for acid-base balance. CO2 regulates breathing in the opposite direction from oxygen. Thus when the CO2 pressure (i.e., the degree of acidity somewhere within the respiratory centre) rises, ventilation rises, and when it falls, ventilation falls. On arrival at high altitude, any increase in ventilation caused by the low oxygen environment will lead to a fall in CO2 pressure, which causes alkalosis and acts to oppose the increased ventilation (figure 2). Therefore, the dilemma on arrival is that the body cannot maintain constancy in both oxygen pressure and acid-base balance. Human beings require many hours and even days to regain proper balance.
One method for rebalancing is for the kidneys to increase alkaline bicarbonate excretion in the urine, which compensates for the respiratory loss of acidity, thus helping to restore the body’s acid-base balance toward the sea-level values. The renal excretion of bicarbonate is a relatively slow process. For example, on going from sea level to 4,300 m (14,110 ft), acclimatization requires from seven to ten days (figure 3). This action of the kidneys, which reduces the alkaline inhibition of ventilation, was once thought to be the major reason for the slow increase in ventilation following ascent, but more recent research assigns a dominant role to a progressive increase in the sensitivity of the hypoxic sensing ability of the carotid bodies during the early hours to days following ascent to altitude. This is the interval of ventilatory acclimatization. The acclimatization process allows, in effect, ventilation to rise in response to low arterial oxygen pressure even though the CO2 pressure is falling. As the ventilation rises and CO2 pressure falls with acclimatization at altitude, there is a resultant and concomitant rise in oxygen pressure within the lung alveoli and the arterial blood.
Figure 3. Time course of ventilatory acclimatization for sea level subjects taken to 4,300 m altitude
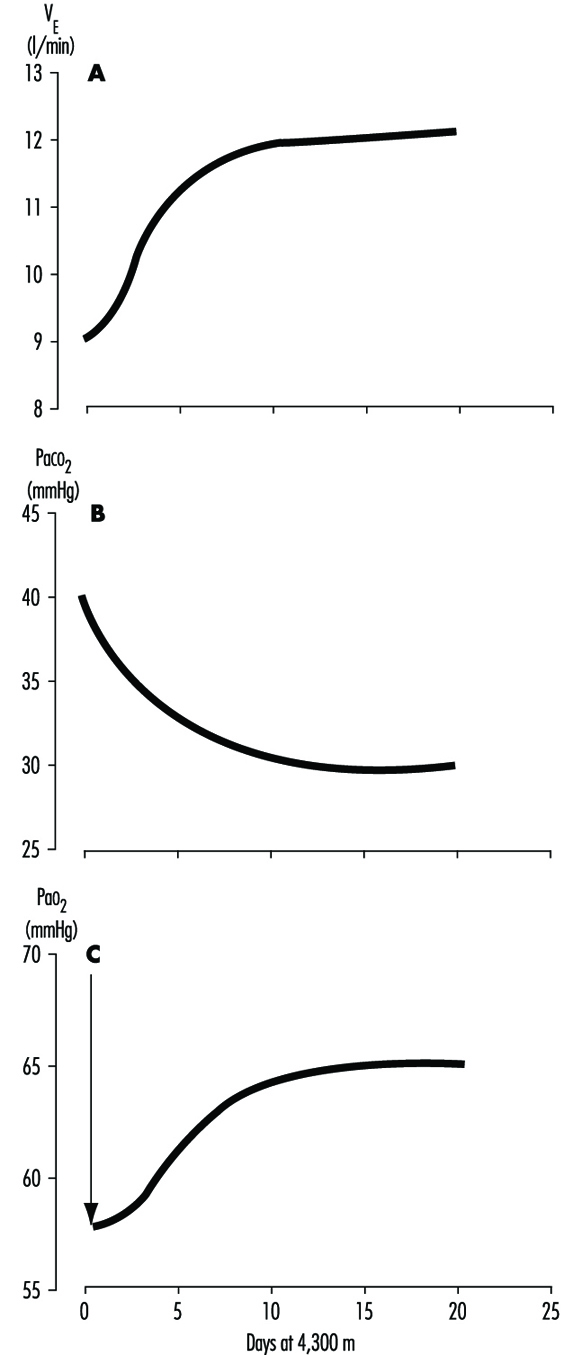
Because of the possibility of transient hypoxic ventilatory depression at altitude, and because acclimatization is a process which begins only upon entering a low oxygen environment, the minimal arterial oxygen pressure occurs upon arrival at altitude. Thereafter, the arterial oxygen pressure rises relatively rapidly for the initial days and thereafter increases more slowly, as in figure 3. Because the hypoxia is worse soon after arrival, the lethargy and symptoms which accompany altitude exposure are also worse during the first hours and days. With acclimatization, a restored sense of well-being usually develops.
The time required for acclimatization increases with increasing altitude, consistent with the concept that greater increase in ventilation and acid-base adjustments require longer intervals for renal compensation to occur. Thus while acclimatization may require three to five days for a sea-level native to acclimatize at 3,000 m, for altitudes above 6,000 to 8,000 m, complete acclimatization, even if it is possible, may require six weeks or more (figure 4). When the altitude-acclimatized person returns to sea level, the process reverses. That is, the arterial oxygen pressure now rises to the sea-level value and ventilation falls. Now there is less CO2 exhaled, and CO2 pressure rises in the blood and in the respiratory centre. The acid-base balance is altered toward the acid side, and the kidneys must retain bicarbonate to restore balance. Although the time required for the loss of acclimatization is not as well understood, it seems to require approximately as long an interval as the acclimatization process itself. If so, then return from altitude, hypothetically, gives a mirror image of altitude ascent, with one important exception: arterial oxygen pressures immediately become normal on descent.
Figure 4. Effects of altitude on barometric pressure and inspired PO2
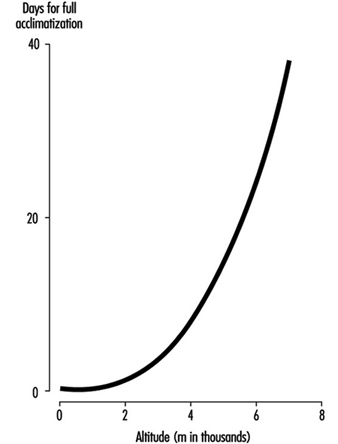
Variability among individuals
As might be expected, individuals vary with regard to time required for, and magnitude of, ventilatory acclimatization to a given altitude. One very important reason is the large variation between individuals in the ventilatory response to hypoxia. For example, at sea level, if one holds the CO2 pressure constant, so that it does not confound the ventilatory response to low oxygen, some normal persons show little or no increase in ventilation, while others show a very large (up to fivefold) increase. The ventilatory response to breathing low-oxygen mixtures seems to be an inherent characteristic of an individual, because family members behave more alike than do persons who are not related. Those persons who have poor ventilatory responses to low oxygen at sea level, as expected, also seem to have smaller ventilatory responses over time at high altitude. There may be other factors causing inter-individual variability in acclimatization, such as variability in the magnitude of ventilatory depression, in the function of the respiratory centre, in sensitivity to acid-base changes, and in renal handling of bicarbonate, but these have not been evaluated.
Sleep
Poor sleep quality, particularly before there is ventilatory acclimatization, is not only a common complaint, but also a factor that will impair occupational efficiency. Many things interfere with the act of breathing., including emotions, physical activity, eating and the degree of wakefulness. Ventilation decreases during sleep, and the capacity for breathing to be stimulated by low oxygen or high CO2 also decreases. Respiratory rate and depth of breathing both decrease. Further, at high altitude, where there are fewer oxygen molecules in the air, the amount of oxygen stored in the lung alveoli between breaths is less. Thus if breathing ceases for a few seconds (called apnoea, which is a common event at high altitude), the arterial oxygen pressure falls more rapidly than at sea level, where, in essence, the reservoir for oxygen is greater.
Periodic cessation of breathing is almost universal during the first few nights following ascent to high altitude. This is a reflection of the respiratory dilemma of altitude, described earlier, working in cyclic fashion: hypoxic stimulation increases ventilation, which in turn lowers carbon dioxide levels, inhibits breathing, and increases hypoxic stimulation, which again stimulates ventilation. Usually there is an apnoeic period of 15 to 30 seconds, followed by several very large breaths, which often briefly awakens the subject, after which there is another apnoea. The arterial oxygen pressure sometimes falls to alarming levels as a result of the apnoeic periods. There may be frequent awakenings, and even when total sleep time is normal its fragmentation impairs sleep quality such that there is the impression of having had a restless or sleepless night. Giving oxygen eliminates the cycling of hypoxic stimulation, and alkalotic inhibition abolishes the periodic breathing and restores normal sleep.
Middle-aged males in particular also are at risk for another cause of apnoea, namely intermittent obstruction of the upper airway, the common cause of snoring. While intermittent obstruction at the back of the nasal passages usually causes only annoying noise at sea level, at high altitude, where there is a smaller reservoir of oxygen in the lungs, such obstruction may lead to severely low levels of arterial oxygen pressure and poor sleep quality.
Intermittent Exposure
There are work situations, particularly in the Andes of South America, that require a worker to spend several days at altitudes above 3,000 to 4,000 m, and then to spend several days at home, at sea level. The particular work schedules (how many days are to be spent at altitude, say four to 14, and how many days, say three to seven, at sea level) are usually determined by the economics of the workplace more than by health considerations. However, a factor to be considered in the economics is the interval required both for acclimatization and loss of acclimatization to the altitude in question. Particular attention should be placed on the worker’s sense of well-being and performance on the job on arrival and the first day or two thereafter, regarding fatigue, time required to perform routine and non-routine functions, and errors made. Also strategies should be considered to minimize the time required for acclimatization at altitude, and to improve function during the waking hours.
Physiological Effects of Reduced Barometric Pressure
The major effects of high altitude on humans relate to the changes in barometric pressure (PB) and its consequential changes in the ambient pressure of oxygen (O2). Barometric pressure decreases with increasing altitude in a logarithmic fashion and can be estimated by the following equation:
![]()
where a = altitude, expressed in metres. In addition, the relationship of barometric pressure to altitude is influenced by other factors such as distance from the equator and season. West and Lahiri (1984) found that direct measurements of barometric pressure near the equator and at the summit of Mt. Everest (8,848 m) were greater than predictions based on the International Civil Aviation Organization Standard Atmosphere. Weather and temperature also affect the relationship between barometric pressure and altitude to the extent that a low-pressure weather system can reduce pressure, making sojourners to high altitude “physiologically higher”. Since the inspired partial pressure of oxygen (PO2) remains constant at approximately 20.93% of barometric pressure, the most important determinant of inspired PO2 at any altitude is the barometric pressure. Thus, inspired oxygen decreases with increasing altitude due to decreased barometric pressure, as shown in figure 1.
Figure 1. Effects of altitude on barometric pressure and inspired PO2
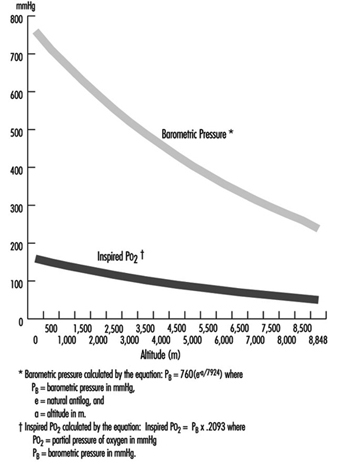
Temperature and ultraviolet radiation also change at high altitudes. Temperature decreases with increasing altitude at a rate of approximately 6.5 °C per 1,000 m. Ultraviolet radiation increases approximately 4% per 300 m due to decreased cloudiness, dust, and water vapour. In addition, as much as 75% of ultraviolet radiation can be reflected back by snow, further increasing exposure at high altitude. Survival in high altitude environments is dependent on adaptation to and/or protection from each of these elements.
Acclimatization
While rapid ascent to high altitudes often results in death, slow ascent by mountaineers can be successful when accompanied by compensatory physiological adaptation measures. Acclimatization to high altitudes is geared towards maintaining an adequate supply of oxygen to meet metabolic demands despite the decreasing inspired PO2. In order to achieve this goal, changes occur in all organ systems involved with oxygen uptake into the body, distribution of O2 to the necessary organs, and O2 unloading to the tissues.
Discussion of oxygen uptake and distribution requires understanding the determinants of oxygen content in the blood. As air enters the alveolus, the inspired PO2 decreases to a new level (called the alveolar PO2) because of two factors: increased partial pressure of water vapour from humidification of inspired air, and increased partial pressure of carbon dioxide (PCO2) from CO2 excretion. From the alveolus, oxygen diffuses across the alveolar capillary membrane into the blood as a result of a gradient between alveolar PO2 and blood PO2. The majority of oxygen found in blood is bound to haemoglobin (oxyhaemoglobin). Thus, oxygen content is directly related to both the haemoglobin concentration in the blood and the percentage of O2 binding sites on haemoglobin that are saturated with oxygen (oxyhaemoglobin saturation). Therefore, understanding the relationship between arterial PO2 and oxyhaemoglobin saturation is essential for understanding the determinants of oxygen content in the blood. Figure 2 illustrates the oxyhaemoglobin dissociation curve. With increasing altitude, inspired PO2 decreases and, therefore, arterial PO2 and oxyhaemoglobin saturation decreases. In normal subjects, altitudes greater than 3,000 m are associated with sufficiently decreased arterial PO2 that oxyhaemoglobin saturation falls below 90%, on the steep portion of the oxyhaemoglobin dissociation curve. Further increases in altitude will predictably result in significant desaturation in the absence of compensatory mechanisms.
Figure 2. Oxyhaemoglobin dissociation curve
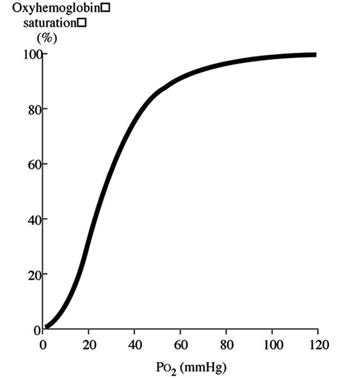
The ventilatory adaptations that occur in high-altitude environments protect the arterial partial pressure of oxygen against the effects of decreasing ambient oxygen levels, and can be divided into acute, subacute and chronic changes. Acute ascent to high altitude results in a fall in the inspired PO2 which in turn leads to a decrease in the arterial PO2 (hypoxia). In order to minimize the effects of decreased inspired PO2 on arterial oxyhaemoglobin saturation, the hypoxia that occurs at high altitude triggers an increase in ventilation, mediated through the carotid body (hypoxic ventilatory response–HVR). Hyperventilation increases carbon dioxide excretion and subsequently the arterial and then the alveolar partial pressure of carbon dioxide (PCO2) falls. The fall in alveolar PCO2 allows alveolar PO2 to rise, and consequently, arterial PO2 and arterial O2 content increases. However, the increased carbon dioxide excretion also causes a decrease in blood hydrogen ion concentration ([H+]) leading to the development of alkalosis. The ensuing alkalosis inhibits the hypoxic ventilatory response. Thus, on acute ascent to high altitude there is an abrupt increase in ventilation that is modulated by the development of an alkalosis in the blood.
Over the next several days at high altitude, further changes in ventilation occur, commonly referred to as ventilatory acclimatization. Ventilation continues to increase over the next several weeks. This further increase in ventilation occurs as the kidney compensates for the acute alkalosis by excretion of bicarbonate ions, with a resultant rise in blood [H+]. It was initially believed that renal compensation for the alkalosis removed the inhibitory influence of alkalosis on the hypoxic ventilatory response, thereby allowing the full potential of the HVR to be reached. However, measurements of blood pH revealed that the alkalosis persists despite the increase in ventilation. Other postulated mechanisms include: (1) cerebrospinal fluid (CSF) pH surrounding the respiratory control centre in the medulla may have returned to normal despite the persistent serum alkalosis; (2) increased sensitivity of the carotid body to hypoxia; (3) increased response of the respiratory controller to CO2. Once ventilatory acclimatization has occurred, both hyperventilation and the increased HVR persist for several days after return to lower altitudes, despite resolution of hypoxia.
Further ventilatory changes occur after several years of living at high altitude. Measurements in high-altitude natives have shown a decreased HVR when compared to values obtained in acclimatized individuals, although not to levels seen in subjects at sea level. The mechanism for the decreased HVR is unknown, but may be related to hypertrophy of the carotid body and/or development of other adaptive mechanisms for preserving tissue oxygenation such as: increased capillary density; increased gas exchange capacity of the tissues; increased number and density of mitochondria; or increased vital capacity.
In addition to its effect on ventilation, hypoxia also induces constriction of the vascular smooth muscle in the pulmonary arteries (hypoxic vasoconstriction). The ensuing increase in pulmonary vascular resistance and pulmonary artery pressure redirects blood flow away from poorly ventilated alveoli with low alveolar PO2 and towards better ventilated alveoli. In this manner, pulmonary arterial perfusion is matched to lung units that are well ventilated, providing another mechanism for preserving arterial PO2.
Oxygen delivery to the tissues is further enhanced by adaptations in the cardiovascular and haematological systems. On initial ascent to high altitude, heart rate increases, resulting in an increase in cardiac output. Over several days, cardiac output falls due to decreased plasma volume, caused by an increased water loss that occurs at high altitudes. With more time, increased erythropoietin production leads to increased haemoglobin concentration, providing the blood with increased oxygen-carrying capacity. In addition to increasing levels of haemoglobin, changes in the avidity of oxygen binding to haemoglobin may also help maintain tissue oxygenation. A shift of the oxyhaemoglobin dissociation curve to the right may be expected because it would favour release of oxygen to the tissues. However, data obtained from the summit of Mt. Everest and from hypobaric chamber experiments simulating the summit suggest that the curve is shifted to the left (West and Lahiri 1984; West and Wagner 1980; West et al. 1983). Although a left shift would make oxygen unloading to the tissues more difficult, it may be advantageous at extreme altitudes because it would facilitate oxygen uptake in the lungs despite markedly reduced inspired PO2 (43 mmHg on the summit of Mt. Everest versus 149 mmHg at sea level).
The last link in the chain of oxygen supply to the tissues is cellular uptake and utilization of O2. Theoretically, there are two potential adaptations that can occur. First, minimization of the distance that oxygen has to travel on diffusion out of the blood vessel and into the intracellular site responsible for oxidative metabolism, the mitochondria. Second, biochemical alterations can occur that improve mitochondrial function. Minimization of diffusion distance has been suggested by studies that show either increased capillary density or increased mitochondrial density in muscle tissue. It is unclear whether these changes reflect either recruitment or development of capillaries and mitochondria, or are an artefact due to muscle atrophy. In either case, the distance between the capillaries and the mitochondria would be decreased, thereby facilitating oxygen diffusion. Biochemical alterations that may improve mitochondrial function include increased myoglobin levels. Myoglobin is an intracellular protein that binds oxygen at low tissue PO2 levels and facilitates oxygen diffusion into the mitochondria. Myoglobin concentration increases with training and correlates with muscle cell aerobic capacity. Although these adaptations are theoretically beneficial, conclusive evidence is lacking.
Early accounts of high altitude explorers describe changes in cerebral function. Decreased motor, sensory and cognitive abilities, including decreased ability to learn new tasks and difficulty expressing information verbally, have all been described. These deficits may lead to poor judgement and to irritability, further compounding the problems encountered in high-altitude environments. On return to sea level, these deficits improve with a variable time course; reports have indicated impaired memory and concentration lasting from days to months, and decreased finger-tapping speed for one year (Hornbein et al. 1989). Individuals with greater HVR are more susceptible to long-lasting deficits, possibly because the benefit of hyperventilation on arterial oxyhaemoglobin saturation may be offset by hypocapnia (decreased PCO2 in the blood), which causes constriction of the cerebral blood vessels leading to decreased cerebral blood flow.
The preceding discussion has been limited to resting conditions; exercise provides an additional stress as oxygen demand and consumption increases. The fall in ambient oxygen at high altitude causes a fall in maximal oxygen uptake and, therefore, maximal exercise. In addition, the decreased inspired PO2 at high altitudes severely impairs oxygen diffusion into the blood. This is illustrated in figure 3, which plots the time course of oxygen diffusion into the alveolar capillaries. At sea level, there is excess time for equilibration of end-capillary PO2 to alveolar PO2, whereas at the summit of Mt. Everest, full equilibration is not realized. This difference is due to the decreased ambient oxygen level at high altitudes leading to a decreased diffusion gradient between alveolar and venous PO2. With exercise, cardiac output and blood flow increase, thereby reducing transit time of blood cells across the alveolar capillary, further exacerbating the problem. From this discussion, it becomes apparent that the left shift in the O2 and haemoglobin dissociation curve with altitude is necessary as compensation for the decreased diffusion gradient for oxygen in the alveolus.
Figure 3. The calculated time course of oxygen tension in the alveolar capillary
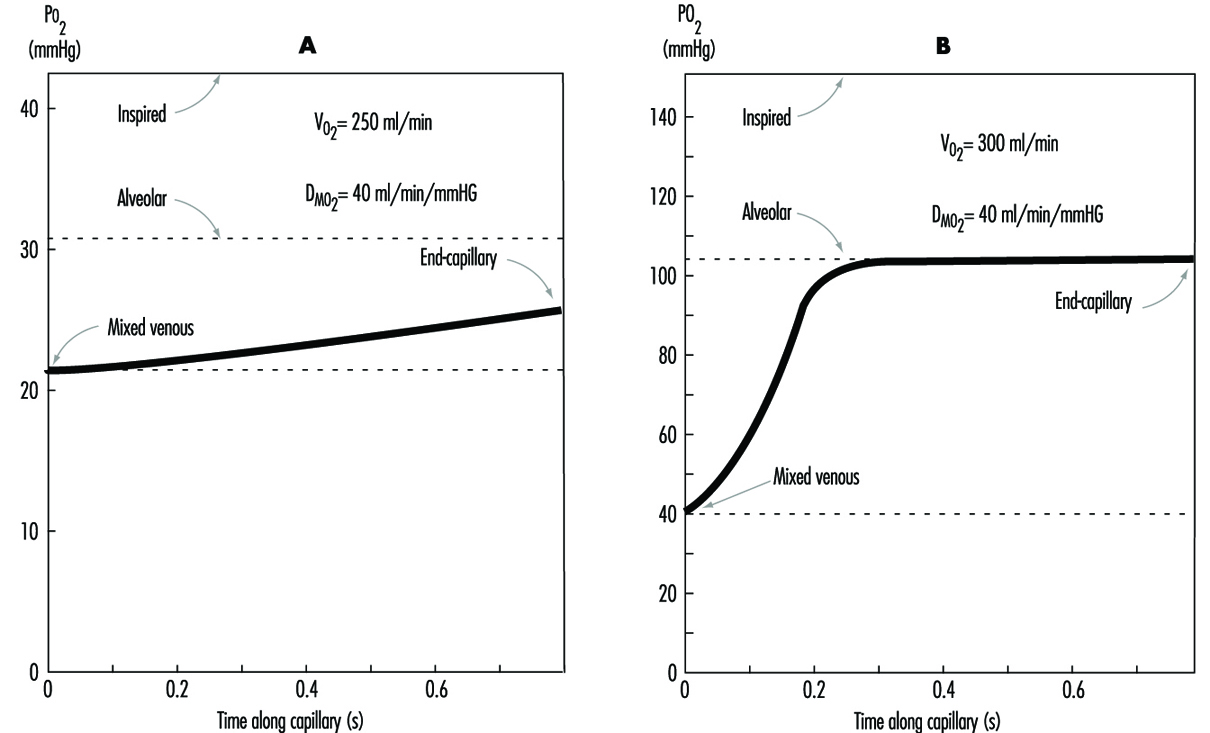
Disturbed sleep is common among sojourners at high altitude. Periodic (Cheyne-Stokes) breathing is universal and characterized by periods of rapid respiratory rate (hyperpnoea) alternating with periods of absent respirations (apnoea) leading to hypoxia. Periodic breathing tends to be more pronounced in individuals with the greatest hypoxic ventilatory sensitivity. Accordingly, sojourners with lower HVR have less severe periodic breathing. However, sustained periods of hypoventilation are then seen, corresponding with sustained decreases in oxyhaemoglobin saturation. The mechanism for periodic breathing probably relates to increased HVR causing increased ventilation in response to hypoxia. The increased ventilation leads to increased blood pH (alkalosis), which in turn suppresses ventilation. As acclimatization progresses, periodic breathing improves. Treatment with acetazolamide reduces periodic breathing and improves arterial oxyhaemoglobin saturation during sleep. Caution should be used with medications and alcohol that suppress ventilation, as they may exacerbate the hypoxia seen during sleep.
Pathophysiological Effects of Reduced Barometric Pressure
The complexity of human physiological adaptation to high altitude provides numerous potential maladaptive responses. Although each syndrome will be described separately, there is considerable overlap between them. Illnesses such as acute hypoxia, acute mountain sickness, high-altitude pulmonary oedema, and high-altitude cerebral oedema most likely represent a spectrum of abnormalities that share a similar pathophysiology.
Hypoxia
Hypoxia occurs with ascent to high altitudes because of the decreased barometric pressure and the resultant decrease in ambient oxygen. With rapid ascent, hypoxia occurs acutely, and the body does not have time to adjust. Mountaineers have generally been protected from the effects of acute hypoxia because of the time that elapses, and hence the acclimatization that occurs, during the climb. Acute hypoxia is problematic for both aviators and rescue personnel in high-altitude environments. Acute oxyhaemoglobin desaturation to values less than 40 to 60% leads to loss of consciousness. With less severe desaturation, individuals note headache, confusion, drowsiness and loss of coordination. Hypoxia also induces a state of euphoria which Tissandier, during his balloon flight in 1875, described as experiencing “inner joy”. With more severe desaturation, death occurs. Acute hypoxia responds rapidly and completely to either administration of oxygen or descent.
Acute mountain sickness
Acute mountain sickness (AMS) is the most common disorder in high-altitude environments and afflicts up to two-thirds of sojourners. The incidence of acute mountain sickness is dependent on multiple factors, including rate of ascent, length of exposure, degree of activity, and individual susceptibility. Identification of affected individuals is important in order to prevent progression to pulmonary or cerebral oedema. Identification of acute mountain sickness is made through recognition of characteristic signs and symptoms occurring in the appropriate setting. Most often, acute mountain sickness occurs within a few hours of a rapid ascent to altitudes greater than 2,500 m. The most common symptoms include headache that is more pronounced at night, loss of appetite that may be accompanied by nausea and vomiting, disturbed sleep, and fatigue. Individuals with AMS often complain of shortness of breath, cough and neurological symptoms such as memory deficits and auditory or visual disturbances. Findings on physical exam may be lacking, although fluid retention may be an early sign. The pathogenesis of acute mountain illness may relate to relative hypoventilation that would increase cerebral blood flow and intracranial pressure by increasing arterial PCO2 and decreasing arterial PO2. This mechanism may explain why persons with greater HVR are less likely to develop acute mountain sickness. The mechanism for fluid retention is not well understood, but may be related to abnormal plasma levels for proteins and/or hormones that regulate renal excretion of water; these regulators may respond to the increased activity of the sympathetic nervous system noted in patients with acute mountain sickness. The accumulation of water may in turn lead to the development of oedema or swelling of the interstitial spaces in the lungs. More severe cases may go on to develop pulmonary or cerebral oedema.
Prevention of acute mountain sickness can be accomplished through slow, graded ascent, allowing adequate time for acclimatization. This may be especially important for those individuals with greater susceptibility or a prior history of acute mountain sickness. In addition, administration of acetazolamide before or during ascent may help prevent and ameliorate symptoms of acute mountain sickness. Acetazolamide inhibits the action of carbonic anhydrase in the kidneys and leads to increased excretion of bicarbonate ions and water, producing an acidosis in the blood. The acidosis stimulates respiration, leading to increased arterial oxyhaemoglobin saturation and decreased periodic breathing during sleep. Through this mechanism, acetazolamide speeds the natural process of acclimatization.
Treatment of acute mountain sickness can be accomplished most effectively by descent. Further ascent to high altitudes is contra-indicated, as the disease may progress. When descent is not possible, oxygen may be administered. Alternatively, portable lightweight fabric hyperbaric chambers may be brought on expeditions to high-altitude environments. Hyperbaric bags are particularly valuable when oxygen is not available and descent is not possible. Several drugs are available that improve symptoms of acute mountain sickness, including acetazolamide and dexamethasone. The mechanism of action of dexamethasone is unclear, although it may act by decreasing oedema formation.
High-altitude pulmonary oedema
High-altitude pulmonary oedema affects approximately 0.5 to 2.0% of individuals who ascend to altitudes greater than 2,700 m and is the most common cause of death due to illnesses encountered at high altitudes. High-altitude pulmonary oedema develops from 6 to 96 hours after ascent. Risk factors for the development of high-altitude pulmonary oedema are similar to those for acute mountain sickness. Common early signs include symptoms of acute mountain sickness accompanied by decreased exercise tolerance, increased recovery time after exercise, shortness of breath on exertion, and persistent dry cough. As the condition worsens, the patient develops shortness of breath at rest, findings of audible congestion in the lungs, and cyanosis of the nail beds and lips. The pathogenesis of this disorder is uncertain but probably relates to increased microvascular pressure or increased permeability of the microvasculature leading to the development of pulmonary oedema. Although pulmonary hypertension may help explain the pathogenesis, elevation in the pulmonary artery pressure due to hypoxia has been observed in all individuals who ascend to high altitude, including those who do not develop pulmonary oedema. Nevertheless, susceptible individuals may possess uneven hypoxic constriction of the pul-monary arteries, leading to over-perfusion of the microvasculature in localized areas where hypoxic vasoconstriction was absent or diminished. The resulting increase in pressure and shear forces may damage the capillary membrane, leading to oedema formation. This mechanism explains the patchy nature of this disease and its appearance on x-ray examination of the lungs. As with acute mountain sickness, individuals with a lower HVR are more likely to develop high-altitude pulmonary oedema as they have lower oxyhaemoglobin saturations and, therefore, greater hypoxic pulmonary vasoconstriction.
Prevention of high-altitude pulmonary oedema is similar to prevention of acute mountain sickness and includes gradual ascent and use of acetazolamide. Recently, use of the smooth-muscle relaxing agent nifedipine has been shown to be of benefit in preventing disease in individuals with a prior history of high-altitude pulmonary oedema. Additionally, avoidance of exercise may have a preventive role, although it is probably limited to those individuals who already posses a subclinical degree of this disease.
Treatment of high-altitude pulmonary oedema is best accomplished by assisted evacuation to a lower altitude, keeping in mind that the victim needs to limit his or her exertion. After descent, improvement is rapid and additional treatment other than bed rest and oxygen are usually not necessary. When descent is not possible, oxygen therapy may be beneficial. Drug treatment has been attempted with multiple agents, most successfully with the diuretic furosemide and with morphine. Caution must be used with these drugs, as they can lead to dehydration, decreased blood pressure, and respiratory depression. Despite the effectiveness of descent as therapy, mortality remains at approximately 11%. This high mortality rate may reflect failure to diagnose the disease early in its course, or inability to descend coupled with lack of availability of other treatments.
High-altitude cerebral oedema
High-altitude cerebral oedema represents an extreme form of acute mountain sickness that has progressed to include generalized cerebral dysfunction. The incidence of cerebral oedema is unclear because it is difficult to differentiate a severe case of acute mountain sickness from a mild case of cerebral oedema. The pathogenesis of high-altitude cerebral oedema is an extension of the pathogenesis of acute mountain sickness; hypoventilation increases cerebral blood flow and intracranial pressure progressing to cerebral oedema. Early symptoms of cerebral oedema are identical to symptoms of acute mountain sickness. As the disease progresses, additional neurological symptoms are noted, including severe irritability and insomnia, ataxia, hallucinations, paralysis, seizures and eventually coma. Examination of the eyes commonly reveals swelling of the optic disc or papilloedema. Retinal haemorrhages are frequently noted. In addition, many cases of cerebral oedema have concurrent pulmonary oedema.
Treatment of high-altitude cerebral oedema is similar to treatment of other high-altitude disorders, with descent being the preferred therapy. Oxygen should be administered to maintain oxyhaemoglobin saturation greater that 90%. Oedema formation may be decreased with use of corticosteroids such as dexamethasone. Diuretic agents have also been utilized to decrease oedema, with uncertain efficacy. Comatose patients may require additional support with airway management. The response to treatment is variable, with neurological deficits and coma persisting for days to weeks after evacuation to lower altitudes. Preventative measures for cerebral oedema are identical to measures for other high-altitude syndromes.
Retinal haemorrhages
Retinal haemorrhages are extremely common, affecting up to 40% of individuals at 3,700 m and 56% at 5,350 m. Retinal haemorrhages are usually asymptomatic. They are most likely caused by increased retinal blood flow and vascular dilatation due to arterial hypoxia. Retinal haemorrhages are more common in individuals with headaches and can be precipitated by strenuous exercise. Unlike other high-altitude syndromes, retinal haemorrhages are not preventable by acetazolamide or furosemide therapy. Spontaneous resolution is usually seen within two weeks.
Chronic mountain sickness
Chronic mountain sickness (CMS) afflicts residents and long-term inhabitants of high altitude. The first description of chronic mountain sickness reflected Monge’s observations of Andean natives living at altitudes above 4,000 m. Chronic mountain sickness, or Monge’s disease, has since been described in most high-altitude dwellers except Sherpas. Males are more commonly affected than females. Chronic mountain sickness is characterized by plethora, cyanosis and elevated red blood cell mass leading to neurological symptoms that include headache, dizziness, lethargy and impaired memory. Victims of chronic mountain sickness may develop right heart failure, also called cor pulmonale, due to pulmonary hypertension and markedly reduced oxyhaemoglobin saturation. The pathogenesis of chronic mountain sickness is unclear. Measurements from affected individuals have revealed a decreased hypoxic ventilatory response, severe hypoxemia that is exacerbated during sleep, increased haemoglobin concentration and increased pulmonary artery pressure. Although a cause-and-effect relationship seems likely, evidence is lacking and often confusing.
Many symptoms of chronic mountain sickness can be ameliorated by descent to sea level. Relocation to sea level removes the hypoxic stimulus for red blood cell production and pulmonary vasoconstriction. Alternate treatments include: phlebotomy to reduce red blood cell mass, and low-flow oxygen during sleep to improve hypoxia. Therapy with medroxyprogesterone, a respiratory stimulant, has also been found to be effective. In one study, ten weeks of medroxyprogesterone therapy was followed by improved ventilation and hypoxia, and decreased red blood cell counts.
Other conditions
Patients with sickle cell disease are more likely to suffer from painful vaso-occlusive crisis at high altitude. Even moderate altitudes of 1,500 m have been known to precipitate crises, and altitudes of 1,925 m are associated with a 60% risk of crises. Patients with sickle cell disease residing at 3,050 m in Saudi Arabia have twice as many crises as patients residing at sea level. In addition, patients with sickle cell trait may develop splenic infarct syndrome on ascent to high altitude. Likely aetiologies for the increased risk of vaso-occlusive crisis include: dehydration, increased red blood cell count, and immobility. Treatment of vaso-occlusive crisis includes descent to sea level, oxygen and intravenous hydration.
Essentially no data exist describing the risk to pregnant patients on ascent to high altitudes. Although patients residing at high altitude have an increased risk of pregnancy-induced hypertension, no reports of increased foetal demise exist. Severe hypoxia may cause abnormalities in foetal heart rate; however, this occurs only at extreme altitudes or in the presence of high-altitude pulmonary oedema. Therefore, the greatest risk to the pregnant patient may relate to the remoteness of the area rather than to altitude-induced complications.
Health Considerations for Managing Work at High Altitudes
Large numbers of people work at high altitudes, particularly in the cities and villages of the South American Andes and the Tibetan plateau. The majority of these people are highlanders who have lived in the area for many years and perhaps several generations. Much of the work is agricultural in nature—for example, tending domesticated animals.
However, the focus of this article is different. Recently there has been a large increase in commercial activities at altitudes of 3,500 to 6,000 m. Examples include mines in Chile and Peru at altitudes of around 4,500 m. Some of these mines are very large, employing over 1,000 workers. Another example is the telescope facility at Mauna Kea, Hawaii, at an altitude of 4,200 m.
Traditionally, the high mines in the South American Andes, some of which date back to the Spanish colonial period, have been worked by indigenous people who have been at high altitude for generations. Recently however, increasing use is being made of workers from sea level. There are several reasons for this change. One is that there are not enough people in these remote areas to operate the mines. An equally important reason is that as the mines become increasingly automated, skilled people are required to operate large digging machines, loaders and trucks, and local people may not have the necessary skills. A third reason is the economics of developing these mines. Whereas previously whole towns were set up in the vicinity of the mine to accommodate the workers’ families, and necessary ancillary facilities such as schools and hospitals, it is now seen to be preferable to have the families live at sea level, and have the workers commute to the mines. This is not purely an economic issue. The quality of life at an altitude of 4,500 m is less than at lower altitudes (e.g., children grow more slowly). Therefore the decision to have the families remain at sea level while the workers commute to high altitude has a sound socio-economic basis.
The situation where a workforce moves from sea level to altitudes of approximately 4,500 m raises many medical issues, many of which are poorly understood at the present time. Certainly most people who travel from sea level to an altitude of 4,500 m develop some symptoms of acute mountain sickness initially. Tolerance to the altitude often improves after the first two or three days. However, the severe hypoxia of these altitudes has a number of deleterious effects on the body. Maximal work capacity is decreased, and people fatigue more rapidly. Mental efficiency is reduced and many people find it is much more difficult to concentrate. Sleep quality is often poor, with frequent arousals and periodic breathing (the breathing waxes and wanes three or four times every minute) with the result that that the arterial PO2 falls to low levels following the periods of apnoea or reduced breathing.
Tolerance to high altitude varies greatly between individuals, and it is often very difficult to predict who is going to be intolerant of high altitude. A substantial number of people who would like to work at an altitude of 4,500 m find that they are unable to do so, or that the quality life is so poor that they refuse to remain at that altitude. Topics such as the selection of workers who are likely to tolerate high altitude, and the scheduling of their work between high altitude and the period with their families at sea level, are relatively new and not well understood.
Pre-employment Examination
In addition to the usual type of pre-employment examination, special attention should be given to the cardio-pulmonary system, because working at high altitude makes great demands on the respiratory and cardiovascular systems. Medical conditions such as early chronic obstructive pulmonary disease and asthma will be much more disabling at high altitude because of the high levels of ventilation, and should be specifically looked for. A heavy cigarette smoker with symptoms of early bronchitis is likely to have difficulty tolerating high altitude. Forced spirometry should be measured in addition to the usual chest examination including chest radiograph. If possible, an exercise test should be carried out because any exercise intolerance will be exaggerated at high altitude.
The cardiovascular system should be carefully examined, including an exercise electrocardiogram if that is feasible. Blood counts should be made to exclude workers with unusual degrees of anaemia or polycythaemia.
Living at high altitude increases the psychological stress in many people, and a careful history should be taken to exclude prospective workers with previous behavioural problems. Many modern mines at high altitude are dry (no alcohol permitted). Gastro-intestinal symptoms are common in some people at high altitude, and workers who have a history of dyspepsia may do poorly.
Selection of Workers to Tolerate High Altitude
In addition to excluding workers with lung or heart disease who are likely to do poorly at high altitude, it would be very valuable if tests could be carried out to determine who is likely to tolerate altitude well. Unfortunately little is known at the present time about predictors of tolerance to high altitude, though considerable work is being done on this at the present time.
The best predictor of tolerance to high altitude is probably previous experience at high altitude. If someone has been able to work at an altitude of 4,500 m for several weeks without appreciable problems, it is very likely that he or she will be able to do this again. By the same token, somebody who tried to work at high altitude and found that he or she could not tolerate it, is very likely to have the same problem next time. Therefore in selecting workers, a great deal of emphasis should be placed on successful previous employment at high altitude. However, clearly this criterion cannot be used for all workers because otherwise no new people would enter the high-altitude working pool.
Another possible predictor is the magnitude of the ventilatory response to hypoxia. This can be measured at sea level by giving the prospective worker a low concentration of oxygen to breathe and measuring the increase in ventilation. There is some evidence that people who have a relatively weak hypoxic ventilatory response tolerate high altitude poorly. For example, Schoene (1982) showed that 14 high-altitude climbers had significantly higher hypoxic ventilatory responses than ten controls. Further measurements were made on the 1981 American Medical Research Expedition to Everest, where it was shown that the hypoxic ventilatory response measured before and on the Expedition correlated well with performance high on the mountain (Schoene, Lahiri and Hackett 1984). Masuyama, Kimura and Sugita (1986) reported that five climbers who reached 8,000 m in Kanchenjunga had a higher hypoxic ventilatory response than five climbers who did not.
However, this correlation is by no means universal. In a prospective study of 128 climbers going to high altitudes, a measure of hypoxic ventilatory response did not correlate with the height reached, whereas a measurement of maximal oxygen uptake at sea level did correlate (Richalet, Kerome and Bersch 1988). This study also suggested that the heart rate response to acute hypoxia might be a useful predictor of performance at high altitude. There have been other studies showing a poor correlation between hypoxic ventilatory response and performance at extreme altitude (Ward, Milledge and West 1995).
The problem with many of these studies is that the results are chiefly applicable to much higher altitudes than of interest here. Also there are many examples of climbers with moderate values of hypoxic ventilatory response who do well at high altitude. Nevertheless, an abnormally low hypoxic ventilatory response is probably a risk factor for tolerating even medium altitudes such as 4,500 m.
One way of measuring the hypoxic ventilatory response at sea level is to have the subject rebreathe into a bag which is initially filled with 24% oxygen, 7% carbon dioxide, and the balance nitrogen. During rebreathing the PCO2 is monitored and held constant by means of a variable bypass and carbon dioxide absorber. Rebreathing can be continued until the inspired PO2 falls to about 40 mmHg (5.3 kPa). The arterial oxygen saturation is measured continually with a pulse oximeter, and the ventilation plotted against the saturation (Rebuck and Campbell 1974). Another way of measuring the hypoxic ventilatory response is to determine the inspiratory pressure during a brief period of airway occlusion while the subject is breathing a low-oxygen mixture (Whitelaw, Derenne and Milic-Emili 1975).
Another possible predictor of tolerance to high altitude is work capacity during acute hypoxia at sea level. The rationale here is that someone who is not able to tolerate acute hypoxia is more likely to be intolerant of chronic hypoxia. There is little evidence for or against this hypothesis. Soviet physiologists used tolerance to acute hypoxia as one of the criteria for selection of climbers for their successful 1982 Everest expedition (Gazenko 1987). On the other hand, the changes that occur with acclimatization are so profound that it would not be surprising if exercise performance during acute hypoxia were poorly correlated with the ability to work during chronic hypoxia.
Another possible predictor is the increase in pulmonary artery pressure during acute hypoxia at sea level. This can be measured non-invasively in many people by Doppler ultrasound. The main rationale for this test is the known correlation between the development of high-altitude pulmonary oedema and the degree of hypoxic pulmonary vasoconstriction (Ward, Milledge and West 1995). However, since high-altitude pulmonary oedema is uncommon in people working at an altitude of 4,500 m, the practical value of this test is questionable.
The only way to determine whether these tests for the selection of workers have practical value is a prospective study where the results of the tests done at sea level are correlated with subsequent assessment of tolerance to high altitude. This raises the question of how high-altitude tolerance will be measured. The usual way of doing this is by questionnaires such as the Lake Louise questionnaire (Hackett and Oelz 1992). However, questionnaires may be unreliable in this population because workers perceive that if they admit to altitude intolerance, they might lose their jobs. It is true that there are objective measures of altitude intolerance such as quitting work, rales in the lungs as indications of subclinical pulmonary oedema, and mild ataxia as an indication of subclinical high-altitude cerebral oedema. However, these features will be seen only in people with severe altitude intolerance, and a prospective study based solely on such measurements would be very insensitive.
It should be emphasized that the value of these possible tests for determining tolerance to working at high altitude has not been established. However, the economic implications of taking on a substantial number of workers who are unable to perform satisfactorily at high altitude are such that it would be very valuable to have useful predictors. Studies are presently underway to determine whether some of these predictors are valuable and feasible. Measurements such as the hypoxic ventilatory response to hypoxia, and work capacity during acute hypoxia at sea level, are not particularly difficult. However, they need to be done by a professional laboratory, and the cost of these investigations can be justified only if the predictive value of the measurements is substantial.
Scheduling between High Altitude and Sea Level
Again, this article is addressed to the specific problems which occur when commercial activities such as mines at altitudes of about 4,500 m employ workers who commute from sea level where their families live. Scheduling is obviously not an issue where people live permanently at high altitude.
Designing the optimal schedule for moving between high altitude and sea level is a challenging problem, and as yet there is little scientific basis for the schedules that have been employed so far. These have been based mainly on social factors such as how long the workers are willing to spend at high altitude before seeing their families again.
The main medical rationale for spending several days at a time at high altitude is the advantage gained from acclimatization. Many people who develop symptoms of acute mountain sickness after going to high altitude feel much better after two to four days. Therefore rapid acclimatization is occurring over this period. In addition it is known that the ventilatory response to hypoxia takes seven to ten days to reach a steady state (Lahiri 1972; Dempsey and Forster 1982). This increase in ventilation is one of the most important features of the acclimatization process, and therefore it is reasonable to recommend that the working period at high altitude be at least ten days.
Other features of high-altitude acclimatization probably take much longer to develop. One example is polycythaemia, which takes several weeks to reach a steady state. However, it should be added that the physiological value of polycythaemia is much less certain than was thought at one time. Indeed, Winslow and Monge (1987) have shown that the severe degrees of polycythaemia which are sometimes seen in permanent dwellers at altitudes of about 4,500 m are counterproductive in that work capacity can sometimes be increased if the haematocrit is lowered by removing blood over several weeks.
Another important issue is the rate of deacclimatization. Ideally the workers should not lose all the acclimatization that they have developed at high altitude during their period with their families at sea level. Unfortunately, there has been little work on the rate of deacclimatization, although some measurements suggest that the rate of change of the ventilatory response during deacclimatization is slower than during acclimatization (Lahiri 1972).
Another practical issue is the time required to move workers from sea level to high altitude and back again. In a new mine at Collahuasi in north Chile, it takes only a few hours to reach the mine by bus from the coastal town of Iquique, where most of the families are expected to live. However, if the worker resides in Santiago, the trip could take over a day. Under these circumstances, a short working period of three or four days at high altitude would clearly be inefficient because of the time wasted in travelling.
Social factors also play a critical role in any scheduling that involves time away from the family. Even if there are medical and physiological reasons why an acclimatization period of 14 days is optimal, the fact that the workers are unwilling to leave their families for more than seven or ten days may be an overriding factor. Experience so far shows that a schedule of seven days at high altitude followed by seven days at sea level, or ten days at high altitude followed by the same period at sea level are probably the most acceptable schedules.
Note that with this type of schedule, the worker never fully acclimatizes to high altitude, nor fully deacclimatizes while at sea level. He therefore spends his time oscillating between the two extremes, never receiving the full benefit of either state. In addition, some workers complain of extreme tiredness when they return to sea level, and spend the first two or three days recovering. Possibly this is related to the poor quality of sleep which is often a feature of living at high altitude. These problems highlight our ignorance of the factors that determine the best schedules, and more work is clearly needed in this area.
Whatever schedule is used, it is highly advantageous if the workers can sleep at a lower altitude than the workplace. Naturally whether this is feasible depends on the topography of the region. A lower altitude for sleeping is not feasible if it takes several hours to reach it because this cuts too much off the working day. However, if there is a location several hundred metres lower which can be reached within, say, one hour, setting up sleeping quarters at this lower altitude will improve sleep quality, workers’ comfort and sense of well-being, and productivity.
Oxygen Enrichment of Room Air to Reduce the Hypoxia of High Altitude
The deleterious effects of high altitude are caused by the low partial pressure of oxygen in the air. In turn, this results from the fact that while the oxygen concentration is the same as at sea level, the barometric pressure is low. Unfortunately there is little that can be done at high altitude to counter this “climatic aggression”, as it was dubbed by Carlos Monge, the father of high-altitude medicine in Peru (Monge 1948).
One possibility is to increase the barometric pressure in a small area, and this is the principle of the Gamow bag, which is sometimes used for the emergency treatment of mountain sickness. However, pressurizing large spaces such as rooms is difficult from a technical point of view, and there are also medical problems associated with entering and leaving a room with increased pressure. An example is middle ear discomfort if the Eustachian tube is blocked.
The alternative is to raise the oxygen concentration in some parts of the work facility, and this is a relatively new development that shows great promise (West 1995). As pointed out earlier, even after a period of acclimatization of seven to ten days at an altitude of 4,500 m, severe hypoxia continues to reduce work capacity, mental efficiency and sleep quality. It would therefore be highly advantageous to reduce the degree of hypoxia in some parts of the work facility if that were feasible.
This can be done by adding oxygen to the normal air ventilation of some rooms. The value of relatively minor degrees of oxygen enrichment of the room air is remarkable. It has been shown that every 1% increase in oxygen concentration (for example from 21 to 22%) reduces the equivalent altitude by 300 m. The equivalent altitude is that which has the same inspired PO2 during air breathing as in the oxygen-enriched room. Thus at an altitude of 4,500 m, raising the oxygen concentration of a room from 21 to 26% would reduce the equivalent altitude by 1,500 m. The result would be an equivalent altitude of 3,000 m, which is easily tolerated. The oxygen would be added to the normal room ventilation and therefore would be part of the air conditioning. We all expect that a room will provide a comfortable temperature and humidity. Control of the oxygen concentration can be regarded as a further logical step in humanity’s control of our environment.
Oxygen enrichment has become feasible because of the introduction of relatively inexpensive equipment for providing large quantities of nearly pure oxygen. The most promising is the oxygen concentrator that uses a molecular sieve. Such a device preferentially adsorbs nitrogen and thus produces an oxygen-enriched gas from air. It is difficult to produce pure oxygen with this type of concentrator, but large amounts of 90% oxygen in nitrogen are readily available, and these are just as useful for this application. These devices can work continuously. In practice, two molecular sieves are used in an alternating fashion, and one is purged while the other is actively adsorbing nitrogen. The only requirement is electrical power, which is normally in abundant supply at a modern mine. As a rough indication of the cost of oxygen enrichment, a small commercial device can be bought off the shelf, and this produces 300 litres per hour of 90% oxygen. It was developed to produce oxygen for treating patients with lung disease in their homes. The device has a power requirement of 350 watts and the initial cost is about US$2,000. Such a machine is sufficient to raise the oxygen concentration in a room by 3% for one person at a minimal though acceptable level of room ventilation. Very large oxygen concentrators are also available, and they are used in the paper pulp industry. It is also possible that liquid oxygen might be economical under some circumstances.
There are several areas in a mine, for example, where oxygen enrichment might be considered. One would be the director’s office or conference room, where important decisions are being made. For example, if there is a crisis in the mine such as a serious accident, such a facility would probably result in clearer thinking than the normal hypoxic environment. There is good evidence that an altitude of 4,500 m impairs brain function (Ward, Milledge and West 1995). Another place where oxygen enrichment would be beneficial is a laboratory where quality control measurements are being carried out. A further possibility is oxygen enrichment of sleeping quarters to improve sleep quality. Double blind trials of the effectiveness of oxygen enrichment at altitudes of about 4,500 m would be easy to design and should be carried out as soon as possible.
Possible complications of oxygen enrichment should be considered. Increased fire hazard is one issue that has been raised. However, increasing the oxygen concentration by 5% at an altitude of 4,500 m produces an atmosphere which has a lower flammability than air at sea level (West 1996). It should be borne in mind that although oxygen enrichment increases the PO2, this is still much lower than the sea-level value. Flammability of an atmosphere depends on two variables (Roth 1964):
- the partial pressure of oxygen, which is much lower in the enriched air at high altitude than at sea level
- the quenching effect of the inert components (i.e., nitrogen) of the atmosphere.
This quenching is slightly reduced at high altitude, but the net effect is still a lower flammability. Pure or nearly pure oxygen is dangerous, of course, and the normal precautions should be taken in piping the oxygen from the oxygen concentrator to the ventilation ducting.
Loss of acclimatization to high altitude is sometimes cited as a disadvantage of oxygen enrichment. However, there is no basic difference between entering a room with an oxygen-enriched atmosphere, and descending to a lower altitude. Everybody would sleep at a lower altitude if they could, and therefore this is hardly an argument against using oxygen enrichment. It is true that frequent exposure to a lower altitude will result in less acclimatization to the higher altitude, other things being equal. However, the ultimate objective is effective working at the high altitude of the mine, and this can presumably be enhanced using oxygen enrichment.
It is sometimes suggested that altering the atmosphere in this way might increase the legal liability of the facility if some kind of hypoxia-related illness developed. Actually, the opposite view seems more reasonable. It is possible that a worker who develops, say, a myocardial infarction while working at high altitude could claim that the altitude was a contributing factor. Any procedure which reduces the hypoxic stress makes altitude-induced illnesses less likely.
Emergency Treatment
The various types of high-altitude sickness, including acute mountain sickness, high-altitude pulmonary oedema and high-altitude cerebral oedema, were discussed earlier in this chapter. Little needs to be added in the context of work at high altitude.
Anyone who develops a high-altitude illness should be allowed to rest. This may be sufficient for conditions such as acute mountain sickness. Oxygen should be given by mask if this is available. However, if the patient does not improve, or deteriorates, descent is by far the best treatment. Usually this is easily done in a large commercial facility, because transportation is always available. All the high-altitude-related illnesses usually respond rapidly to removal to lower altitude.
There may be a place in a commercial facility for a small pressurized container in which the patient can be placed, and the equivalent altitude reduced by pumping in air. In the field, this is commonly done using a strong bag. One design is known as the Gamow bag, after its inventor. However, the main advantage of the bag is its portability, and since this feature is not really essential in a commercial facility, it would probably be better to use a larger, rigid tank. This should be big enough for an attendant to be inside the facility with the patient. Of course adequate ventilation of such a container is essential. Interestingly, there is anecdotal evidence that raising the atmospheric pressure in this way is sometimes more efficacious in the treatment of high-altitude illness than giving the patient a high concentration of oxygen. It is not clear why this should be so.
Acute mountain sickness
This is usually self-limiting and the patient feels much better after a day or two. The incidence of acute mountain sickness can be reduced by taking acetazolamide (Diamox), one or two 250 mg tablets per day. These can be started before reaching high altitude or can be taken when symptoms develop. Even people with mild symptoms find that half a tablet at night often improves the quality of sleep. Aspirin or paracetamol is useful for headache. Severe acute mountain sickness can be treated with dexamethasone, 8 mg initially, followed by 4 mg every six hours. However, descent is by far the best treatment if the condition is severe.
High-altitude pulmonary oedema
This is a potentially serious complication of mountain sickness and must be treated. Again the best therapy is descent. While awaiting evacuation, or if evacuation is not possible, give oxygen or place in a high-pressure chamber. Nifedipine (a calcium channel blocker) should be given. The dose is 10 mg sublingually followed by 20 mg slow release. This results in a fall in pulmonary artery pressure and is often very effective. However, the patient should be taken down to a lower altitude.
High-altitude cerebral oedema
This is potentially a very serious complication and is an indication for immediate descent. While awaiting evacuation, or if evacuation is not possible, give oxygen or place in an increased pressure environment. Dexamethasone should be given, 8 mg initially, followed by 4 mg every six hours.
As indicated earlier, people who develop severe acute mountain sickness, high-altitude pulmonary oedema or high-altitude cerebral oedema are likely to have a recurrence if they return to high altitude. Therefore if a worker develops any of these conditions, attempts should be made to find employment at a lower altitude.
Prevention of Occupational Hazards at High Altitudes
Working at high altitudes induces a variety of biological responses, as described elsewhere in this chapter. The hyperventilatory response to altitude should cause a marked increase in the total dose of hazardous substances which may be inhaled by persons occupationally exposed, as compared to people working under similar conditions at sea level. This implies that 8-hour exposure limits used as the basis of exposure standards should be reduced. In Chile, for example, the observation that silicosis progresses faster in mines at high altitudes, led to the reduction of the permitted exposure level proportional to the barometric pressure at the workplace, when expressed in terms of mg/m3. While this may be overcorrecting at intermediate altitudes, the error will be in the favour the exposed worker. The threshold limit values (TLVs), expressed in terms of parts per million (ppm), require no adjustment, however, because both the proportion of millimoles of contaminant per mole of oxygen in air and the number of moles of oxygen required by a worker remain approximately constant at different altitudes, even though the air volume containing one mole of oxygen will vary.
In order to assure that this is true, however, the method of measurement used to determine the concentration in ppm must be truly volumetric, as is the case with Orsat’s apparatus or the Bacharach Fyrite instruments. Colourimetric tubes that are calibrated to read in ppm are not true volumetric measurements because the markings on the tube are actually caused by a chemical reaction between the air contaminant and some reagent. In all chemical reactions, substances combine in proportion to the number of moles present, not in proportion to volumes. The hand-operated air pump draws a constant volume of air through the tube at any altitude. This volume at a higher altitude will contain a smaller mass of contaminant, giving a reading lower than the actual volumetric concentration in ppm (Leichnitz 1977). Readings should be corrected by multiplying the reading by the barometric pressure at sea level and dividing the result by the barometric pressure at the sampling site, using the same units (such as torr or mbar) for both pressures.
Diffusional samplers: The laws of gas diffusion indicate that the collection efficiency of diffusional samplers is independent of barometric pressure changes. Experimental work by Lindenboom and Palmes (1983) shows that other, as yet undetermined factors influence the collection of NO2 at reduced pressures. The error is approximately 3.3% at 3,300 m and 8.5% at 5,400 m equivalent altitude. More research is needed on the causes of this variation and the effect of altitude on other gases and vapours.
No information is available on the effect of altitude on portable gas detectors calibrated in ppm, which are equipped with electrochemical diffusion sensors, but it could reasonably be expected that the same correction mentioned under colourimetric tubes would apply. Obviously the best procedure would be to calibrate them at altitude with a test gas of known concentration.
The principles of operation and measurement of electronic instruments should be examined carefully to determine whether they need recalibration when employed at high altitudes.
Sampling pumps: These pumps usually are volumetric—that is, they displace a fixed volume per revolution—but they usually are the last component of the sampling train, and the actual volume of air aspirated is affected by the resistance to flow opposed by the filters, hose, flow meters and orifices that are part of the sampling train. Rotameters will indicate a lower flow rate than that actually flowing through the sampling train.
The best solution of the problem of sampling at high altitudes is to calibrate the sampling system at the sampling site, obviating the problem of corrections. A briefcase sized bubble film calibration laboratory is available from sampling pump manufacturers. This is easily carried to location and permits rapid calibration under actual working conditions. It even includes a printer which provides a permanent record of calibrations made.
TLVs and Work Schedules
TLVs have been specified for a normal 8-hour workday and a 40-hour workweek. The present tendency in work at high altitudes is to work longer hours for a number of days and then commute to the nearest town for an extended rest period, keeping the average time at work within the legal limit, which in Chile is 48 hours per week.
Departures from the normal 8-hour working schedules make it necessary to examine the possible accumulation in the body of toxic substances due to the increase in exposure and reduction of detoxification times.
Chilean occupational health regulations have recently adopted the “Brief and Scala model’’ described by Paustenbach (1985) for reducing TLVs in the case of extended working hours. At altitude, the correction for barometric pressure should also be used. This usually results in very substantial reductions of permissible exposure limits.
In the case of cumulative hazards not subject to detoxifying mechanisms, such as silica, correction for extended working hours should be directly proportional to the actual hours worked in excess of the usual 2,000 hours per year.
Physical Hazards
Noise: The sound pressure level produced by noise of a given amplitude is in direct relation to air density, as is the amount of energy transmitted. This means that the reading obtained by a sound level meter and the effect on the inner ear are reduced in the same way, so no corrections would be required.
Accidents: Hypoxia has a pronounced influence on the central nervous system, reducing response time and disrupting vision. An increase in the incidence of accidents should be expected. Above 3,000 m, the performance of persons engaged in critical tasks will benefit from supplementary oxygen.
Precautionary Note: Air Sampling
Kenneth I. Berger and William N. Rom
The monitoring and maintenance of the occupational safety of workers requires special consideration for high altitude environments. High-altitude conditions can be expected to influence the accuracy of sampling and measuring instruments that have been calibrated for use at sea level. For example, active sampling devices rely on pumps to pull a volume of air onto a collection medium. Accurate measurement of the pump flow rate is essential in order to determine the exact volume of air drawn through the sampler and, therefore, the concentration of the contaminant. Flow calibrations are often performed at sea level. However, changes in air density with increasing altitude may alter the calibration, thereby invalidating subsequent measurements made in high altitude environments. Other factors that may influence the accuracy of sampling and measurement instruments at high altitude include changing temperature and relative humidity. An additional factor that should be considered when evaluating worker exposure to inhaled substances is the increased respiratory ventilation that occurs with acclimatization. Since ventilation is markedly increased after ascent to high altitude, workers may be exposed to excessive total doses of inhaled occupational contaminants, even though measured concentrations of the contaminant are below the threshold limit value.
Workplace Biohazards
The assessment of biohazards in the workplace has been concentrated on agricultural workers, health-care workers and laboratory personnel, who are at considerable risk of adverse health effects. A detailed compilation of biohazards by Dutkiewicz et al. (1988) shows how widespread the risks can be to workers in many other occupations as well (table 1).
Dutkiewicz et al. (1988) further taxonomically classified the micro-organisms and plants (table 2), as well as animals (table 3), which might possibly present biohazards in work settings.
Table 1. Occupational settings with potential exposure of workers to biological agents
|
Sector |
Examples |
|
Agriculture |
Cultivating and harvesting |
|
Agricultural products |
Abattoirs, food packaging plants |
|
Laboratory animal care |
|
|
Health care |
Patient care: medical, dental |
|
Pharmaceutical and herbal products |
|
|
Personal care |
Hairdressing, chiropody |
|
Clinical and research laboratories |
|
|
Biotechnology |
Production facilities |
|
Day-care centres |
|
|
Building maintenance |
“Sick” buildings |
|
Sewage and compost facilities |
|
|
Industrial waste disposal systems |
Source: Dutkiewicz et al. 1988.
Micro-organisms
Micro-organisms are a large and diverse group of organisms that exist as single cells or cell clusters (Brock and Madigan 1988). Microbial cells are thus distinct from the cells of animals and plants, which are unable to live alone in nature but can exist only as parts of multicellular organisms.
Very few areas on the surface of this planet do not support microbial life, because micro-organisms have an astounding range of metabolic and energy-yielding abilities and many can exist under conditions that are lethal to other life forms.
Four broad classes of micro-organisms that can interact with humans are bacteria, fungi, viruses and protozoa. They are hazardous to workers due to their wide distribution in the working environment. The most important micro-organisms of occupational hazard are listed in tables 2 and 3.
There are three major sources of such microbes:
- those arising from microbial decomposition of various substrates associated with particular occupations (e.g., mouldy hay leading to hypersensitivity pneumonitis)
- those associated with certain types of environments (e.g., bacteria in water supplies)
- those stemming from infective individuals harbouring a particular pathogen (e.g., tuberculosis).
Ambient air may be contaminated with or carry significant levels of a variety of potentially harmful micro-organisms (Burrell 1991). Modern buildings, especially those designed for commercial and administrative purposes, constitute a unique ecological niche with their own biochemical environment, fauna and flora (Sterling et al. 1991). The potential adverse effects on workers are described elsewhere in this Encyclopaedia.
Water has been recognized as an important vehicle for extra-intestinal infection. A variety of pathogens are acquired through occupational, recreational and even therapeutic contact with water (Pitlik et al. 1987). The nature of non-enteric water-borne disease is often determined by the ecology of aquatic pathogens. Such infections are of basically two types: superficial, involving damaged or previously intact mucosae and skin; and systemic, often serious infections that may occur in the setting of depressed immunity. A broad spectrum of aquatic organisms, including viruses, bacteria, fungi, algae and parasites may invade the host through such extra-intestinal routes as the conjunctivae, respiratory mucosae, skin and genitalia.
Although zoonotic spread of infectious disease continues to occur in laboratory animals used in biomedical research, reported outbreaks have been minimized with the advent of rigorous veterinary and husbandry procedures, the use of commercially reared animals and the institution of appropriate personnel health programmes (Fox and Lipman 1991). Maintaining animals in modern facilities with appropriate safeguards against the introduction of vermin and biological vectors is also important in preventing zoonotic disease in personnel. Nevertheless, established zoonotic agents, newly discovered micro-organisms or new animal species not previously recognized as carriers of zoonotic micro-organisms are encountered, and the potential for spread of infectious disease from animals to humans still exists.
Active dialogue between veterinarians and physicians regarding the potential of zoonotic disease, the species of animals that are involved, and the methods of diagnosis, is an indispensable component of a successful preventive health programme.
Table 2. Viruses, bacteria, fungi and plants: Known biohazards in the workplace
|
Infec- |
Infection zoo- |
Allergic |
Respir- |
Toxin |
Carcino- |
|
|
Viruses |
x |
x |
||||
|
Bacteria |
||||||
|
Rickettsiae |
x |
|||||
|
Chlamydiae |
x |
|||||
|
Spiral bacteria |
x |
|||||
|
Gram-negative |
|
|
|
|
||
|
Gram-positive |
|
|
||||
|
Spore-forming |
|
|
|
|||
|
Non-sporing gram- |
|
|
||||
|
Mycobacteria |
x |
x |
||||
|
Actinomycetes |
x |
|||||
|
Fungi |
||||||
|
Moulds |
x |
x |
x(m)3 |
x |
||
|
Dermatophytes |
x |
x |
x |
|||
|
Yeast-like geophilic |
|
|
||||
|
Endogenous yeasts |
x |
|||||
|
Parasites of wheat |
x |
|||||
|
Mushrooms |
x |
|||||
|
Other lower plants |
||||||
|
Lichens |
x |
|||||
|
Liverworts |
x |
|||||
|
Ferns |
x |
|||||
|
Higher plants |
||||||
|
Pollen |
x |
|||||
|
Volatile oils |
x |
x |
||||
|
Dusts-processing |
x |
x |
x |
1 Infection-zoonosis: Causes infection or invasion usually contracted from vertebrate animals (zoonosis).
2 (e) Endotoxin.
3 (m) Mycotoxin.
Source: Dutkiewicz et al. 1988.
Some Occupational Settings with Biohazards
Medical and laboratory staff and other health-care workers, including related professions, are exposed to infection by micro-organisms if the appropriate preventive measures are not taken. Hospital workers are exposed to many biological hazards, including human immunodeficiency virus (HIV), hepatitis B, herpes viruses, rubella and tuberculosis (Hewitt 1993).
Work in the agricultural sector is associated with a wide variety of occupational hazards. Exposure to organic dust, and to airborne micro-organisms and their toxins, may lead to respiratory disorders (Zejda et al. 1993). These include chronic bronchitis, asthma, hypersensitivity pneumonitis, organic dust toxic syndrome and chronic obstructive pulmonary disease. Dutkiewicz and his colleagues (1988) studied samples of silage for the identification of potential agents causing symptoms of organic and toxic syndrome. Very high levels of total aerobic bacteria and fungi were found. Aspergillus fumigatus predominated among the fungi, whereas bacillus and gram-negative organisms (Pseudomonas, Alcaligenes, Citrobacter and Klebsiella species) and actinomycetes prevailed among the bacteria. These results show that contact with aerosolized silage carries the risk of exposure to high concentrations of micro-organisms, of which A. fumigatus and endotoxin-producing bacteria are the most probable disease agents.
Short-term exposures to certain wood dusts may result in asthma, conjunctivitis, rhinitis or allergic dermatitis. Some thermophilic micro-organisms found in wood are human pathogens, and inhalation of ascomycete spores from stored wood chips has been implicated in human illnesses (Jacjels 1985).
Examples illustrative of specific working conditions follow:
- The fungus Penicillium camemberti var. candidum is used in the production of some types of cheese. The high frequency of precipitating antibodies of this fungus in the workers’ blood samples, together with the clinical causes of the airway symptoms, indicate an aetiological relationship between airway symptoms and heavy exposure to this fungus (Dahl et al. 1994).
- Micro-organisms (bacteria and fungi) and endotoxins are potential agents of occupational hazard in a potato processing plant (Dutkiewicz 1994). The presence of precipitins to microbial antigens was significantly correlated with the occurrence of the work-related respiratory and general symptoms that were found in 45.9% of the examined workers.
- Museum and library personnel are exposed to moulds (e.g., Aspergillus, Pencillium) which, under certain conditions, contaminate books (Kolmodin-Hedman et al. 1986). Symptoms experienced are attacks of fever, chill, nausea and cough.
- Ocular infections can result from the use of industrial microscope eyepieces on multiple shifts. Staphylococcus aureus has been identified among the micro-organism cultures (Olcerst 1987).
Prevention
An understanding of the principles of epidemiology and the spread of infectious disease is essential in the methods used in the control of the causing organism.
Preliminary and periodic medical examinations of workers should be carried out in order to detect biological occupational diseases. There are general principles for conducting medical examinations in order to detect adverse health effects of workplace exposure, including biological hazards. Specific procedures are to be found elsewhere in this Encyclopaedia. For example, in Sweden the Farmers’ Federation initiated a programme of preventive occupational health services for farmers (Hoglund 1990). The main goal of the Farmers’ Preventive Health Service (FPHS) is to prevent work-related injuries and illnesses and to provide clinical services to farmers for occupational medical problems.
For some infectious disease outbreaks, appropriate preventive measures may be difficult to put in place until the disease is identified. Outbreaks of the viral Crimean-Congo haemorrhagic fever (CCHF) which demonstrated this problem were reported among hospital staff in the United Arab Emirates (Dubai), Pakistan and South Africa (Van Eeden et al. 1985).
Table 3. Animals as a source of occupational hazards
|
Infection |
Infection1 |
Allergic |
Toxin |
Vector2 |
|
|
Invertebrates other than arthropods |
|||||
|
Protozoa |
x |
x |
|||
|
Sponges |
x |
||||
|
Coelenterates |
x |
||||
|
Flatworms |
x |
x |
|||
|
Roundworms |
x |
x |
x |
||
|
Bryozoa |
x |
||||
|
Sea-squirts |
x |
||||
|
Arthropods |
|||||
|
Crustaceans |
x |
||||
|
Arachnids |
|||||
|
Spiders |
x(B)3 |
||||
|
Mites |
x |
x |
x(B) |
x |
|
|
Ticks |
x(B) |
x |
|||
|
Insects |
|||||
|
Cockroaches |
x |
||||
|
Beetles |
x |
||||
|
Moths |
x |
x |
|||
|
Flies |
x(B) |
x |
|||
|
Bees |
x |
x(B) |
|||
|
Vertebrates |
|||||
|
Fish |
x |
x(B) |
|||
|
Amphibians |
x |
||||
|
Reptiles |
x(B) |
||||
|
Birds |
x |
||||
|
Mammals |
x |
||||
1 Infection-zoonosis: Causes infection or invasion contracted from vertebrate animals.
2 Vector of pathogenic viruses, bacteria or parasites.
3 Toxic B produces toxin or venom transmitted by bite or sting.
Vertebrates: Snakes and Lizards
In hot and temperate zones, snakebites may constitute a definite hazard for certain categories of workers: agricultural workers, woodcutters, building and civil engineering workers, fishermen, mushroom gatherers, snake charmers, zoo attendants and laboratory workers employed in the preparation of antivenom serums. The vast majority of snakes are harmless to humans, although a number are capable of inflicting serious injury with their venomous bites; dangerous species are found among both the terrestrial snakes (Colubridae and Viperidae) and aquatic snakes (Hydrophiidae) (Rioux and Juminer 1983).
According to the World Health Organization (WHO 1995), snakebites are estimated to cause 30,000 deaths per year in Asia and about 1,000 deaths each in Africa and South America. More detailed statistics are available from certain countries. Over 63,000 snakebites and scorpion stings with over 300 deaths are reported yearly in Mexico. In Brazil, about 20,000 snakebites and 7,000 to 8,000 scorpion stings occur annually, with a case-fatality rate of 1.5% for snake bites and between 0.3% and 1% for scorpion stings. A study in Ouagadougou, Burkina Faso, showed 7.5 snakebites per 100,000 population in peri-urban areas and up to over 69 per 100,000 in more remote areas, where case-fatality rates reached 3%.
Snakebites are a problem also in developed parts of the world. Each year about 45,000 snakebites are reported in the United States, where the availability of health care has reduced the number of deaths to 9–15 per year. In Australia, where some of the world’s most venomous snakes exist, the annual number of snakebites is estimated at between 300 and 500, with an average of two deaths.
Environmental changes, particularly deforestation, may have caused the disappearance of many snake species in Brazil. However, the number of reported cases of snakebites did not decrease as other and sometimes more dangerous species proliferated in some of the deforested areas (WHO 1995).
Sauria (lizards)
There are only two species of venomous lizards, both members of the genus Heloderma: H. suspectum (Gila monster) and H. horridum (beaded lizard). Venom similar to that of the Viperidae penetrates wounds inflicted by the anterior curved teeth, but bites in humans are uncommon and recovery is generally rapid (Rioux and Juminer 1983).
Prevention
Snakes do not usually attack humans unless they feel menaced, are disturbed or are trodden on. In regions infested with venomous snakes, workers should wear foot and leg protection and be provided with monovalent or polyvalent antivenom serum. It is recommended that persons working in a danger area at a distance of over half-an-hour’s travel from the nearest first-aid post should carry an antivenom kit containing a sterilized syringe. However, it should be explained to workers that bites even from the most venomous snakes are seldom fatal, since the amount of venom injected is usually small. Certain snake charmers achieve immunization by repeated injections of venom, but no scientific method of human immunization has yet been developed (Rioux and Juminer 1983).
International Standards and Biological Hazards
Many national occupational standards include biological hazards in their definition of harmful or toxic substances. However, in most regulatory frameworks, biological hazards are chiefly restricted to micro-organisms or infectious agents. Several US Occupational Safety and Health Administration (OSHA) regulations include provisions on biological hazards. The most specific are those concerning hepatitis B vaccine vaccination and blood-borne pathogens; biological hazards are also covered in regulations with a broader scope (e.g., those on hazard communication, the specifications for accident prevention signs and tags, and the regulation on training curriculum guidelines).
Although not the subject of specific regulations, the recognition and avoidance of hazards relating to animal, insect or plant life is addressed in other OSHA regulations concerning specific work settings—for example, the regulation on telecommunications, the one on temporary labour camps and the one on pulpwood logging (the latter including guidelines concerning snake-bite first-aid kits).One of the most comprehensive standards regulating biological hazards in the workplace is European Directive No. 90/679. It defines biological agents as “micro-organisms, including those which have been genetically modified, cell cultures and human endoparasites, which may be able to provoke any infection, allergy or toxicity,” and classifies biological agents into four groups according to their level of risk of infection. The Directive covers the determination and assessment of risks and employers’ obligations in terms of the replacement or reduction of risks (through engineering control measures, industrial hygiene, collective and personal protection measures and so on), information (for workers, workers’ representatives and the competent authorities), health surveillance, vaccination and record-keeping. The Annexes provide detailed information on containment measures for different “containment levels” according to the nature of the activities, the assessment of risk to workers and the nature of the biological agent concerned.
Aquatic Animals
D. Zannini*
* Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Aquatic animals dangerous to humans are to be found among practically all of the divisions (phyla). Workers may come into contact with these animals in the course of various activities including surface and underwater fishing, the installation and handling of equipment in connection with the exploitation of petroleum under the sea, underwater construction, and scientific research, and thus be exposed to health risks. Most of the dangerous species inhabit warm or temperate waters.
Characteristics and Behaviour
Porifera. The common sponge belongs to this phylum. Fishermen who handle sponges, including helmet and scuba divers, and other underwater swimmers, may contract contact dermatitis with skin irritation, vesicles or blisters. The “sponge diver’s sickness” of the Mediterranean region is caused by the tentacles of a small coelenterate (Sagartia rosea) that is a parasite of the sponge. A form of dermatitis known as “red moss” is found among North American oyster fishers resulting from contact with a scarlet sponge found on the shell of the oysters. Cases of type 4 allergy have been reported. The poison secreted by the sponge Suberitus ficus contains histamine and antibiotic substances.
Coelenterata. These are represented by many families of the class known as Hydrozoa, which includes the Millepora or coral (stinging coral, fire coral), the Physalia (Physalia physalis, sea wasp, Portuguese man-of-war), the Scyphozoa (jellyfish) and the Actiniaria (stinging anemone), all of which are found in all parts of the ocean. Common to all these animals is their ability to produce an urticaria by the injection of a strong poison that is retained in a special cell (the cnidoblast) containing a hollow thread, which explodes outwards when the tentacle is touched, and penetrates the person’s skin. The various substances contained in this structure are responsible for such symptoms as severe itching, congestion of the liver, pain, and depression of the central nervous system; these substances have been identified as thalassium, congestine, equinotoxin (which contains 5-hydroxytryptamine and tetramine) and hypnotoxin, respectively. Effects on the individual depend upon the extent of the contact made with the tentacles and hence on the number of microscopic punctures, which may amount to many thousands, up to the point where they may cause the death of the victim within a few minutes. In view of the fact that these animals are dispersed so widely throughout the world, many incidents of this nature occur but the number of fatalities is relatively small. Effects on the skin are characterized by intense itching and the formation of papules having a bright red, mottled appearance, developing into pustules and ulceration. Intense pain similar to electric shock may be felt. Other symptoms include difficulty in breathing, generalized anxiety and cardiac upset, collapse, nausea and vomiting, loss of consciousness, and primary shock.
Echinoderma. This group includes the starfishes and sea urchins, both of which possess poisonous organs (pedicellariae), but are not dangerous to humans. The spine of the sea urchin can penetrate the skin, leaving a fragment deeply imbedded; this can give rise to a secondary infection followed by pustules and persistent granuloma, which can be very troublesome if the wounds are close to tendons or ligaments. Among the sea urchins, only the Acanthaster planci seems to have a poisonous spine, which can give rise to general disturbances such as vomiting, paralysis and numbness.
Mollusca. Among the animals belonging to this phylum are the cone shells, and these can be dangerous. They live on a sandy sea-bottom and appear to have a poisonous structure consisting of a radula with needle-like teeth, which can strike at the victim if the shell is handled incautiously with the bare hand. The poison acts on the neuromuscular and central nervous systems. Penetration of the skin by the point of a tooth is followed by temporary ischaemia, cyanosis, numbness, pain, and paraesthesia as the poison spreads gradually through the body. Subsequent effects include paralysis of the voluntary muscles, lack of coordination, double vision and general confusion. Death can follow as a result of respiratory paralysis and circulatory collapse. Some 30 cases have been reported, of which 8 were fatal.
Platyhelminthes. These include the Eirythoe complanata and the Hermodice caruncolata, known as “bristle worms”. They are covered with numerous bristle-like appendages, or setae, containing a poison (nereistotoxin) with a neurotoxic and local irritant effect.
Polyzoa (Bryozoa). These are made up of a group of animals which form plant-like colonies resembling gelatinous moss, which frequently encrust rocks or shells. One variety, known as Alcyonidium, can cause an urticarious dermatitis on the arms and face of fishermen who have to clean this moss off their nets. It can also give rise to an allergic eczema.
Selachiis (Chondrichthyes). Animals belonging to this phylum include the sharks and sting-rays. The sharks live in fairly shallow water, where they search for prey and may attack people. Many varieties have one or two large, poisonous spines in front of the dorsal fin, which contain a weak poison that has not been identified; these can cause a wound giving rise to immediate and intense pain with reddening of the flesh, swelling and oedema. A far greater danger from these animals is their bite, which, because of several rows of sharp pointed teeth, causes severe laceration and tearing of the flesh leading to immediate shock, acute anaemia and drowning of the victim. The danger that sharks represent is a much-discussed subject, each variety seeming to be particularly aggressive. There seems no doubt that their behaviour is unpredictable, although it is said that they are attracted by movement and by the light colour of a swimmer, as well as by blood and by vibrations resulting from a fish or other prey that has just been caught. Sting-rays have large, flat bodies with a long tail having one or more strong spines or saws, which can be poisonous. The poison contains serotonine, 5-nucleotidase and phosphodiesterase, and can cause generalized vasoconstriction and cardio-respiratory arrest. Sting-rays live in the sandy regions of coastal waters, where they are well hidden, making it easy for bathers to step on one without seeing it. The ray reacts by bringing over its tail with the projecting spine, impaling the spike keep into the flesh of the victim. This may cause piercing wounds in a limb or even penetration of an internal organ such as the peritoneum, lung, heart or liver, particularly in the case of children. The wound can also give rise to great pain, swelling, lymphatic oedema and various general symptoms such as primary shock and cardio-circulatory collapse. Injury to an internal organ may lead to death in a few hours. Sting-ray incidents are among the most frequent, there being some 750 every year in the United States alone. They can also be dangerous for fishermen, who should immediately cut off the tail as soon as the fish is brought aboard. Various species of rays such as the torpedo and the narcine possess electric organs on their back, which, when stimulated by touch alone, can produce electric shocks ranging from 8 up to 220 volts; this may be enough to stun and temporarily disable the victim, but recovery is usually without complications.
Osteichthyes. Many fishes of this phylum have dorsal, pectoral, caudal and anal spines which are connected with a poison system and whose primary purpose is defence. If the fish is disturbed or stepped upon or handled by a fisherman, it will erect the spines, which can pierce the skin and inject the poison. Not infrequently they will attack a diver seeking fish, or if they are disturbed by accidental contact. Numerous incidents of this kind are reported because of the widespread distribution of fish of this phylum, which includes the catfish, which are also found in fresh water (South America, West Africa and the Great Lakes), the scorpion fish (Scorpaenidae), the weever fish (Trachinus), the toadfish, the surgeon fish and others. Wounds from these fishes are generally painful, particularly in the case of the catfish and the weever fish, causing reddening or pallor, swelling, cyanosis, numbness, lymphatic oedema and haemorrhagic suffusion in the surrounding flesh. There is a possibility of gangrene or phlegmonous infection and peripheral neuritis on the same side as the wound. Other symptoms include faintness, nausea, collapse, primary shock, asthma and loss of consciousness. They all represent a serious danger for underwater workers. A neurotoxic and haemotoxic poison has been identified in the catfish, and in the case of the weever fish a number of substances have been isolated such as 5-hydroxytryptamine, histamine and catecholamine. Some catfishes and stargazers that live in fresh water, as well as the electric eel (Electrophorus), have electric organs (see under Selachii above).
Hydrophiidae. This group (sea snakes) is to be found mostly in the seas around Indonesia and Malaysia; some 50 species have been reported, including Pelaniis platurus, Enhydrina schistosa and Hydrus platurus. The venom of these snakes is very similar to that of the cobra, but is 20 to 50 times as poisonous; it is made up of a basic protein of low molecular weight (erubotoxin) which affects the neuromuscular junction blocking the acetylcholine and provoking myolysis. Fortunately sea snakes are generally docile and bite only when stepped on, squeezed or dealt a hard blow; furthermore, they inject little or no venom from their teeth. Fishermen are among those most exposed to this hazard and account for 90% of all reported incidents, which result either from stepping on the snake on the sea bottom or from encountering them among their catch. Snakes are probably responsible for thousands of the occupational accidents attributed to aquatic animals, but few of these are serious, while only a small percentage of the serious accidents turn out to be fatal. Symptoms are mostly slight and not painful. Effects are usually felt within two hours, starting with muscular pain, difficulty with neck movement, lack of dexterity, and trismus, and sometimes including nausea and vomiting. Within a few hours myoglobinuria (the presence of complex proteins in urine) will be seen. Death can ensue from paralysis of the respiratory muscles, from renal insufficiency due to tubular necrosis, or from cardiac arrest due to hyperkalaemia.
Prevention
Every effort should be made to avoid all contact with the spines of these animals when they are being handled, unless strong gloves are worn, and the greatest care should be taken when wading or walking on a sandy sea bottom. The wet suit worn by skin divers offers protection against the jellyfish and the various Coelenterata as well as against snakebite. The more dangerous and aggressive animals should not be molested, and zones where there are jellyfish should be avoided, as they are difficult to see. If a sea snake is caught on a line, the line should be cut and the snake allowed to go. If sharks are encountered, there are a number of principles that should be observed. People should keep their feet and legs out of the water, and the boat should be gently brought to shore and kept still; a swimmer should not stay in the water with a dying fish or with one that is bleeding; a shark’s attention should not be attracted by the use of bright colours, jewellery, or by making a noise or explosion, by showing a bright light, or by waving the hands towards it. A diver should never dive alone.
Terrestrial Venomous Animals
J.A. Rioux and B. Juminer*
*Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety.
Annually millions of scorpion stings and anaphylactic reactions to insect stings may occur worldwide, causing tens of thousands of deaths in humans each year. Between 30,000 and 45,000 cases of scorpion stings are reported annually in Tunisia, causing between 35 and 100 deaths, mostly among children. Envenomation (toxic effects) is an occupational hazard for populations involved in agriculture and forestry in these regions.
Among the animals that can inflict injury on humans by the action of their venom are invertebrates, such as Arachnida (spiders, scorpions and sun spiders), Acarina (ticks and mites), Chilopoda (centipedes) and Hexapoda (bees, wasps, butterflies, and midges).
Invertebrates
Arachnida (spiders—Aranea)
All species are venomous, but in practice only a few types produce injury in humans. Spider poisoning may be of two types:
- Cutaneous poisoning, in which the bite is followed after a few hours by oedema centred around a cyanotic mark, and then by a blister; extensive local necrosis may ensue, and healing may be slow and difficult in cases of bites from spiders of the Lycosa genus (e.g., the tarantula).
- Nerve poisoning due to the exclusively neurotoxic venom of the mygales (Latrodectus ctenus), which produces serious injury, with early onset, tetany, tremors, paralysis of the extremities and, possibly, fatal shock; this type of poisoning is relatively common amongst forestry and agricultural workers and is particularly severe in children: in the Amazonas, the venom of the “black widow” spider (Latrodectus mactans) is used for poison arrows.
Prevention. In areas where there is a danger of venomous spiders, sleeping accommodation should be provided with mosquito nets and workers should be equipped with footwear and working clothes that give adequate protection.
Scorpions (Scorpionida)
These arachnids have a sharp poison claw on the end of the abdomen with which they can inflict a painful sting, the seriousness of which varies according to the species, the amount of venom injected and the season (the most dangerous season being at the end of the scorpions’ hibernation period). In the Mediterranean region, South America and Mexico, the scorpion is responsible for more deaths than poisonous snakes. Many species are nocturnal and are less aggressive during the day. The most dangerous species (Buthidae) are found in arid and tropical regions; their venom is neurotropic and highly toxic. In all cases, the scorpion sting immediately produces intense local signs (acute pain, inflammation) followed by general manifestations such as tendency to fainting, salivation, sneezing, lachrymation and diarrhoea. The course in young children is often fatal. The most dangerous species are found amongst the genera Androctonus (sub-Saharan Africa), Centrurus (Mexico) and Tituus (Brazil). The scorpion will not spontaneously attack humans, and stings only when it considers itself endangered, as when trapped in a dark corner or when boots or clothes in which it has taken refuge are shaken or put on. Scorpions are highly sensitive to halogenated pesticides (e.g., DDT).
Sun spiders (Solpugida)
This order of arachnid is found chiefly in steppe and sub-desert zones such as the Sahara, Andes, Asia Minor, Mexico and Texas, and is non-venomous; nevertheless, sun spiders are extremely aggressive, may be as large as 10 cm across and have a fearsome appearance. In exceptional cases, the wounds they inflict may prove serious due to their multiplicity. Solpugids are nocturnal predators and may attack a sleeping individual.
Ticks and mites (Acarina)
Ticks are blood-sucking arachnids at all stages of their life cycle, and the “saliva” they inject through their feeding organs may have a toxic effect. Poisoning may be severe, although mainly in children (tick paralysis), and may be accompanied by reflex suppression. In exceptional cases death may ensue due to bulbar paralysis (in particular where a tick has attached itself to the scalp). Mites are haematophagic only at the larval stage, and their bite produces pruritic inflammation of the skin. The incidence of mite bites is high in tropical regions.
Treatment. Ticks should be detached after they are anaesthetized with a drop of benzene, ethyl ether or xylene. Prevention is based on the use of organophosphorus pesticide pest repellents.
Centipedes (Chilopoda)
Centipedes differ from millipedes (Diplopoda) in that they have only one pair of legs per body segment and that the appendages of the first body segment are poison fangs. The most dangerous species are encountered in the Philippines. Centipede venom has only a localized effect (painful oedema).
Treatment. Bites should be treated with topical applications of dilute ammonia, permanganate or hypochlorite lotions. Antihistamines may also be administered.
Insects (Hexapoda)
Insects may inject venom via the mouthparts (Simuliidae—black flies, Culicidae—mosquitoes, Phlebotomus—sandflies) or via the sting (bees, wasps, hornets, carnivorous ants). They may cause rash with their hairs (caterpillars, butterflies), or they may produce blisters by their haemolymph (Cantharidae—blister flies and Staphylinidae—rove beetles). Black fly bites produce necrotic lesions, sometimes with general disorders; mosquito bites produce diffuse pruriginous lesions. The stings of Hymenoptera (bees, etc.) produce intense local pain with erythema, oedema and, sometimes, necrosis. General accidents may result from sensitization or multiplicity of stings (shivering, nausea, dyspnoea, chilling of the extremities). Stings on the face or the tongue are particularly serious and may cause death by asphyxiation due to glottal oedema. Caterpillars and butterflies may cause generalized pruriginous skin lesions of an urticarial or oedematous type (Quincke’s oedema), sometimes accompanied by conjunctivitis. Superimposed infection is not infrequent. The venom from blister flies produces vesicular or bullous skin lesions (Poederus). There is also the danger of visceral complications (toxic nephritis). Certain insects such as Hymenoptera and caterpillars are found in all parts of the world; other suborders are more localized, however. Dangerous butterflies are found mainly in Guyana and the Central African Republic; blister flies are found in Japan, South America and Kenya; black flies live in the intertropical regions and in central Europe; sandflies are found in the Middle East.
Prevention. First level prevention includes mosquito nets and repellent and/or insecticide application. Workers who are severely exposed to insect bites can be desensitized in cases of allergy by the administration of increasingly large doses of insect body extract.
Clinical Features of Snakebite
David A. Warrell*
* Adapted from The Oxford Textbook of Medicine, edited by DJ Weatherall, JGG Ledingham and DA Warrell (2nd edition, 1987), pp. 6.66-6.77. By permission of Oxford University Press.
Clinical Features
A proportion of patients bitten by venomous snakes (60%), depending on the species, will develop minimal or no signs of toxic symptoms (envenoming) despite having puncture marks which indicate that the snake’s fangs have penetrated the skin.
Fear and effects of treatment, as well as the snake’s venom, contribute to the symptoms and signs. Even patients who are not envenomed may feel flushed, dizzy and breathless, with constriction of the chest, palpitations, sweating and acroparaesthesiae. Tight tourniquets may produce congested and ischaemic limbs; local incisions at the site of the bite may cause bleeding and sensory loss; and herbal medicines often induce vomiting.
The earliest symptoms directly attributable to the bite are local pain and bleeding from the fang punctures, followed by pain, tenderness, swelling and bruising extending up the limb, lymphangitis and tender enlargement of regional lymph nodes. Early syncope, vomiting, colic, diarrhoea, angio-oedema and wheezing may occur in patients bitten by European Vipera, Daboia russelii, Bothrops sp, Australian Elapids and Atractaspis engaddensis. Nausea and vomiting are common symptoms of severe envenoming.
Types of bites
Colubridae (back-fanged snakes such as Dispholidus typus, Thelotornis sp, Rhabdophis sp, Philodryas sp)
There is local swelling, bleeding from the fang marks and sometimes (Rhabophis tigrinus) fainting. Later vomiting, colicky abdominal pain and headache, and widespread systemic bleeding with extensive ecchymoses (bruising), incoagulable blood, intravascular haemolysis and kidney failure may develop. Envenoming may develop slowly over several days.
Atractaspididae (burrowing asps, Natal black snake)
Local effects include pain, swelling, blistering, necrosis and tender enlargement of local lymph nodes. Violent gastro-intestinal symptoms (nausea, vomiting and diarrhoea), anaphylaxis (dyspnoea, respiratory failure, shock) and ECG changes (a-v block, ST, T-wave changes) have been described in patients envenomed by A. engaddensis.
Elapidae (cobras, kraits, mambas, coral snakesand Australian venomous snakes)
Bites by kraits, mambas, coral snakes and some cobras (e.g., Naja haje and N. nivea) produce minimal local effects, whereas bites by African spitting cobras (N. nigricollis, N. mossambica, etc.) and Asian cobras (N. naja, N. kaouthia, N. sumatrana, etc.) cause tender local swelling which may be extensive, blistering and superficial necrosis.
Early symptoms of neurotoxicity before there are objective neurological signs include vomiting, “heaviness” of the eyelids, blurred vision, fasciculations, paraesthesiae around the mouth, hyperacusis, headache, dizziness, vertigo, hypersalivation, congested conjunctivae and “gooseflesh”. Paralysis starts as ptosis and external ophthalmoplegia appearing as early as 15 minutes after the bite, but sometimes delayed for ten hours or more. Later the face, palate, jaws, tongue, vocal cords, neck muscles and muscles of deglutition become progressively paralysed. Respiratory failure may be precipitated by upper airway obstruction at this stage, or later after paralysis of intercostal muscles, diaphragm and accessory muscles of respiration. Neurotoxic effects are completely reversible, either acutely in response to antivenom or anticholinesterases (e.g., following bites by Asian cobras, some Latin American coral snakes—Micrurus, and Australian death adders—Acanthophis) or they may wear off spontaneously in one to seven days.
Envenoming by Australian snakes causes early vomiting, headache and syncopal attacks, neurotoxicity, haemostatic disturbances and, with some species, ECG changes, generalized rhabdomyolysis and kidney failure. Painful enlargement of regional lymph nodes suggests impending systemic envenoming, but local signs are usually absent or mild except after bites by Pseudechis sp.
Venom ophthalmia caused by “spitting” elapids
Patients “spat” at by spitting elapids experience intense pain in the eye, conjunctivitis, blepharospasm, palpebral oedema and leucorrhoea. Corneal erosions are detectable in more than half the patients spat at by N. nigricollis. Rarely, venom is absorbed into the anterior chamber, causing hypopyon and anterior uveitis. Secondary infection of corneal abrasions may lead to permanent blinding opacities or panophthalmitis.
Viperidae (vipers, adders, rattlesnakes, lance-headed vipers, moccasins and pit vipers)
Local envenoming is relatively severe. Swelling may become detectable within 15 minutes but is sometimes delayed for several hours. It spreads rapidly and may involve the whole limb and adjacent trunk. There is associated pain and tenderness in regional lymph nodes. Bruising, blistering and necrosis may appear during the next few days. Necrosis is particularly frequent and severe following bites by some rattlesnakes, lance-headed vipers (genus Bothrops), Asian pit vipers and African vipers (genera Echis and Bitis). When the envenomed tissue is contained in a tight fascial compartment such as the pulp space of the fingers or toes or the anterior tibial compartment, ischaemia may result. If there is no swelling two hours after a viper bite it is usually safe to assume that there has been no envenoming. However, fatal envenoming by a few species can occur in the absence of local signs (e.g., Crotalus durissus terrificus, C. scutulatus and Burmese Russell’s viper).
Blood pressure abnormalities are a consistent feature of envenoming by Viperidae. Persistent bleeding from fang puncture wounds, venepuncture or injection sites, other new and partially healed wounds and post partum, suggests that the blood is incoagulable. Spontaneous systemic haemorrhage is most often detected in the gums, but may also be seen as epistaxis, haematemesis, cutaneous ecchymoses, haemoptysis, subconjunctival, retroperitoneal and intracranial haemorrhages. Patients envenomed by the Burmese Russell’s viper may bleed into the anterior pituitary gland (Sheehan’s syndrome).
Hypotension and shock are common in patients bitten by some of the North American rattlesnakes (e.g., C. adamanteus, C. atrox and C. scutulatus), Bothrops, Daboia and Vipera species (e.g., V. palaestinae and V. berus). The central venous pressure is usually low and the pulse rate rapid, suggesting hypovolaemia, for which the usual cause is extravasation of fluid into the bitten limb. Patients envenomed by Burmese Russell’s vipers show evidence of generally increased vascular permeability. Direct involvement of the heart muscle is suggested by an abnormal ECG or cardiac arrhythmia. Patients envenomed by some species of the genera Vipera and Bothrops may experience transient recurrent fainting attacks associated with features of an autopharmacological or anaphylactic reaction such as vomiting, sweating, colic, diarrhoea, shock and angio-oedema, appearing as early as five minutes or as late as many hours after the bite.
Renal (kidney) failure is the major cause of death in patients envenomed by Russell’s vipers who may become oliguric within a few hours of the bite and have loin pain suggesting renal ischaemia. Renal failure is also a feature of envenoming by Bothrops species and C. d. terrificus.
Neurotoxicity, resembling that seen in patients bitten by Elapidae, is seen after bites by C. d. terrificus, Gloydius blomhoffii, Bitis atropos and Sri Lankan D. russelii pulchella. There may be evidence of generalized rhabdomyolysis. Progression to respiratory or generalized paralysis is unusual.
Laboratory Investigations
The peripheral neutrophil count is raised to 20,000 cells per microlitre or more in severely envenomed patients. Initial haemo-concentration, resulting from extravasation of plasma (Crotalus species and Burmese D. russelii), is followed by anaemia caused by bleeding or, more rarely, haemolysis. Thrombocytopenia is common following bites by pit vipers (e.g., C. rhodostoma, Crotalus viridis helleri) and some Viperidae (e.g., Bitis arietans and D. russelii), but is unusual after bites by Echis species. A useful test for venom-induced defibrin(ogen)ation is the simple whole blood clotting test. A few millilitres of venous blood is placed in a new, clean, dry, glass test tube, left undisturbed for 20 minutes at ambient temperature, and then tipped to see if it has clotted or not. Incoagulable blood indicates systemic envenoming and may be diagnostic of a particular species (for example Echis species in Africa). Patients with generalized rhabdomyolysis show a steep rise in serum creatine kinase, myoglobin and potassium. Black or brown urine suggests generalized rhabdomyolysis or intravascular haemolysis. Concentrations of serum enzymes such as creatine phosphokinase and aspartate aminotransferase are moderately raised in patients with severe local envenoming, probably because of local muscle damage at the site of the bite. Urine should be examined for blood/haemoglobin, myoglobin and protein and for microscopic haematuria and red cell casts.
Treatment
First aid
Patients should be moved to the nearest medical facility as quickly and comfortably as possible, avoiding movement of the bitten limb, which should be immobilized with a splint or sling.
Most traditional first-aid methods are potentially harmful and should not be used. Local incisions and suction may introduce infection, damage tissues and cause persistent bleeding, and are unlikely to remove much venom from the wound. The vacuum extractor method is of unproven benefit in human patients and could damage soft tissues. Potassium permanganate and cryotherapy potentiate local necrosis. Electric shock is potentially dangerous and has not proved beneficial. Tourniquets and compression bands can cause gangrene, fibrinolysis, peripheral nerve palsies and increased local envenoming in the occluded limb.
The pressure immobilization method involves firm but not tight bandaging of the entire bitten limb with a crepe bandage 4-5 m long by 10 cm wide starting over the site of the bite and incorporating a splint. In animals, this method was effective in preventing systemic uptake of Australian elapid and other venoms, but in humans it has not been subjected to clinical trials. Pressure immobilization is recommended for bites by snakes with neurotoxic venoms (e.g., Elapidae, Hydrophiidae) but not when local swelling and necrosis may be a problem (e.g., Viperidae).
Pursuing, capturing or killing the snake should not be encouraged, but if the snake has been killed already it should be taken with the patient to hospital. It must not be touched with bare hands, as reflex bites may occur even after the snake is apparently dead.
Patients being transported to hospital should be laid on their side to prevent aspiration of vomit. Persistent vomiting is treated with chlorpromazine by intravenous injection (25 to 50 mg for adults, 1 mg/kg body weight for children). Syncope, shock, angio-oedema and other anaphylactic (autopharmacological) symptoms are treated with 0.1% adrenaline by subcutaneous injection (0.5 ml for adults, 0.01 ml/kg body weight for children), and an antihistamine such as chlorpheniramine maleate is given by slow intravenous injection (10 mg for adults, 0.2 mg/kg body weight for children). Patients with incoagulable blood develop large haematomas after intramuscular and subcutaneous injections; the intravenous route should be used whenever possible. Respiratory distress and cyanosis are treated by establishing an airway, giving oxygen and, if necessary, assisted ventilation. If the patient is unconscious and no femoral or carotid pulses can be detected, cardiopulmonary resuscitation (CPR) should be started immediately.
Hospital treatment
Clinical assessment
In most cases of snakebite there are uncertainties about the species responsible and the quantity and composition of venom injected. Ideally, therefore, patients should be admitted to hospital for at least 24 hours of observation. Local swelling is usually detectable within 15 minutes of significant pit viper envenoming and within two hours of envenoming by most other snakes. Bites by kraits (Bungarus), coral snakes (Micrurus, Micruroides), some other elapids and sea snakes may cause no local envenoming. Fang marks are sometimes invisible. Pain and tender enlargement of lymph nodes draining the bitten area is an early sign of envenoming by Viperidae, some Elapidae and Australasian elapids. All the patient’s tooth sockets should be examined meticulously, as this is usually the first site at which spontaneous bleeding can be detected clinically; other common sites are nose, eyes (conjunctivae), skin and gastro-intestinal tract. Bleeding from venipuncture sites and other wounds implies incoagulable blood. Hypotension and shock are important signs of hypovolaemia or cardiotoxicity, seen particularly in patients bitten by North American rattlesnakes and some Viperinae (e.g., V berus, D russelii, V palaestinae). Ptosis (e.g., drooping of the eyelid) is the earliest sign of neurotoxic envenoming. Respiratory muscle power should be assessed objectively—for example, by measuring vital capacity. Trismus, generalized muscle tenderness and brownish-black urine suggests rhabdomyolysis (Hydrophiidae). If a procoagulant venom is suspected, coagulability of whole blood should be checked at the bedside using the 20-minute whole blood clotting test.
Blood pressure, pulse rate, respiratory rate, level of consciousness, presence/absence of ptosis, extent of local swelling and any new symptoms must be recorded at frequent intervals.
Antivenom treatment
The most important decision is whether or not to give antivenom, as this is the only specific antidote. There is now convincing evidence that in patients with severe envenoming, the benefits of this treatment far outweigh the risk of antivenom reactions (see below).
General indications for antivenom
Antivenom is indicated if there are signs of systemic envenoming such as:
- haemostatic abnormalities such as spontaneous systemic bleeding, incoagulable blood or profound thrombocytopenia (50/l x 10-9)
- neurotoxicity
- hypotension and shock, abnormal ECG or other evidence of cardiovascular dysfunction
- impaired consciousness of any cause
- generalized rhabdomyolysis.
Supporting evidence of severe envenoming is a neutrophil leucocytosis, elevated serum enzymes such as creatine kinase and aminotransferases, haemoconcentration, severe anaemia, myoglobinuria, haemoglobinuria, methaemoglobinuria, hypoxaemia or acidosis.
In the absence of systemic envenoming, local swelling involving more than half the bitten limb, extensive blistering or bruising, bites on digits and rapid progression of swelling are indications for antivenom, especially in patients bitten by species whose venoms are known to cause local necrosis (e.g., Viperidae, Asian cobras and African spitting cobras).
Special indications for antivenom
Some developed countries have the financial and technical resources for a wider range of indications:
United States and Canada: After bites by the most dangerous rattlesnakes (C. atrox, C. adamanteus, C. viridis, C. horridus and C. scutulatus) early antivenom therapy is recommended before systemic envenoming is evident. Rapid spread of local swelling is considered to be an indication for antivenom, as is immediate pain or any other symptom or sign of envenoming after bites by coral snakes (Micruroides euryxanthus and Micrurus fulvius).
Australia: Antivenom is recommended for patients with proved or suspected snakebite if there are tender regional lymph nodes or other evidence of systemic spread of venom, and in anyone effectively bitten by an identified highly venomous species.
Europe: (Adder: Vipera berus and other European Vipera): Antivenom is indicated to prevent morbidity and reduce the length of convalescence in patients with moderately severe envenoming as well as to save the lives of severely envenomed patients. Indications are:
- fall in blood pressure (systolic to less than 80 mmHg, or by more than 50 mmHg from the normal or admission value) with or without signs of shock
- other signs of systemic envenoming (see above), including spontaneous bleeding, coagulopathy, pulmonary oedema or haemorrhage (shown by chest radiograph), ECG abnormalities and a definite peripheral leucocytosis (more than 15,000/ μl) and elevated serum creatine kinase
- severe local envenoming—swelling of more than half the bitten limb developing within 48 hours of the bite—even in the absence of systemic envenoming
- in adults, swelling extending beyond the wrist after bites on the hand or beyond the ankle after bites on the foot within four hours of the bite.
Patients bitten by European Vipera who show any evidence of envenoming should be admitted to hospital for observation for at least 24 hours. Antivenom should be given whenever there is evidence of systemic envenoming—(1) or (2) above—even if its appearance is delayed for several days after the bite.
Prediction of antivenom reactions
It is important to realize that most antivenom reactions are not caused by acquired Type I, IgE-mediated hypersensitivity but by complement activation by IgG aggregates or Fc fragments. Skin and conjunctival tests do not predict early (anaphylactic) or late (serum sickness type) antivenom reactions but delay treatment and may sensitize the patient. They should not be used.
Contraindications to antivenom
Patients with a history of reactions to equine antiserum suffer an increased incidence and severity of reactions when given equine antivenom. Atopic subjects have no increased risk of reactions, but if they develop a reaction it is likely to be severe. In such cases, reactions may be prevented or ameliorated by pretreatment with subcutaneous adrenaline, antihistamine and hydrocortisone, or by continuous intravenous infusion of adrenaline during antivenom administration. Rapid desensitization is not recommended.
Selection and administration of antivenom
Antivenom should be given only if its stated range of specificity includes the species responsible for the bite. Opaque solutions should be discarded, as precipitation of protein indicates loss of activity and increased risk of reactions. Monospecific (monovalent) antivenom is ideal if the biting species is known. Polyspecific (polyvalent) antivenoms are used in many countries because it is difficult to identify the snake responsible. Polyspecific antivenoms may be just as effective as monospecific ones but contain less specific venom-neutralizing activity per unit weight of immunoglobulin. Apart from the venoms used for immunizing the animal in which the antivenom has been produced, other venoms may be covered by paraspecific neutralization (e.g., Hydrophiidae venoms by tiger snake—Notechis scutatus—antivenom).
Antivenom treatment is indicated as long as signs of systemic envenoming persist (i.e., for several days) but ideally it should be given as soon as these signs appear. The intravenous route is the most effective. Infusion of antivenom diluted in approximately 5 ml of isotonic fluid/kg body weight is easier to control than intravenous “push” injection of undiluted antivenom given at the rate of about 4 ml/min, but there is no difference in the incidence or severity of antivenom reactions in patients treated by these two methods.
Dose of antivenom
Manufacturers’ recommendations are based on mouse protection tests and may be misleading. Clinical trials are needed to establish appropriate starting doses of major antivenoms. In most countries the dose of antivenom is empirical. Children must be given the same dose as adults.
Response to antivenom
Marked symptomatic improvement may be seen soon after antivenom has been injected. In shocked patients, the blood pressure may rise and consciousness return (C. rhodostoma, V. berus, Bitis arietans). Neurotoxic signs may improve within 30 minutes (Acanthophis sp, N. kaouthia), but this usually takes several hours. Spontaneous systemic bleeding usually stops within 15 to 30 minutes, and blood coagulability is restored within six hours of antivenom, provided that a neutralizing dose has been given. More antivenom should be given if severe signs of envenoming persist after one to two hours or if blood coagulability is not restored within about six hours. Systemic envenoming may recur hours or days after an initially good response to antivenom. This is explained by continuing absorption of venom from the injection site and the clearance of antivenom from the bloodstream. The apparent serum half-lives of equine F(ab’)2 antivenoms in envenomed patients range from 26 to 95 hours. Envenomed patients should therefore be assessed daily for at least three or four days.
Antivenom reactions
- Early (anaphylactic) reactions develop within 10 to 180 minutes of starting antivenom in 3 to 84% of patients. The incidence increases with dose and decreases when more highly refined antivenom is used and administration is by intramuscular rather than intravenous injection. The symptoms are itching, urticaria, cough, nausea, vomiting, other manifestations of autonomic nervous system stimulation, fever, tachycardia, bronchospasm and shock. Very few of these reactions can be attributed to acquired Type I IgE-mediated hypersensitivity.
- Pyrogenic reactions result from contamination of the antivenom with endotoxins. Fever, rigors, vasodilatation and a fall in blood pressure develop one to two hours after treatment. In children, febrile convulsions may be precipitated.
- Late reactions of serum sickness (immune complex) type may develop 5 to 24 (mean 7) days after antivenom. The incidence of those reactions and the speed of their development increases with the dose of antivenom. Clinical features include fever, itching, urticaria, arthralgia (including the temporomandibular joint), lymphadenopathy, periarticular swellings, mononeuritis multiplex, albuminuria and, rarely, encephalopathy.
Treatment of antivenom reactions
Adrenaline (epinephrine) is the effective treatment for early reactions; 0.5 to 1.0 ml of 0.1% (1 in 1000, 1 mg/ml) is given by subcutaneous injection to adults (children 0.01 ml/kg) at the first signs of a reaction. The dose may be repeated if the reaction is not controlled. An antihistamine H1 antagonist, such as chlorpheniramine maleate (10 mg for adults, 0.2 mg/kg for children) should be given by intravenous injection to combat the effects of histamine release during the reaction. Pyrogenic reactions are treated by cooling the patient and giving antipyretics (paracetamol). Late reactions respond to an oral antihistamine such as chlorpheniramine (2 mg every six hours for adults, 0.25 mg/kg/day in divided doses for children) or to oral prednisolone (5 mg every six hours for five to seven days for adults, 0.7 mg/kg/day in divided doses for children).
Supportive treatment
Neurotoxic envenoming
Bulbar and respiratory paralysis may lead to death from aspiration, airway obstruction or respiratory failure. A clear airway must be maintained and, if respiratory distress develops, a cuffed endotracheal tube should be inserted or tracheostomy performed. Anticholinesterases have a variable but potentially useful effect in patients with neurotoxic envenoming, especially when post-synaptic neurotoxins are involved. The “Tensilon test” should be done in all cases of severe neurotoxic envenoming as with suspected myasthenia gravis. Atropine sulphate (0.6 mg for adults, 50 μg/kg body weight for children) is given by intravenous injection (to block muscarinic effects of acetylcholine) followed by an intravenous injection of edrophonium chloride (10 mg for adults, 0.25 mg/kg for children). Patients who respond convincingly can be maintained on neostigmine methyl sulphate (50 to 100 μg/kg body weight) and atropine, every four hours or by continuous infusion.
Hypotension and shock
If the jugular or central venous pressure is low or there is other clinical evidence of hypovolaemia or exsanguination, a plasma expander, preferably fresh whole blood or fresh frozen plasma, should be infused. If there is persistent or profound hypotension or evidence of increased capillary permeability (e.g., facial and conjunctival oedema, serous effusions, haemoconcentration, hypoalbuminaemia) a selective vasoconstrictor such as dopamine (starting dose 2.5 to 5 μg/kg body weight/min by infusion into a central vein) should be used.
Oliguria and renal failure
Urine output, serum creatinine, urea and electrolytes should be measured each day in patients with severe envenoming and in those bitten by species known to cause renal failure (e.g., D. russelii, C. d. terrificus, Bothrops species, sea snakes). If urine output drops below 400 ml in 24 hours, urethral and central venous catheters should be inserted. If urine flow fails to increase after cautious rehydration and diuretics (e.g., frusemide up to 1000 mg by intravenous infusion), dopamine (2.5 μg/kg body weight/min by intravenous infusion) should be tried and the patient placed on strict fluid balance. If these measures are ineffective, peritoneal or haemodialysis or haemofiltration are usually required.
Local infection at the site of the bite
Bites by some species (e.g., Bothrops sp, C. rhodostoma) seem particularly likely to be complicated by local infections caused by bacteria in the snake’s venom or on its fangs. These should be prevented with penicillin, chloramphenicol or erythromycin and a booster dose of tetanus toxoid, especially if the wound has been incised or tampered with in any way. An aminoglycoside such as gentamicin and metronidazole should be added if there is evidence of local necrosis.
Management of local envenoming
Bullae can be drained with a fine needle. The bitten limb should be nursed in the most comfortable position. Once definite signs of necrosis have appeared (blackened anaesthetic area with putrid odour or signs of sloughing), surgical debridement, immediate split skin grafting and broad-spectrum antimicrobial cover are indicated. Increased pressure within tight fascial compartments such as the digital pulp spaces and anterior tibial compartment may cause ischaemic damage. This complication is most likely after bites by North American rattlesnakes such as C. adamanteus, Calloselasma rhodostoma, Trimeresurus flavoviridis, Bothrops sp and Bitis arietans. The signs are excessive pain, weakness of the compartmental muscles and pain when they are passively stretched, hypaesthesia of areas of skin supplied by nerves running through the compartment, and obvious tenseness of the compartment. Detection of arterial pulses (e.g., by Doppler ultrasound) does not exclude intracompartmental ischaemia. Intracompartmental pressures exceeding 45 mm Hg are associated with a high risk of ischaemic necrosis. In these circumstances, fasciotomy may be considered but must not be attempted until blood coagulability and a platelet count of more than 50,000/ μl have been restored. Early adequate antivenom treatment will prevent the development of intracompartmental syndromes in most cases.
Haemostatic disturbances
Once specific antivenom has been given to neutralize venom procoagulants, restoration of coagulability and platelet function may be accelerated by giving fresh whole blood, fresh frozen plasma, cryoprecipitates (containing fibrinogen, factor VIII, fibronectin and some factors V and XIII) or platelet concentrates. Heparin must not be used. Corticosterioids have no place in the treatment of envenoming.
Treatment of snake venom ophthalmia
When cobra venom is “spat” into the eyes, first aid consists of irrigation with generous volumes of water or any other bland liquid which is available. Adrenaline drops (0.1 per cent) may relieve the pain. Unless a corneal abrasion can be excluded by fluorescein staining or slit lamp examination, treatment should be the same as for any corneal injury: a topical antimicrobial such as tetracycline or chloramphenicol should be applied. Instillation of diluted antivenom is not currently recommended.
More...
Disasters and Major Accidents
Type and Frequency of Disasters
In 1990, the 44th General Assembly of the United Nations launched the decade for the reduction of frequency and impact of natural disasters (Lancet 1990). A committee of experts endorsed a definition of disasters as “a disruption of the human ecology that exceeds the capacity of the community to function normally”.
Over the past few decades, disaster data on a global level reveal a distinct pattern with two main features—an increase over time of the number of people affected, and a geographical correlation (International Federation of Red Cross and Red Crescent Societies (IFRCRCS) 1993). In figure 1, despite the great variation from year to year, a definite rising trend is quite visible. Figure 2 shows the countries most severely affected by major disasters in 1991. Disasters affect every country of the world, but it is the poorest countries where people most frequently lose their lives.
Figure 1. Number of persons affected worldwide by disasters per year during 1967-91
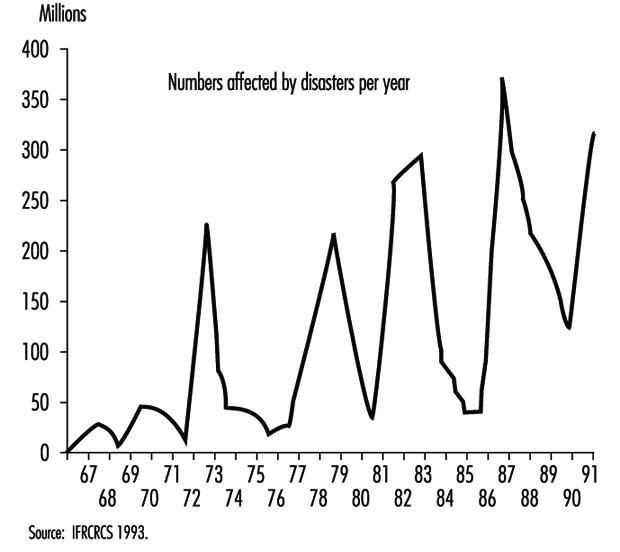
Figure 2. Number of people dead from major disasters in 1991: Top 20 countries
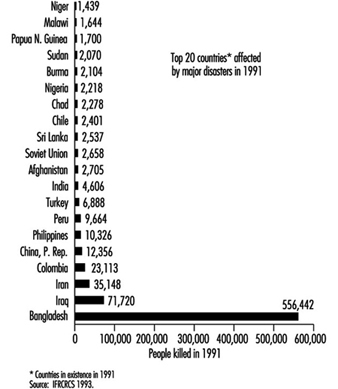
Numerous and different definitions and classifications of disasters are available and have been reviewed (Grisham 1986; Lechat 1990; Logue, Melick and Hansen 1981; Weiss and Clarkson 1986). Three of them are mentioned here as examples: The US Centers for Disease Control (CDC 1989) identified three major categories of disasters: geographical events such as earthquakes and volcanic eruptions; weather-related problems, including hurricanes, tornadoes, heat waves, cold environments and floods; and, finally, human-generated problems, which encompass famines, air pollutions, industrial disasters, fires and nuclear reactor incidents. Another classification by cause (Parrish, Falk and Melius 1987) included weather and geological events among natural disasters, whereas human-made causes were defined as non-natural, technological, purposeful events perpetuated by people (e.g., transportation, war, fire/explosion, chemical and radioactive release). A third classification (table1), compiled at the Centre for Research on the Epidemiology of Disaster in Louvain, Belgium, was based on a workshop convened by the UN Disaster Relief Organization in 1991 and was published in the World Disaster Report 1993 (IFRCRCS 1993).
Table 1. Definitions of disaster types
|
Sudden natural |
Long-term natural |
Sudden human-made |
Long-term human-made |
|
Avalanche Cold wave Earthquake Aftershock Floods Flash flood Dam collapse Volcanic eruption Glowing Heat wave High wind Storm Hail Sand storm Storm surges Thunder storm Tropical storm Tornado Insect infestation Landslide Earth flow Power shortage Tsunami and tidal |
Epidemics Drought Desertification Famine Food shortage or |
Structural collapse Building collapse Mine collapse or cave-in Air disaster Land disaster Sea disaster Industrial/technological Explosions Chemical explosions Nuclear explosion Mine explosions Pollution Acid rain Chemical pollution Atmosphere pollution Chlorofluoro-carbons Oil pollution Fires Forest/grassland fire |
National (civil strife, International Displaced population Displaced persons Refugees |
Source: IFRCRCS 1993.
Figure 3 reports the number of events for individual disaster types. The item “Accidents” includes all sudden human-made events, and is second only to “Flood” in frequency. “Storm” is in third place, followed by “Earthquake” and “Fire”.
Figure 3. 1967-91: Total number of events for each type of disaster
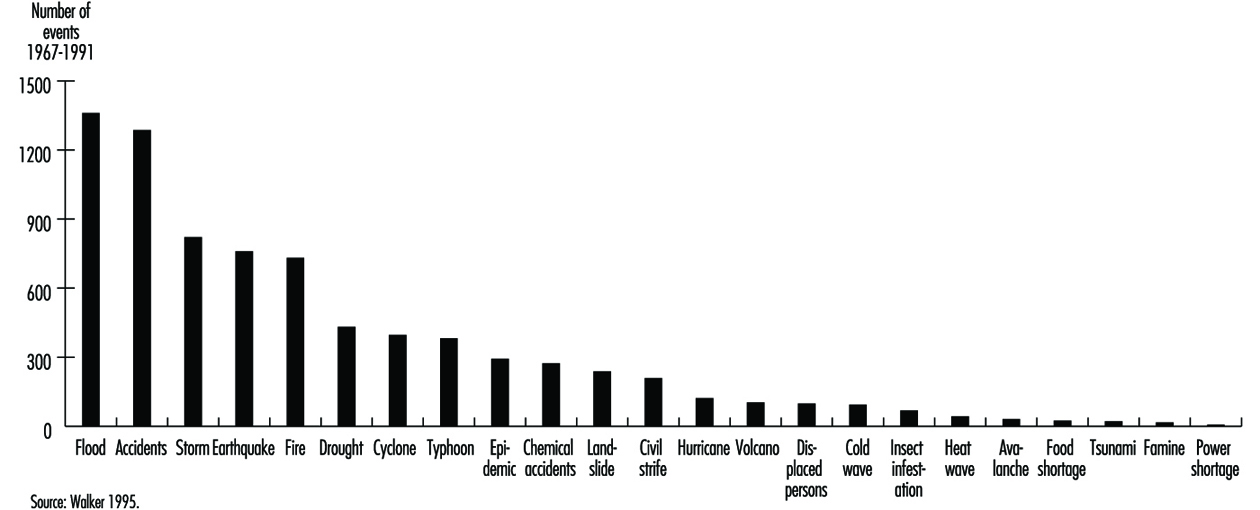
Additional information on type, frequency and consequences of natural and non-natural disasters between 1969 and 1993 has been drawn from data of the IFRCRCS 1993.
Although agencies measure the severity of disasters by the number of people killed, it is becoming increasingly important also to look at the number affected. Across the world, almost a thousand times more people are affected by disaster than are killed and, for many of these people, survival after the disaster is becoming increasingly difficult, leaving them more vulnerable to future shocks. This point is relevant not only for natural disasters (table 2) but also human-made disasters (table 3), especially in the case of chemical accidents whose effects on exposed people may become apparent after years or even decades (Bertazzi 1989). Addressing human vulnerability to disaster is at the heart of disaster preparedness and prevention strategies.
Table 2. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
76,883 |
9,027 |
56,072 |
2,220 |
99 |
144,302 |
|
Injured |
1,013 |
14,944 |
27,023 |
3,521 |
100 |
46,601 |
|
Otherwise affected |
10,556,984 |
4,400,232 |
105,044,476 |
563,542 |
95,128 |
120,660,363 |
|
Homeless |
172,812 |
360,964 |
3,980,608 |
67,278 |
31,562 |
4,613,224 |
Source: Walker 1995.
Table 3. Number of victims of disasters with a non-natural trigger from 1969 to 1993: 25-year average by region
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Killed |
16,172 |
3,765 |
2,204 |
739 |
18 |
22,898 |
|
Injured |
236 |
1,030 |
5,601 |
483 |
476 |
7,826 |
|
Affected |
3,694 |
48,825 |
41,630 |
7,870 |
610 |
102,629 |
|
Homeless |
2,384 |
1,722 |
6,275 |
7,664 |
24 |
18,069 |
Source: Walker 1995.
Drought, famine and floods continue to affect far more people than any other type of disaster. High winds (cyclones, hurricanes and typhoons) cause proportionally more deaths than famines and floods, in relation to the affected population as a whole; and earthquakes, the most sudden-onset disaster of all, continue to have the greatest ratio of deaths to affected population (table 4). Technological accidents affected more people than fires (table 5).
Table 4. Number of victims of disasters with a natural trigger from 1969 to 1993: 25-year average by type
|
Earthquake |
Drought |
Flood |
High wind |
Landslide |
Volcano |
Total |
|
|
Killed |
21,668 |
73,606 |
12,097 |
28,555 |
1,550 |
1,009 |
138,486 |
|
Injured |
30,452 |
0 |
7,704 |
7,891 |
245 |
279 |
46,571 |
|
Affected |
1,764,724 |
57,905,676 |
47,849,065 |
9,417,442 |
131,807 |
94,665 |
117,163,379 |
|
Homeless |
224,186 |
22,720 |
3,178,267 |
1,065,928 |
106,889 |
12,513 |
4,610,504 |
Source: Walker 1995.
Table 5. Disasters and Major Accidents
|
Accident |
Technological accident |
Fire |
Total |
|
|
Killed |
3,419 |
603 |
3,300 |
7,321 |
|
Injured |
1,596 |
5,564 |
699 |
7,859 |
|
Affected |
17,153 |
52,704 |
32,771 |
102,629 |
|
Homeless |
868 |
8,372 |
8,829 |
18,069 |
Source: Walker 1995.
Table 6 and table 7 show the number of grouped disaster types over 25 years, by continent. High winds, accidents (mostly transport accidents) and floods account for the largest number of disaster events, with the largest proportion of events being in Asia. Africa accounts for the vast majority of the world’s drought events. While few people are killed by disasters in Europe, the region suffers from disaster events on a scale comparable to that in Asia or Africa, the lower mortality figures reflecting a much lower human vulnerability to crisis. A clear example is the comparison of the human death tolls after the chemical accidents in Seveso (Italy) and in Bhopal (India) (Bertazzi 1989).
Table 6. Disasters with a natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
40 |
125 |
225 |
167 |
83 |
640 |
|
Drought and famine |
277 |
49 |
83 |
15 |
14 |
438 |
|
Flood |
149 |
357 |
599 |
123 |
138 |
1,366 |
|
Landslide |
11 |
85 |
93 |
19 |
10 |
218 |
|
High wind |
75 |
426 |
637 |
210 |
203 |
1,551 |
|
Volcano |
8 |
27 |
43 |
16 |
4 |
98 |
|
Other* |
219 |
93 |
186 |
91 |
4 |
593 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 7. Disasters with a non-natural trigger from 1969 to 1993: Number of events over 25 years
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
213 |
321 |
676 |
274 |
18 |
1,502 |
|
Technological accident |
24 |
97 |
97 |
88 |
4 |
310 |
|
Fire |
37 |
115 |
236 |
166 |
29 |
583 |
Source: Walker 1995.
Figures for 1994 (table 8 and table 9) show that Asia continues to be the most disaster-prone region, with major accidents, floods and high wind disasters being the most common event types. Earthquakes, while causing high death rates per event, are in fact no more common than major technological disasters. The one-year average number of non-natural events, apart from fire, is slightly diminished in comparison with the preceding 25-year period. The average numbers of natural disasters, instead, were higher, with the exception of floods and volcanoes. In 1994, Europe had more human-made disasters than Asia (39 versus 37).
Table 8. Disasters with a natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Earthquake |
3 |
3 |
12 |
1 |
1 |
20 |
|
Drought and famine |
0 |
2 |
1 |
0 |
1 |
4 |
|
Flood |
15 |
13 |
27 |
13 |
0 |
68 |
|
Landslide |
0 |
1 |
3 |
1 |
0 |
5 |
|
High wind |
6 |
14 |
24 |
5 |
2 |
51 |
|
Volcano |
0 |
2 |
5 |
0 |
1 |
8 |
|
Other* |
2 |
3 |
1 |
2 |
0 |
8 |
* Other includes: avalanche, cold wave, heat wave, insect infestation, tsunami.
Source: Walker 1995.
Table 9. Disasters with a non-natural trigger: Number by global region and type in 1994
|
Africa |
America |
Asia |
Europe |
Oceania |
Total |
|
|
Accident |
8 |
12 |
25 |
23 |
2 |
70 |
|
Technological accident |
1 |
5 |
7 |
7 |
0 |
20 |
|
Fire |
0 |
5 |
5 |
9 |
2 |
21 |
Source: Walker 1995.
Major Chemical Accidents
In this century, the worst non-natural disasters resulting in human suffering and death have been caused by wars, transport and industrial activities. At first, industrial disasters mainly affected people engaged in specific occupations, but later, particularly after the Second World War with the rapid growth and expansion of the chemical industry and the use of nuclear power, these occurrences led to serious danger even to people outside work areas, and to the general environment. We focus here on major accidents involving chemicals.
The first documented chemical disaster with industrial origins goes back to the 1600s. It was described by Bernardino Ramazzini (Bertazzi 1989). Today’s chemical disasters differ in the way they happen and in the type of chemicals involved (ILO 1988). Their potential hazard is a function both of the inherent nature of the chemical and the quantity that is present on site. A common feature is that they usually are uncontrolled events involving fires, explosions or releases of toxic substances that result either in the death and injury of a large number of people inside or outside the plant, extensive property and environmental damage, or both.
Table 10 gives some examples of typical major chemical accidents due to explosions. Table 11 lists some major fire disasters. Fires occur in industry more frequently than explosions and toxic releases, although the consequences in terms of loss of life are generally less. Better prevention and preparedness might be the explanation. Table 12 lists some major industrial accidents involving toxic releases of different chemicals. Chlorine and ammonia are the toxic chemicals most commonly used in major hazard quantities, and both have a history of major accidents. The release of flammable or toxic materials in the atmosphere may also lead to fires.
Table 10. Examples of industrial explosions
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Dimethyl ether |
245 |
3,800 |
Ludwigshafen, Federal Republic of Germany, 1948 |
|
Kerosene |
32 |
16 |
Bitburg, Federal Republic of Germany, 1948 |
|
Isobutane |
7 |
13 |
Lake Charles, Louisiana, United States, 1967 |
|
Oil slops |
2 |
85 |
Pernis, Netherlands, 1968 |
|
Propylene |
– |
230 |
East Saint Louis, Illinois, United States, 1972 |
|
Propane |
7 |
152 |
Decatur, Illinois, United States, 1974 |
|
Cyclohexane |
28 |
89 |
Flixborough, United Kingdom, 1974 |
|
Propylene |
14 |
107 |
Beek, Netherlands, 1975 |
Adapted from ILO 1988.
Table 11. Examples of major fires
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Methane |
136 |
77 |
Cleveland, Ohio, United States, 1944 |
|
Liquefied petroleum gas |
18 |
90 |
Ferzyn, France, 1966 |
|
Liquefied natural gas |
40 |
– |
Staten Island, New York, United States, 1973 |
|
Methane |
52 |
– |
Santa Cruz, Mexico, 1978 |
|
Liquefied petroleum gas |
650 |
2,500 |
Mexico City, Mexico, 1985 |
Adapted from ILO 1988.
Table 12. Examples of major toxic releases
|
Chemical involved |
Consequences |
Place and date |
|
|
Death |
Injuries |
||
|
Phosgene |
10 |
– |
Poza Rica, Mexico, 1950 |
|
Chlorine |
7 |
– |
Wilsum, Federal Republic of Germany, 1952 |
|
Dioxin/TCDD |
– |
193 |
Seveso, Italy, 1976 |
|
Ammonia |
30 |
25 |
Cartagena, Colombia, 1977 |
|
Sulphur dioxide |
– |
100 |
Baltimore, Maryland, United States, 1978 |
|
Hydrogen sulphide |
8 |
29 |
Chicago, Illinois, United States, 1978 |
|
Methyl isocyanate |
2,500 |
200,000 |
Bhopal, India, 1984 |
Adapted from ILO 1988.
A review of the literature concerning major chemical disasters enables us to identify several other common characteristics of today’s industrial disasters. We will review them briefly, to provide not only a classification of general value, but also an appreciation of the nature of the problem and the challenges that face us.
Overt Disasters
Overt disasters are environmental releases which leave no ambiguity about their sources and their potential harm. Examples are Seveso, Bhopal and Chernobyl.
Seveso plays the role of prototype for chemical industrial disasters (Homberger et al. 1979; Pocchiari et al. 1983, 1986). The accident took place on 10 July 1976 in the Seveso area, close to Milan, Italy, in a plant where trichlorophenol was produced, and it caused the contamination of several square kilometres of populated countryside by the powerfully toxic 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD). More than 700 people were evacuated, and restrictions were applied to another 30,000 inhabitants. The most clearly established health effect was chloracne, but the picture of health consequences possibly linked to this incident has not yet been completed (Bruzzi 1983; Pesatori 1995).
Bhopal represents, probably, the worst chemical industrial disaster ever (Das 1985a, 1985b; Friedrich Naumann Foundation 1987; Tachakra 1987). On the night of 2 December 1984, a gas leak caused a deadly cloud to spread over the city of Bhopal, in central India, leaving thousands dead and hundreds of thousands injured in the space of a few hours. The accident occurred because of a runaway reaction in one of the tanks in which methyl isocyanate (MIC) was stored. The concrete storage tank, containing some 42 tons of this compound, which was used to manufacture pesticides, burst open and vented MIC and other breakdown chemicals into the air. Above and beyond the obvious catastrophic impact of the accident, questions still exist as to the possible long-term consequences for the health of those affected and/or exposed (Andersson et al. 1986; Sainani et al. 1985).
Slow-Onset Disasters
Slow-onset disasters may become apparent only because human targets happen to be on the release path, or because, as time passes, some environmental evidence of a threat from noxious materials crops up.
One of the most impressive and instructive examples of the first type is “Minamata disease”. In 1953 unusual neurological disorders began to strike people living in fishing villages along Minamata Bay, Japan. The disease was named kibyo, the “mystery illness”. After numerous investigations, poisoned fish emerged as the probable culprit, and in 1957 the disease was produced experimentally by feeding cats with fish caught in the bay. The following year, the suggestion was put forward that the clinical picture of kibyo, which included polyneuritis, cerebellar ataxia and cortical blindness, was similar to that due to poisoning by alkyl mercury compounds. A source of organic mercury had to be sought, and it was eventually found in a factory discharging its effluent into Minamata Bay. By July 1961, the disease had occurred in 88 persons, of whom 35 (40%) had died (Hunter 1978).
An example of the second type is Love Canal, an excavation site near Niagara Falls in the United States. The area had been used as a chemical and municipal disposal site over a period of about 30 years, until 1953. Homes were later built next to the landfill. In the late 1960s, there were complaints of chemical odours in home basements, and chemical leaching in areas surrounding the site began to be reported with increasing frequency over time. In the 1970s, residents began to fear that a serious threat to their health could arise, and this shared perception prompted environmental and health investigations to be carried out. None of the published studies could conclusively support a causal link between exposure to chemicals at the disposal site and adverse health effects among the residents. Yet, there is no doubt that serious social and psychological consequences have resulted among the population in the area, particularly those who were evacuated (Holden 1980).
Mass Food Poisonings
Outbreaks of food poisoning can be caused by toxic chemicals released into the environment through the use of chemicals in the handling and processing of food. One of the most serious episodes of this type occurred in Spain (Spurzem and Lockey 1984; WHO 1984; Lancet 1983). In May 1981, an outbreak of a previously unknown syndrome began to appear in the working-class suburbs of Madrid. Over 20,000 persons were ultimately involved.
By June 1982, 315 patients had died (around 16 deaths per 1,000 cases). Initially, the clinical features included interstitial pneumonitis, diverse skin rashes, lymphadenopathies, intense eosinophilia, and gastro-intestinal symptoms. Nearly one-fourth of those who survived the acute phase required later hospitalization for neuromuscular alterations. Schleroderma-like changes of the skin also were observed in this late stage along with pulmonary hypertension and Raynaud’s phenomenon.
One month after the occurrence of the first cases, the illness was found to be associated with the consumption of inexpensive denatured rapeseed oil, sold in unlabelled plastic containers and usually acquired from itinerant salesmen. The warning issued by the Spanish government against the consumption of the suspected oil caused a dramatic fall in the number of hospitalizations from toxic pneumonitis (Gilsanz et al. 1984; Kilbourne et al. 1983).
Polychlorinated biphenyls (PCBs) were involved in other widely reported accidental mass food poisonings in Japan (Masuda and Yoshimura 1984) and in Taiwan (Chen et al. 1984).
Transnational Disasters
Today’s human-made disasters do not necessarily respect national political boundaries. An obvious example is Chernobyl, whose contamination reached from the Atlantic Ocean to the Ural Mountains (Nuclear Energy Agency, 1987). Another example comes from Switzerland (Friedrich Naumann Foundation 1987; Salzman 1987). On 1 November 1986, shortly after midnight, a fire developed in a warehouse operated by the multinational pharmaceutical company Sandoz in Schweizerhalle, 10 km southeast of Basel, and some 30 tons of the chemicals stored in the warehouse were drained along with water from the fire-fighting into the nearby River Rhine. Severe ecological damage occurred over a length of about 250 km. Apart from symptoms of irritation reported in the parts of the Basel area reached by gases and vapours produced by the fire, no cases of serious illness were reported. Nonetheless, this accident triggered serious concern in at least four European countries (Switzerland, France, Germany, The Netherlands).
Transnationality applies not only to consequences and harm caused by disasters, but also to their remote causes. Bhopal might serve as an example. In analysing the causes of that disaster, some persons reached the conclusion that “The Bhopal disaster occurred because of specific acts and decisions which were taken in Danbury, Connecticut or elsewhere in the corporate superstructure, but not in Bhopal.” (Friedrich Naumann Foundation 1987.)
“Developing” Disasters
The emerging pattern of industrialization as well as modernization of agriculture in developing countries involves the application and use of imported or adopted technology and products, within contexts which are quite different from those in which they were intended to be used. Businesses facing the tightening of regulations in industrial countries may export hazardous industries to world regions where less stringent measures for protection of the environment and public health exist. Industrial activities become concentrated in existing urban settlements and add significantly to the pressure caused by overcrowding and shortages of community services. Such activities are distributed between a small highly organized sector and a large unorganized sector; governmental controls in regard to labour and environmental safety in the latter sector are less stringent (Krishna Murti 1987). An example comes from Pakistan, where among 7,500 field workers in a malaria control programme in 1976, as many as 2,800 experienced some form of toxicity (Baker et al. 1978). It was also estimated that about 500,000 acute pesticide poisonings occur annually, resulting in about 9,000 deaths, and that only about 1% of the deadly cases occur in industrialized countries, although those countries consume about 80% of the total world agrochemical production (Jeyaratnam 1985).
It has also been argued that developing societies might actually find themselves carrying a double burden instead of being cleared from the one of underdevelopment. It could be, in fact, that the consequences of improper industrialization are simply being added to those of the countries’ underdeveloped states (Krishna Murti 1987). It is clear, thus, that international cooperation ought to be urgently strengthened in three domains: scientific work, public health and industrial siting and safety policies.
Lessons for the Future
Despite the variety of the reviewed industrial disasters, some common lessons have been learned on how to prevent their occurrence, and also on how to mitigate the impact of major chemical disasters on the population. In particular:
- Different experts should be on the scene working in close coordination; they should usually cover the fields related to the environmental fate of the agent, its toxic properties to humans and biota, analytical methods, clinical medicine and pathology, biostatistics and epidemiology.
- Based on pre-existing and/or early available evidence, a comprehensive study plan should be developed as early as possible to identify goals, problems and resource requirements.
- Early phase activities affect the course of any subsequent action. Since long-term effects should be expected after virtually every type of industrial disaster, great care should be devoted to insure availability of requisite information for later studies (e.g., proper identifiers of the exposed for follow-up).
- In planning long-term investigations, feasibility should be given high consideration to facilitate scientific and public health achievements and clarity of communication.
- Overall, for reasons of validity and cost effectiveness, it is advisable to rely on “hard” information, whenever available, either in identifying and enumerating the study population (e.g., residence) or in estimating exposure (e.g., environmental and biological measurements) and choosing the endpoints (e.g., mortality).
Control of Major Hazard Installations for the Prevention of Major Accidents
The objective of this article is to provide guidance for establishing a system to control major hazard installations. Two ILO documents and the more recent ILO Convention (see "ILO Convention") form the basis of the first part of this article. The European Directive forms the basis for the second part of this article.
The ILO Perspective
Much of what follows has been extracted from two documents Prevention of Major Industrial Accidents (ILO 1991) and Major Hazard Control: A Practical Manual (ILO 1988). The document “Convention concerning the Prevention of Major Industrial Accidents” (ILO 1993) (see "ILO Convention") serves to complement and update material from the earlier two documents. Each of these documents proposes ways to protect workers, the public and the environment against the risk of major accidents by (1) preventing major accidents from occurring at these installations and (2) minimizing the consequences of a major accident onsite and offsite, for example by (a) arranging appropriate separation between major hazard installations and housing and other centres of population nearby, such as hospitals, schools and shops, and (b) appropriate emergency planning.
The 1993 ILO Convention should be referred to for specifics; what follows is more of a narrative overview of the document.
Major hazard installations possess the potential, by virtue of the nature and quantity of hazardous substances present, to cause a major accident in one of the following general categories:
- the release of toxic substances in tonnage quantities which are lethal or harmful even at considerable distances from the point of release through contamination of air, water and/or soil
- the release of extremely toxic substances in kilogram quantities, which are lethal or harmful even at considerable distance from the point of release
- the release of flammable liquids or gases in tonnage quantities, which may either burn to produce high levels of thermal radiation or form an explosive vapour cloud
- the explosion of unstable or reactive materials.
Member country obligations
The 1993 Convention expects member countries who are not immediately able to implement all of the preventive and protective measures provided for in the Convention:
- to draw up plans, in consultation with the most representative organizations of employers and workers, and with other interested parties who may be affected, for the progressive implementation of said measures within a fixed time-frame
- to implement and periodically review a coherent national policy concerning the protection of workers, the public and the environment against the risk of major accidents
- to implement the policy through preventive and protective measures for major hazard installations and, where, practicable, promote the use of the best available safety technologies and
- to apply the Convention in accordance with national law and practice.
Components of a major hazard control system
The variety of major accidents leads to the concept of major hazard as an industrial activity requiring controls over and above those applied in normal factory operations, in order to protect both workers and people living and working outside. These controls aim not only at preventing accidents but also at mitigating the consequences of any accidents which could occur.
Controls need to be based on a systematic approach. Basic components of this system are:
- identification of major hazard installations together with their respective threshold quantities and inventory. Governmental authorities and employers should require the identification of major hazard installations on a priority basis; these should be regularly reviewed and updated.
- information about the installation. Once the major hazard installations have been identified, additional information needs to be collected about their design and operation. The information should be gathered and arranged systematically, and should be accessible to all parties concerned within the industry and outside the industry. In order to achieve a complete description of the hazards, it may be necessary to carry out safety studies and hazard assessments to discover possible process failures and to set priorities during the process of hazard assessment.
- special provision to protect confidential information
- action inside the industrial activity. Employers have the primary responsibility for operating and maintaining a safe facility. A sound safety policy is required. Technical inspection, maintenance, facility modification, training and selecting of suitable personnel must be carried out according to standard quality control procedures for major hazard installations. In addition to the preparation of the safety report, accidents of any type should be investigated and copies of reports submitted to the competent authority.
- actions by the government or other competent authorities. Assessment of the hazards for the purposes of licensing (where appropriate), inspection and enforcement of legislation. Land-use planning can appreciably reduce the potential for a disaster. The training of factory inspectors also is an important role of the government or other competent authority.
- emergency planning. This aims at the reduction of the consequences of major accidents. In setting up emergency planning, a distinction is made between onsite and offsite planning.
The responsibilities of employers
Major hazard installations have to be operated at a very high standard of safety. In addition, employers play a key role in the organization and implementation of a major hazard control system. In particular, as outlined in table 13, employers have the responsibility to:
- Provide the information required to identify major hazard installations within a fixed time-frame.
- Carry out the hazard assessment.
- Report to the competent authority on the results of the hazard assessment.
- Introduce technical measures, including design, safety systems construction, choice of chemicals, operation, maintenance and systematic inspection of the installation.
- Introduce organizational measures, including, among others, training and instruction of personnel and staffing levels.
- Set up an emergency plan.
- Take measures to improve plant safety and limit the consequences of an accident.
- Consult with workers and their representatives.
- Improve the system by learning from near misses and related information.
- Ensure that quality control procedures are in effect and audit these periodically.
- Notify the competent authority before any permanent closure of a major hazard installation.
Table 13. The role of major hazard installations management in hazard control
|
Actions (depending on local legislation) |
Action in the event of a major |
|||
|
Provide notification to authorities |
Provide information on |
Prepare an onsite emergency plan |
Inform the public about the major hazard |
Notify authority about major accident |
|
Prepare and submit safety report |
Provide further information on request |
Provide information to local authority to enable it to draw |
Provide information on major accident |
|
First and foremost, employers of installations which can cause a major accident have a duty to control this major hazard. To do this, they must be aware of the nature of the hazard, of the events that cause accidents, and of the potential consequences of such accidents. This means that, in order to control a major hazard successfully, employers must have answers to the following questions:
- Do toxic, explosive or flammable substances in the facility constitute a major hazard?
- Do chemicals or agents exist which, if combined, could become a toxic hazard?
- Which failures or errors can cause abnormal conditions leading to a major accident?
- If a major accident occurs, what are the consequences of a fire, an explosion or a toxic release for the employees, people living outside the facility, the plant or the environment?
- What can management do to prevent these accidents from happening?
- What can be done to mitigate the consequences of an accident?
Hazard assessment
The most appropriate way to answer the above questions is to carry out a hazard assessment, the purpose of which is to understand why accidents occur and how they can be avoided or at least mitigated. Methods which can be used for an assessment are summarized in table 14.
Table 14. Working methods for hazard assessment
|
Method |
Purpose |
Aim |
Working principle |
|
1. Preliminary hazard analysis |
1. Identification of hazards |
1. Completeness of safety concept |
1. Use of “thinking aids” |
|
2. Matrix diagrams of |
|||
|
3. Use of check-lists |
|||
|
4. Failure effect |
2. Use of “searching |
||
|
5. Hazard and |
|||
|
6. Accident sequence |
2. Assessment of hazard according to |
2. Optimization of |
3. Graphic description |
|
7. Fault tree analysis |
|||
|
8. Accident consequence analysis |
3. Assessment of accident consequences |
3. Mitigation of |
4. Mathematical |
Source: ILO 1988.
Safe operation
A general outline of how the hazards should be controlled will be given.
Plant component design
A component has to withstand the following: static loads, dynamic loads, internal and external pressure, corrosion, loads arising from large differences in temperature, loads arising from external impacts (wind, snow, earthquakes, settling). Design standards are therefore a minimum requirement as far as major hazard installations are concerned.
Operation and control
When an installation is designed to withstand all loads that can occur during normal or foreseen abnormal operating conditions, it is the task of a process control system to keep the plant safely within these limits.
In order to operate such control systems, it is necessary to monitor the process variables and active parts of the plant. Operating personnel should be well trained to be aware of the mode of operation and the importance of the control system. To ensure that the operating personnel do not have to rely solely on the functioning of automatic systems, these systems should be combined with acoustic or optical alarms.
It is most important to realize that any control system will have problems in rare operating conditions such as start-up and shut-down phases. Special attention must be paid to these phases of operation. Quality control procedures will be audited by management periodically.
Safety systems
Any major hazard installation will require some form of safety system. The form and design of the system depend on the hazards present in the plant. The following gives a survey of available safety systems:
- systems preventing deviation from permissible operating conditions
- systems preventing failure of safety-related components
- safety-related utility supplies
- alarm systems
- technical protective measures
- prevention of human and organizational errors.
Maintenance and monitoring
The safety of a plant and the function of a safety-related system can only be as good as the maintenance and monitoring of these systems.
Inspection and repair
It is necessary to establish a plan for onsite inspections, for the operating personnel to follow, which should include a schedule and the operating conditions to be adhered to during inspection work. Strict procedures must be specified for carrying out repair work.
Training
As people can have a negative as well as a positive influence on plant safety, it is important to reduce the negative influences and support the positive ones. Both goals can be achieved by proper selection, training and periodic evaluation/assessment of the personnel.
Mitigation of consequences
Even if a hazard assessment has been carried out and the hazards have been detected and appropriate measures to prevent accidents have been taken, the possibility of an accident cannot be completely ruled out. For this reason, it must be part of the safety concept to plan and provide measures which can mitigate the consequences of an accident.
These measures have to be consistent with the hazards identified in the assessment. Furthermore, they must be accompanied by proper training of plant personnel, the emergency forces and responsible representatives from public services. Only training and rehearsals of accident situations can make emergency plans realistic enough to work in a real emergency.
Safety reporting to the competent authority
Depending on local arrangements in different countries, employers of a major hazard installation shall report to the appropriate competent authority. Reporting may be carried out in three steps. These are:
- identification/notification of major hazard installation (including any future changes that are to be made to the installation)
- the preparation of periodic safety reports (which shall be revised in the light of any modifications made to a facility)
- immediate reporting of any type of accident, followed by a detailed report.
Rights and duties of workers and their representatives
Workers and their representatives shall be consulted through appropriate cooperative mechanisms in order to ensure a safe system of work. They shall be consulted in the preparation of, and have access to, safety reports, emergency plans and procedures, and accident reports. They shall receive training for preventing major accidents and in emergency procedures to be followed in the event of a major accident. Finally, workers and their representatives should be able to take corrective action where needed within the scope of their duties, if they believe that there is any imminent danger of a major accident. They also have the right to notify the competent authority of any hazard.
Workers shall comply with all practices and procedures for preventing major accidents and for the control of developments likely to lead to a major accident. They shall comply with all emergency procedures should a major accident occur.
Implementation of a major hazard control system
Although the storage and use of large quantities of hazardous materials is widespread across most countries of the world, the present systems for their control will differ substantially from one country to another. This means that the speed of implementation of a major hazard control system will depend on the facilities already existing in each country, particularly with regard to trained and experienced facility inspectors, together with the resources available locally and nationally for the different components of the control system. For all countries, however, implementation will require the setting of priorities for a stage-by-stage programme.
Identification of major hazards
This is the essential starting point for any major hazard control system—the definition of what actually constitutes a major hazard. Although definitions exist in some countries and particularly in the EU, a particular country’s definition of a major hazard should reflect local priorities and practices and, in particular, the industrial pattern in that country.
Any definition for identifying major hazards is likely to involve a list of hazardous materials, together with an inventory for each, such that any major hazard installation storing or using any of these in excess quantities is by definition a major hazard installation. The next stage is to identify where the major hazard installation exists for any particular region or country. Where a country wishes to identify major hazard installations before the necessary legislation is in place, considerable progress can be achieved informally, particularly where the cooperation of industry is available. Existing sources such as factory inspectorate records, information from industrial bodies and so on, may enable a provisional list to be obtained which, apart from allowing early inspection priorities to be allocated, will enable an assessment to be made of the resources required for different parts of the control system.
Establishment of a group of experts
For countries considering establishing a major hazard control system for the first time, an important first stage is likely to be setting up a group of experts as a special unit at government level. The group will have to set priorities in deciding on its initial programme of activity. The group may be required to train factory inspectors in the techniques of major hazard inspection, including operational standards for such major hazard installations. They should also be able to provide advice about the siting of new major hazards and the use of land nearby. They will need to establish contacts in other countries in order to keep up to date with major hazard developments.
Onsite emergency preparedness
Emergency plans require that the major hazard installation be assessed for the range of accidents that could take place, together with how they would be tackled in practice. The handling of these potential accidents will require both staff and equipment, and a check should be made to ensure that both are available in sufficient numbers. The plans should include the following elements:
- assessment of the size and nature of the events foreseen and the probability of their occurrence
- formulation of the plan and liaison with outside authorities, including emergency services
- procedures: (a) raising the alarm; (b) communications within the plant and outside the plant
- appointment of key personnel and their duties and responsibilities
- emergency control centre
- action onsite and offsite.
Offsite emergency preparedness
This is an area which has received less attention than onsite emergency planning, and many countries will be faced with considering this for the first time. The offsite emergency plan will have to link the possible accidents identified by the major hazard installation, their expected likelihood of occurrence and the proximity of people living and working nearby. It must have addressed the need for the expeditious warning and evacuation of the public, and how these might be achieved. It should be remembered that conventional housing of solid construction offers substantial protection from toxic gas clouds, whereas a shanty-type house is vulnerable to such accidents.
The emergency plan must identify organizations whose help will be required in the event of an emergency and must ensure that they know what role is expected of them: hospitals and medical staff should, for example, have decided how they would handle large numbers of casualties and in particular what treatment they would provide. The offsite emergency plan will need to be rehearsed with public involvement from time to time.
Where a major accident could have transboundary effects, full information is to be provided to the jurisdictions concerned, as well as assistance in cooperation and coordination arrangements.
Siting
The basis for needing a siting policy for major hazard installations is straightforward: since absolute safety cannot be guaranteed, major hazard installations should be separated from people living and working outside the facility. As a first priority, it may be appropriate to concentrate efforts on proposed new major hazards and to try to prevent the encroachment of housing, particularly shanty houses, which are a common feature in many countries.
Training and facility inspectors
The role of the facility inspectors is likely to be central in many countries in implementing a major hazard control system. Facility inspectors will have the knowledge that will enable early identification of major hazards to take place. Where they have specialist inspectors to call upon, factory inspectors will be assisted in the often highly technical aspects of major hazard inspection.
Inspectors will need appropriate training and qualifications to aid them in this work. Industry itself is likely to be the largest source of technical expertise within many countries, and may be able to provide assistance in facility inspectorate training.
The competent authority shall have the right to suspend any operation which poses an imminent threat of a major accident.
Evaluation of major hazards
This should be carried out by specialists, if possible according to guidelines drawn up, for example, by the group of experts or by specialist inspectors, possibly with assistance from the major hazard installation employer management group. Evaluation involves a systematic study for major accident hazard potential. It will be a similar exercise, although in much less detail, to that carried out by the major hazard installation management in producing its safety report for the facility inspectorate and in establishing an onsite emergency plan.
Evaluation will include a study of all handling operations of hazardous materials, including transport.
An examination of the consequences of process instability or major changes in the process variables will be included.
The evaluation also should consider the positioning of one hazardous material in relation to another.
The consequences of common mode failure will also need to be assessed.
The evaluation will consider the consequences of the identified major accidents in relation to offsite populations; this may determine whether the process or plant can be put into operation.
Information to the public
Experience of major accidents, particularly those involving toxic gas releases, has shown the importance of the public nearby having prior warning of: (a) how to recognize that an emergency is occurring; (b) what action they should take; and (c) what remedial medical treatment would be appropriate for anyone being affected by the gas.
For inhabitants of conventional housing of solid construction, the advice in the event of an emergency usually is to go indoors, close all doors and windows, switch off all ventilation or air conditioning, and switch on the local radio for further instructions.
Where large numbers of shanty-dwellers live close to a major hazard installation, this advice would be inappropriate, and large-scale evacuation might be necessary.
Prerequisites for a major hazard control system
Personnel
A fully developed major hazard control system requires a wide variety of specialized personnel. Apart from industrial staff concerned either directly or indirectly with the safe operation of the major hazard installation, required resources include general factory inspectors, specialist inspectors, risk assessors, emergency planners, quality control officers, local authority land planners, police, medical facilities, river authorities and so on, plus legislators to promulgate new legislation and regulations for major hazard control.
In most countries, human resources for these tasks are likely to be limited, and the setting of realistic priorities is essential.
Equipment
A feature of establishing a major hazard control system is that much can be achieved with very little equipment. Factory inspectors will not need much in addition to their existing safety equipment. What will be required is the acquisition of technical experience and knowledge and the means to relay this from the group of experts to, say, the regional labour institute, the facility inspectorate and the industry. Additional training aids and facilities may be necessary.
Information
A key element in establishing a major hazard control system is obtaining state-of-the-art information and quickly passing this information on to all those who will need it for their safety work.
The volume of literature covering the various aspects of major hazards work is now considerable, and, used selectively, this could provide an important source of information to a group of experts.
Responsibility of exporting countries
When, in an exporting member country, the use of hazardous substances, technologies or processes is prohibited as a potential source of a major accident, the information on this prohibition and the reasons for it shall be made available by the exporting member country to any importing country.
Certain non-binding recommendations flowed from the Convention. In particular, one had a transnational focus. It recommends that a national or a multinational enterprise with more than one establishment or facility should provide safety measures relating to the prevention of major accidents and the control of developments likely to lead to a major accident, without discrimination, to the workers in all its establishments, regardless of the place or country in which they are situated. (The reader should also refer to the section “Transnational disasters” in this article.)
The European Directive on Major Accident Hazards of Certain Industrial Activities
Following serious incidents in the chemical industry in Europe in the last two decades, specific legislation covering major hazard activities was developed in various countries in Western Europe. A key feature in the legislation was the obligation of the employer of a major hazard industrial activity to submit information about the activity and its hazards based on the results of systematic safety studies. After the accident in Seveso (Italy) in 1976, the major hazard regulations in the various countries were put together and integrated in an EC Directive. This Directive, on the major accident hazards of certain industrial activities, has been in force since 1984 and is often referred to as the Seveso Directive (Council of the European Communities 1982, 1987).
For the purpose of identifying major hazard installations, the EC Directive uses criteria based on the toxic, flammable and explosive properties of the chemicals (see table 15).
Table 15. EC Directive criteria for major hazard installations
|
Toxic substances (very toxic and toxic): |
|||
|
Substances showing the following values of acute toxicity and having physical and chemical properties capable of entailing major accident hazards: |
|||
|
LD50 oral. rat mg/kg |
LD50 cut. rat/rab mg/kg |
LC50 ihl. 4hr. rat mg/1 |
|
|
1. |
LD50 <5 |
LD <1 |
LD50 <0.10 |
|
2. |
5<LD50 <25 |
10 <LD50 <50 |
0.1<LC50 <0.5 |
|
3. |
25 <LD50 <200 |
50 <LD50 <400 |
0.5 <LC50 <2 |
|
Flammable substances: |
|||
|
1. |
Flammable gases: substances which in the gaseous state at normal pressure and mixed with air become flammable and the boiling-point of which at normal pressure is 20 ºC or below. |
||
|
2. |
Highly flammable liquids: substances which have a flashpoint lower than 21 °C and the boiling point of which at normal pressure is above 20 °C. |
||
|
3. |
Flammable liquids: substances which have a flashpoint lower than 55 °C and which remain liquid under pressure, where particular processing conditions, such as high pressure and high temperature, may create major accident hazards. |
||
|
Explosive substances: |
|||
|
Substances which may explode under the effect of flame or which are more sensitive to shocks or friction than dinitrobenzene. |
|||
For the selection of specific major hazard industrial activities, a list of substances and threshold limits is provided in annexes to the Directive. An industrial activity is defined by the Directive as the aggregate of all installations within a distance of 500 metres of each other and belonging to the same factory or plant. When the quantity of the substances present exceeds the given threshold limit appearing in the list, the activity is referred to as a major hazard installation. The list of substances consists of 180 chemicals, whereas the threshold limits vary between 1 kg for extremely toxic substances to 50,000 tonnes for highly flammable liquids. For isolated storage of substances, a separate list of a few substances is given.
In addition to flammable gases, liquids and explosives, the list contains chemicals such as ammonia, chlorine, sulphur dioxide and acrylonitrile.
In order to facilitate the application of a major hazard control system and to encourage the authorities and management to apply it, it must be priority oriented, with attention being focused on the more hazardous installations. A suggested list of priorities is given in table 16.
Table 16. Priority chemicals used in identifying major hazard installations
|
Names of substances |
Quantity (>) |
EC list serial number |
|
General flammable substances: |
||
|
Flammable gases |
200 t |
124 |
|
Highly flammable liquids |
50,000 t |
125 |
|
Specific flammable substances: |
||
|
Hydrogen |
50 t |
24 |
|
Ethylene oxide |
50 t |
25 |
|
Specific explosives: |
||
|
Ammonium nitrate |
2,500 t |
146 b |
|
Nitroglycerine |
10 t |
132 |
|
Trinitrotoluene |
50 t |
145 |
|
Specific toxic substances: |
||
|
Acrylonitrile |
200 t |
18 |
|
Ammonia |
500 t |
22 |
|
Chlorine |
25 t |
16 |
|
Sulphur dioxide |
250 t |
148 |
|
Hydrogen sulphide |
50 t |
17 |
|
Hydrogen cyanide |
20 t |
19 |
|
Carbon disulphide |
200 t |
20 |
|
Hydrogen fluoride |
50 t |
94 |
|
Hydrogen chloride |
250 t |
149 |
|
Sulphur trioxide |
75 t |
180 |
|
Specific very toxic substances: |
||
|
Methyl isocyanate |
150 kg |
36 |
|
Phosgene |
750 kg |
15 |
With the chemicals shown in the table acting as a guide, a list of installations can be identified. If the list is still too big to be coped with by the authorities, new priorities can be set by means of setting new quantity thresholds. Priority setting also can be used inside the factory to identify the more hazardous parts. In view of the diversity and complexity of industry in general, it is not possible to restrict major hazard installations to certain sectors of industrial activity. Experience, however, indicates that major hazard installations are most commonly associated with the following activities:
- petrochemical works and refineries
- chemical works and chemical production plants
- LPG storage and terminals
- stores and distribution centres for chemicals
- large fertilizer stores
- explosives factories
- works in which chlorine is used in bulk quantities.
Disaster Preparedness
Over the last two decades the emphasis in disaster reduction has switched from mainly improvised relief measures in the post-impact phase to forward planning, or disaster preparedness. For natural disasters this approach has been embraced in the philosophy of the United Nations International Decade for Natural Disaster Reduction (IDNDR) programme. The following four phases are the components of a comprehensive hazard management plan which can be applied to all types of natural and technological disasters:
- pre-disaster planning
- emergency preparedness
- emergency response
- post-impact recovery and reconstruction.
The aim of disaster preparedness is to develop disaster prevention or risk reduction measures in parallel with emergency preparedness and response capabilities. In this process hazard and vulnerability analyses are the scientific activities which provide the basis for the applied tasks of risk reduction and emergency preparedness to be undertaken in collaboration with planners and the emergency services.
Most health professionals would see their role in disaster preparedness as one of planning for the emergency treatment of large numbers of casualties. However, if the impact of disasters is to be drastically reduced in the future, the health sector needs to be involved in the development of preventive measures and in all phases of disaster planning, with scientists, engineers, emergency planners and decision makers. This multidisciplinary approach poses a major challenge to the health sector at the end of the 20th century as natural and human-made calamities become increasingly destructive and costly in terms of lives and property with the expansion of human populations across the globe.
Natural sudden or rapid-onset disasters include extreme weather conditions (floods and high winds), earthquakes, landslides, volcanic eruptions, tsunamis and wild fires, and their impacts have much in common. Famines, drought and desertification, on the other hand, are subject to more long-term processes which at present are only very poorly understood, and their consequences are not so amenable to reduction measures. Presently the most common cause of famine is war or so-called complex disasters (e.g., in Sudan, Somalia or former Yugoslavia).
Large numbers of displaced persons are a common feature of natural and complex disasters, and their nutritional and other health needs require specialized management.
Modern civilization is also becoming accustomed to technological or human-made disasters such as acute air pollution episodes, fires and chemical and nuclear reactor accidents, the last two being the most important today. This article will focus on disaster planning for chemical disasters, as nuclear power accidents are dealt with elsewhere in the Encyclopaedia.
Natural Sudden-Onset Disasters
The most important of these in terms of destructiveness are floods, hurricanes, earthquakes and volcanic eruptions. There have already been some well-publicized successes in disaster reduction through early warning systems, hazard mapping and structural engineering measures in seismic zones.
Thus satellite monitoring using global weather forecasting, together with a regional system for timely delivery of warnings and effective evacuation planning, was responsible for the comparatively small loss of life (just 14 deaths) when Hurricane Hugo, the strongest hurricane so far recorded in the Caribbean, struck Jamaica and the Cayman Islands in 1988. In 1991 adequate warnings provided by Philippine scientists closely monitoring Mount Pinatubo saved many thousands of lives through timely evacuation in one of the largest eruptions of the century. But the “technological fix” is only one aspect of disaster mitigation. The large human and economic losses wrought by disasters in developing countries highlight the major importance of socio-economic factors, above all poverty, in increasing vulnerability, and the need for disaster preparedness measures to take these into account.
Natural disaster reduction has to compete in all countries with other priorities. Disaster reduction can also be promoted through legislation, education, building practices and so on, as part of a society’s general risk reduction programme or safety culture—as an integral part of sustainable development policies and as a quality assurance measure for investment strategies (e.g., in the planning of buildings and infrastructure in new land developments).
Technological Disasters
Clearly, with natural hazards it is impossible to prevent the actual geological or meteorological process from occurring.
However, with technological hazards, major inroads into disaster prevention can be made using risk reduction measures in the design of plants and governments can legislate to establish high standards of industrial safety. The Seveso Directive in EC countries is an example which also includes requirements for the development of onsite and offsite planning for emergency response.
Major chemical accidents comprise large vapour or flammable gas explosions, fires, and toxic releases from fixed hazardous installations or during the transport and distribution of chemicals. Special attention has been given to the storage in large quantities of toxic gases, the most common being chlorine (which, if suddenly released due to the disruption of a storage tank or from a leak in a pipe, can form large denser-than-air clouds which can be blown in toxic concentrations for large distances downwind). Computer models of dispersion of dense gases in sudden releases have been produced for chlorine and other common gases and these are used by planners to devise emergency response measures. These models can also be used to determine the numbers of casualties in a reasonably foreseeable accidental release, just as models are being pioneered for predicting the numbers and types of casualties in major earthquakes.
Disaster Prevention
A disaster is any disruption of the human ecology that exceeds the capacity of the community to function normally. It is a state which is not merely a quantitative difference in the functioning of the health or emergency services—for example, as caused by a large influx of casualties. It is a qualitative difference in that the demands cannot be adequately met by a society without help from unaffected areas of the same or another country. The word disaster is too often used loosely to describe major incidents of a highly publicized or political nature, but when a disaster has actually occurred there may be a total breakdown in normal functioning of a locality. The aim of disaster preparedness is to enable a community and its key services to function in such disorganized circumstances in order to reduce human morbidity and mortality as well as economic losses. Large numbers of acute casualties are not a prerequisite for a disaster, as was shown in the chemical disaster at Seveso in 1976 (when a massive evacuation was mounted because of fears of long-term health risks arising from ground contamination by dioxin).
“Near disasters” may be a better description of certain events, and outbreaks of psychological or stress reactions may also be the only manifestation in some events (e.g., at the reactor accident at Three Mile Island, USA, in 1979). Until the terminology becomes established we should recognize Lechat’s description of the health objectives of disaster management, which include:
- prevention or reduction of mortality due to the impact, to a delay in rescue and to lack of appropriate care
- provision of care for casualties such as immediate post-impact trauma, burns and psychological problems
- management of adverse climatic and environmental conditions (exposure, lack of food and drinking water)
- prevention of short-term and long-term disaster-related morbidity (e.g., outbreaks of communicable diseases due to disruption of sanitation, living in temporary shelters, overcrowding and communal feeding; epidemics such as malaria due to interruption of control measures; rise of morbidity and mortality due to disruption of the health care system; mental and emotional problems)
- ensuring restoration of normal health by preventing long-term malnutrition due to disruption of food supplies and agriculture.
Disaster prevention cannot take place in a vacuum, and it is essential that a structure exists at the national governmental level of every country (the actual organization of which will vary from country to country), as well as at the regional and community level. In countries with high natural risks, there may be few ministries which can avoid being involved. The responsibility for planning is given to existing bodies such as armed forces or civil defence services in some countries.
Where a national system exists for natural hazards it would be appropriate to build on to it a response system for technological disasters, rather than devise a whole new separate system. The Industry and Environment Programme Activity Centre of the United Nations Environment Programme has developed the Awareness and Preparedness for Emergencies at Local Level (APELL) Programme. Launched in cooperation with industry and government, the programme aims to prevent technological accidents and reduce their impacts in developing countries by raising community awareness of hazardous installations and providing assistance in developing emergency response plans.
Hazard Assessment
The different types of natural disaster and their impacts need to be assessed in terms of their likelihood in all countries. Some countries such as the UK are at low risk, with wind storms and floods being the main hazards, while in other countries (e.g., the Philippines) there is a wide range of natural phenomena which strike with relentless regularity and can have serious effects on the economy and even the political stability of the country. Each hazard requires a scientific evaluation which will include at least the following aspects:
- its cause or causes
- its geographical distribution, magnitude or severity and probable frequency of occurrence
- the physical mechanisms of destruction
- the elements and activities most vulnerable to destruction
- possible social and economic consequences of a disaster.
Areas at high risk of earthquakes, volcanoes and floods need to have hazard zone maps prepared by experts to predict the locations and nature of the impacts when a major event occurs. Such hazard assessments can then be used by land-use planners for long-term risk reduction, and by emergency planners who have to deal with the pre-disaster response. However, seismic zoning for earthquakes and hazard mapping for volcanoes are still in their infancy in most developing countries, and extending such risk mapping is seen as a crucial need in the IDNDR.
Hazard assessment for natural hazards requires a detailed study of the records of previous disasters in the preceding centuries and exacting geological field work to ascertain major events such as earthquakes and volcanic eruptions in historic or prehistoric times. Learning about the behaviour of major natural phenomena in the past is a good, but far from infallible, guide for hazard assessment for future events. There are standard hydrological methods for flood estimation, and many flood-prone areas can be easily recognized because they coincide with a well-defined natural flood plain. For tropical cyclones, records of impacts around coastlines can be used to determine the probability of a hurricane striking any one part of the coastline in a year, but each hurricane has to be urgently monitored as soon as it has formed in order to actually forecast its path and speed at least 72 hours ahead, before it makes landfall. Associated with earthquakes, volcanoes and heavy rains are landslides which may be triggered by these phenomena. In the last decade it has been increasingly appreciated that many large volcanoes are at risk from slope failure because of the instability of their mass, which has been built up during periods of activity, and devastating landslides may result.
With technological disasters, local communities need to make inventories of the hazardous industrial activities in their midst. There are now ample examples from past major accidents of what these hazards can lead to, should a failure in a process or containment occur. Quite detailed plans now exist for chemical accidents around hazardous installations in many developed countries.
Risk Assessment
After evaluating a hazard and its likely impacts, the next step is to undertake a risk assessment. Hazard may be defined as the possibility of harm, and risk is the probability of lives being lost, persons injured or property damaged due to a given type and magnitude of natural hazard. Risk can be quantitatively defined as:
Risk = value x vulnerability x hazard
where value can represent a potential number of lives or capital value (of buildings, for example) which may be lost in the event. Ascertaining vulnerability is a key part of risk assessment: for buildings it is the measure of the intrinsic susceptibility of structures exposed to potentially damaging natural phenomena. For example, the likelihood of a building collapsing in an earthquake can be determined from its location relative to a fault line and the seismic resistance of its structure. In the above equation the degree of loss resulting from the occurrence of a natural phenomenon of a given magnitude can be expressed on a scale from 0 (no damage) to 1 (total loss), while hazard is the specific risk expressed as a probability of preventable loss per unit time. Vulnerability is therefore the fraction of value that is likely to be lost as a result of an event. The information needed for making a vulnerability analysis can come, for example, from surveys of homes in hazard areas by architects and engineers. Figure 1 provides some typical risk curves.
Figure 1. Risk is a product of hazard and vulnerability: typical curve shapes
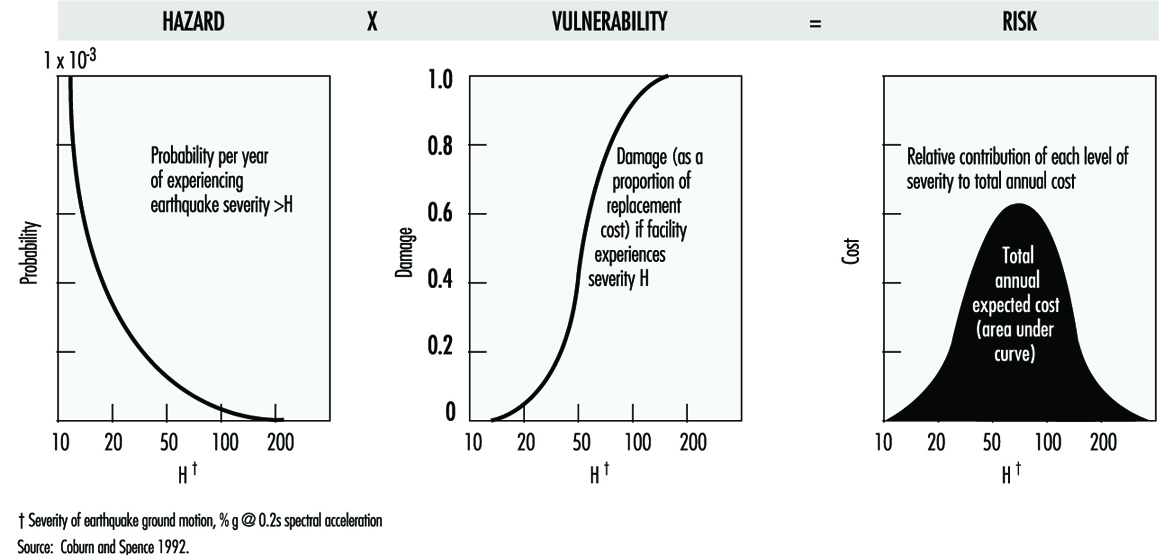
Vulnerability assessments utilizing information on different causes of death and injury according to the different types of impact are much more difficult to undertake at the present time, as the data on which to base them are crude, even for earthquakes, since standardization of injury classifications and even the accurate recording of the number, let alone the causes of deaths, are not yet possible. These serious limitations show the need for much more effort to be put into epidemiological data-gathering in disasters if preventive measures are to develop on a scientific basis.
At present mathematical computation of risk of building collapse in earthquakes and from ash falls in volcanic eruptions can be digitalized onto maps in the form of risk scales, to graphically demonstrate those areas of high risk in a foreseeable event and predict where, therefore, civil defence preparedness measures should be concentrated. Thus risk assessment combined with economic analysis and cost effectiveness will be invaluable in deciding between different options for risk reduction.
In addition to building structures, the other important aspect of vulnerability is infrastructure (lifelines) such as:
- transport
- telecommunications
- water supplies
- sewer systems
- electricity supplies
- health care facilities.
In any natural disaster all of these are at risk of being destroyed or heavily damaged, but as the type of destructive force may differ according to the natural or technological hazard, appropriate protective measures need to be devised in conjunction with the risk assessment. Geographical information systems are modern computer techniques for mapping different data sets to assist in such tasks.
In planning for chemical disasters, quantified risk assessment (QRA) is used as a tool to determine the probability of plant failure and as a guide for decision makers, by providing numerical estimates of risk. Engineering techniques for making this type of analysis are well advanced, as are the means of developing hazard zone maps around hazardous installations. Methods exist for predicting pressure waves and concentrations of radiant heat at different distances from the sites of vapour or flammable gas explosions. Computer models exist for predicting the concentration of denser-than-air gases for kilometres downwind from an accidental release in specified amounts from a vessel or plant under different weather conditions. In these incidents vulnerability mainly has to do with the proximity of housing, schools, hospitals and other key installations. Individual and societal risks need to be computed for the different types of disaster and their significance should be communicated to the local population as part of overall disaster planning.
Risk Reduction
Once vulnerability has been assessed, the feasible measures to reduce vulnerability and overall risk need to be devised.
Thus new buildings should be made seismic resistant if built in a seismic zone, or old buildings can be retrofitted so that they are less likely to collapse. Hospitals may need resiting or “hardening” against hazards such as windstorms, for example. The need for good roads as evacuation routes must never be forgotten in land developments in areas at risk of windstorms or volcanic eruptions and a host of other civil engineering measures can be enacted depending upon the situation. In the longer term the most important measure is the regulation of land use to prevent the development of settlements in hazardous areas, such as flood plains, the slopes of active volcanoes or around major chemical plants. Over-reliance on engineering solutions can bring false reassurance in at-risk areas, or be counterproductive, increasing the risk of rare catastrophic events (e.g., building levees along major rivers prone to severe flooding).
Emergency Preparedness
The planning and organization of emergency preparedness should be a task for a multidisciplinary planning team involved at the community level, and one which should be integrated into hazard assessment, risk reduction and emergency response. In the management of casualties it is now well recognized that medical teams from outside may take at least three days to arrive at the scene in a developing country. As most preventable deaths occur within the first 24 to 48 hours, such assistance will arrive too late. Thus it is at the local level that emergency preparedness should be focused, so that the community itself has the means to begin rescue and relief actions immediately after an event.
Providing adequate information to the public in the planning phase should therefore be a key aspect of emergency preparation.
Information and communication needs
On the basis of the hazard and risk analyses, the means of providing early warning will be essential, together with a system for evacuating people from areas of high risk should an emergency arise. Pre-planning of communications systems between the different emergency services at the local and national levels is necessary and for the effective provision and dissemination of information in a disaster a formal chain of communication will have to be established. Other measures such as stockpiling emergency food and water supplies in households may be included.
A community near a hazardous installation needs to be aware of the warning it may receive in an emergency (e.g., a siren if there is a gas release) and the protective measures people should adopt (e.g., immediately go inside houses and close windows until advised to come out). An essential feature of a chemical disaster is the need to be able to rapidly define the health hazard posed by a toxic release, which means identifying the chemical or chemicals involved, having access to knowledge of their acute or long-term effects and determining who, if anyone, in the general population has been exposed. Establishing lines of communication with poison information and chemical emergency centres is an essential planning measure. Unfortunately it may be difficult or impossible to know the chemicals involved in the event of runaway reactions or chemical fires, and even if it is easy to identify a chemical, knowledge of its toxicology in humans, particularly chronic effects, may be sparse or non-existent, as was found after the release of methyl isocyanate at Bhopal. Yet without information on the hazard, the medical management of casualties and the exposed population, including decisions on the need for evacuation from the contaminated area, will be severely hampered.
A multidisciplinary team to gather information and to undertake rapid health risk assessments and environmental surveys to exclude contamination of ground, water and crops should be pre-planned, recognizing that all available toxicological databases may be inadequate for decision making in a major disaster, or even in small incidents in which a community believes it has suffered serious exposure. The team should have the expertise to confirm the nature of the chemical release and to investigate its likely health and environmental impacts.
In natural disasters, epidemiology is also important for making an assessment of the health needs in the post-impact phase and for infectious diseases surveillance. Information gathering on the effects of the disaster is a scientific exercise which should also be part of a response plan; a designated team should undertake this work to provide important information for the disaster coordinating team as well as for assisting in the modification and improvement of the disaster plan.
Command and control and emergency communications
The designation of the emergency service in charge, and the constitution of a disaster coordinating team, will vary from country to country and with the type of disaster, but it needs to be pre-planned. At the scene a specific vehicle may be designated as the command and control, or onsite coordinating centre. For example, emergency services cannot rely on telephone communications, as these may become overloaded, and so radio links will be needed.
The hospital major incident plan
The capability of hospitals in terms of staff, physical reserves (theatres, beds and so on) and treatment (medicines and equipment) for dealing with any major incident will need to be assessed. Hospitals should have specific plans for dealing with a sudden large influx of casualties, and there should be provision for a hospital flying squad to go to the scene to work with search and rescue teams in extricating trapped victims or to undertake field triage of large numbers of casualties. Major hospitals may be unable to function because of disaster damage, as happened in the earthquake in Mexico City in 1985. Restoring or supporting devastated health services may therefore be necessary. For chemical incidents, hospitals should have established links with poison information centres. As well as being able to draw on a large fund of health care professionals from inside or outside a disaster area to cope with the injured, planning should also include the means for the rapid sending of emergency medical equipment and drugs.
Emergency equipment
The types of search and rescue equipment needed for a specific disaster should be identified at the planning stage along with where it will be stored, as it will need to be rapidly deployed in the first 24 hours, when the most lives can be saved. Key medicines and medical equipment need to be available for rapid deployment, along with personal protective equipment for emergency crews, including health workers at the disaster scene. Engineers skilled in urgently restoring water, electricity, communications and roads can have a major role in alleviating the worst effects of disasters.
Emergency response plan
The separate emergency services and the health care sector, including public health, occupational health and environmental health practitioners, should each have plans for dealing with disasters, which can be incorporated together as one major disaster plan. In addition to the hospital plans, health planning should include detailed response plans for different types of disaster, and these need to be devised in the light of the hazard and risk assessments produced as part of disaster preparedness. Treatment protocols should be drawn up for the specific types of injury that each disaster may produce. Thus a range of traumas, including crush syndrome, should be anticipated from the collapse of buildings in earthquakes, whereas body burns and inhalational injuries are a feature of volcanic eruptions. In chemical disasters, triage, decontamination procedures, the administration of antidotes where applicable and emergency treatment of acute pulmonary injury from irritant toxic gases should all be planned for. Forward planning should be flexible enough to cope with transport emergencies involving toxic substances, especially in areas without fixed installations which would normally require the authorities to make intensive local emergency plans. The emergency management of physical and chemical trauma in disasters is a vital area of health care planning and one which requires training of hospital staff in disaster medicine.
The management of evacuees, the location of evacuation centres and the appropriate preventive health measures should be included. The need for emergency stress management to prevent stress disorders in victims and emergency workers should also be considered. Sometimes psychological disorders may be the predominant or even the only health impact, particularly if the response to an incident has been inadequate and engendered undue anxiety in the community. This is also a special problem of chemical and radiation incidents which can be minimized with adequate emergency planning.
Training and education
Medical staff and other health care professionals at the hospital and primary care level are likely to be unfamiliar with working in disasters. Training exercises involving the health sector and the emergency services are a necessary part of emergency preparedness. Table-top exercises are invaluable and should be made as realistic as possible, since large-scale physical exercises are likely to be held very infrequently because of their high cost.
Post-impact recovery
This phase is the returning of the affected area to its pre-disaster state. Pre-planning should include post-emergency social, economic and psychological care and rehabilitation of the environment. For chemical incidents the latter also includes environmental assessments for contaminants of water and crops, and remedial actions, if needed, such as decontamination of soils and buildings and restoration of potable water supplies.
Conclusion
Relatively little international effort has been put into disaster preparedness compared to relief measures in the past; however, although investment in disaster protection is costly, there is now a large body of scientific and technical knowledge available which if applied correctly would make a substantial difference to the health and economic impacts of disasters in all countries.
Post-Disaster Activities
Industrial accidents may affect groups of workers exposed in the workplace as well as the population living around the plant where the accident takes place. When pollution caused by accident occurs, the size of the affected population is likely to be orders of magnitude greater than the workforce, posing complex logistic problems. The present article focuses on these problems, and applies to agricultural accidents as well.
Reasons for quantifying health effects of an accident include:
- the need to ensure that all exposed persons have received medical attention (regardless of whether or not treatment was actually needed by each of them). Medical attention may consist of the search for and alleviation of clinically recognizable adverse consequences (if any) as well as implementation of means for preventing possible delayed effects and complications. This is obligatory when an accident occurs within a plant; then all the people working there will be known and full follow-up is feasible
- the need to identify persons deserving of compensation as victims of the accident. This implies that individuals must be characterized as to the severity of disease and the credibility of a causal association between their condition and the disaster.
- the acquisition of new knowledge on disease pathogenesis in humans
- the scientific interest of unravelling mechanisms of toxicity in humans, including those aspects which may help in reassessing, for a given exposure, doses considered to be “safe” in humans.
Characterization of Accidents in Relation to Health Consequences
Environmental accidents include a broad range of events occurring under the most diverse of circumstances. They may be first noticed or suspected because of environmental changes or because of the occurrence of disease. In both situations, the evidence (or suggestion) that “something may have gone wrong” may appear suddenly (e.g., the fire in the Sandoz storehouse in Schweizerhalle, Switzerland, in 1986; the epidemic of the condition later labelled as “toxic oil syndrome” (TOS) in Spain in 1981) or insidiously (e.g., excesses of mesothelioma following environmental—non-occupational—exposure to asbestos in Wittenoom, Australia). In all circumstances, at any given moment, uncertainty and ignorance surround both key questions: “Which health consequences have occurred so far?” and “What can be predicted to occur?”
In assessing the impact of an accident on human health, three types of determinants may interact:
- the agent(s) being released, its hazardous properties and the risk created by its release
- the individual disaster experience
- the response measures (Bertazzi 1991).
The nature and quantity of the release might be difficult to determine, as well as the ability of the material to enter into the different compartments of the human environment, such as the food chain and water supply. Twenty years after the accident, the amount of 2,3,7,8-TCDD released in Seveso on July 10, 1976, remains a matter of dispute. In addition, with the limited knowledge about the toxicity of this compound, in the early days after the accident, any prediction of risk was necessarily questionable.
Individual disaster experience consists of fear, anxiety and distress (Ursano, McCaughey and Fullerton 1994) consequent to the accident, irrespective of the nature of the hazard and of the actual risk. This aspect covers both conscious—not necessarily justified—behavioural changes (e.g., the marked decrease in birth rates in many Western European Countries in 1987, following the Chernobyl accident) and psychogenic conditions (e.g., symptoms of distress in school children and Israeli soldiers following the escape of hydrogen sulphide from a faulty latrine in a school on the West Bank of Jordan in 1981). Attitudes towards the accident are also influenced by subjective factors: in Love Canal, for instance, young parents with little experience of contact with chemicals in the workplace were more prone to evacuate the area than were older people with grown-up children.
Finally, an accident may have an indirect impact on the health of those exposed, either creating additional hazards (e.g., distress associated with evacuation) or, paradoxically, leading to circumstances with some potential for benefit (such as people who stop smoking tobacco as a consequence of contact with the milieu of health workers).
Measuring the Impact of an Accident
There is no doubt that each accident requires an assessment of its measurable or potential consequences on the exposed human population (and animals, domestic and/or wild), and periodic updates of such assessment may be required. In fact, many factors influence the detail, extent and nature of the data which can be collected for such an assessment. The amount of available resources is critical. Accidents of the same severity may be granted different levels of attention in different countries, in relation to the ability to divert resources from other health and social issues. International cooperation may partly mitigate this discrepancy: in fact, it is limited to episodes which are particularly dramatic and/or present unusual scientific interest.
The overall impact of an accident upon health ranges from negligible to severe. Severity depends on the nature of the conditions which are produced by the accident (which may include death), on the size of the exposed population, and on the proportion that develop disease. Negligible effects are more difficult to demonstrate epidemiologically.
Sources of data to be used for evaluating health consequences of an accident include in the first place current statistics which exist already (attention to their potential use should always precede any suggestion of creating new population databases). Additional information can be derived from analytical, hypothesis-centred epidemiological studies for the purpose of which current statistics may or may not be useful. If in an occupational setting no health surveillance of the workers is present, the accident can provide the opportunity to establish a surveillance system which will eventually help to protect workers from other potential health hazards.
For the purposes of clinical surveillance (short or long term) and/or provision of compensation, the exhaustive enumeration of the exposed persons is a sine qua non. This is relatively simple in the case of intra-factory accidents. When the affected population can be defined by the place where they live, the list of residents in administrative municipalities (or smaller units, when available) provides a reasonable approach. The construction of a roster may be more problematic under other circumstances, particularly when the need is for a list of people showing symptoms possibly attributable to the accident. In the TOS episode in Spain, the roster of persons to be included in the long-term clinical follow-up was derived from the list of the 20,000 persons applying for financial compensation, subsequently corrected through a revision of the clinical records. Given the publicity of the episode, it is believed that this roster is reasonably complete.
A second requirement is that activities aiming at the measure of the impact of an accident be rational, clear-cut and easy to explain to the affected population. Latency may range between days and years. If some conditions are met, the nature of disease and probability of occurrence can be hypothesized a priori with a precision sufficient for the adequate design of a clinical surveillance programme and ad hoc studies aiming at one or more of the goals mentioned at the beginning of this article. These conditions include the rapid identification of the agent released by the accident, availability of adequate knowledge on its short- and long-term hazardous properties, a quantification of the release, and some information on inter-individual variation in susceptibility to the agent’s effects. In fact, these conditions are rarely met; a consequence of the underlying uncertainty and ignorance is that the pressure of public opinion and the media for prevention or definite medical intervention of doubtful usefulness is more difficult to resist.
Finally, as soon as possible after the occurrence of an accident has been established, a multidisciplinary team (including clinicians, chemists, industrial hygienists, epidemiologists, human and experimental toxicologists) needs to be established, which will be responsible to the political authority and the public. In the selection of experts, it must be borne in mind that the range of chemicals and technology which may underlie an accident is very large, so that different types of toxicity involving a variety of biochemical and physiological systems may result.
Measuring the Impact of Accidents through Current Statistics
Current health status indicators (such as mortality, natality, hospital admissions, sickness absence from work and physician visits) have the potential to provide early insight on the consequences of an accident, provided they are stratifiable for the affected region, which often will not be possible because affected areas can be small and not necessarily overlapping with administrative units. Statistical associations between the accident and an excess of early events (occurring within days or weeks) detected through existing health status indicators are likely to be causal, but do not necessarily reflect toxicity (e.g., an excess of physician visits may be caused by fear rather than by actual occurrence of disease). As always, care must be exercised when interpreting any change in health status indicators.
Although not all accidents produce death, mortality is an easily quantifiable endpoint, either by direct count (e.g., Bhopal) or through comparisons between observed and expected number of events (e.g., acute episodes of air pollution in urban areas). Ascertaining that an accident has not been associated with an early excess of mortality may help in assessing the severity of its impact and in addressing attention to non-lethal consequences. Further, the statistics needed in order to calculate expected numbers of deaths are available in most countries and allow for estimates in areas as small as those which are usually affected by an accident. Assessing mortality from specific conditions is more problematic, because of possible bias in certifying causes of death by health officers who are aware of the diseases expected to increase after the accident (diagnostic suspicion bias).
From the foregoing, the interpretation of health status indicators based on existing data sources requires a careful design of ad hoc analyses, including a detailed consideration of possible confounding factors.
On occasions, early after an accident, the question is posed whether the creation of a conventional population-based cancer registry or a registry of malformations is warranted. For these specific conditions, such registries may provide more reliable information than other current statistics (such as mortality or hospital admissions), particularly if newly created registries are run according to internationally acceptable standards. Nevertheless, their implementation requires the diversion of resources. In addition, if a population-based registry of malformations is established de novo after an accident, probably within nine months it will hardly be capable of producing data comparable to those produced by other registries and a series of inferential problems (particularly statistical error of the second type) will ensue. In the end, the decision largely relies on the evidence of carcinogenicity, embryotoxicity or teratogenicity of the hazard(s) which have been released, and on possible alternative uses of the available resources.
Ad Hoc Epidemiological Studies
Even in areas covered by the most accurate systems for monitoring the reasons for patients’ contacts with physicians and/or hospital admissions, indicators from these areas will not provide all the information needed in order to assess the health impact of an accident and the adequacy of the medical response to it. There are specific conditions or markers of individual response which either do not require contact with the medical establishment or do not correspond to the disease classifications conventionally used in current statistics (so that their occurrence would hardly be identifiable). There may be the need for counting as “victims” of the accident, subjects whose conditions are borderline between occurrence and non-occurrence of disease. It is often necessary to investigate (and evaluate the efficacy of) the range of therapeutical protocols which are used. The problems noted here are but a sampling and do not cover all those which might create the need for an ad hoc investigation. In any case, procedures should be established in order to receive additional complaints.
Investigations differ from the provision of care in that they are not directly related to the individual’s interest as a victim of the accident. An ad hoc investigation should be shaped in order to fulfil its purposes—to provide reliable information and/or demonstrate or disprove a hypothesis. Sampling may be reasonable for research purposes (if accepted by the affected population), but not in the provision of medical care. For instance, in the case of a spill of an agent suspected of damaging bone marrow, there are two totally different scenarios in order to respond to each of the two questions: (1) whether the chemical actually induces leukopenia, and (2) whether all exposed persons have been exhaustively screened for leukopenia. In an occupational setting both questions can be pursued. In a population, the decision also will depend on the possibilities for constructive intervention to treat those affected.
In principle, there is a need to have sufficient epidemiological skill locally to contribute to the decision on whether ad hoc studies ought to be carried out, to design them and to supervise their conduct. However, health authorities, media and/or the population may not consider the epidemiologists of the affected area to be neutral; thus, help from outside may be needed, even at a very early stage. The same epidemiologists should contribute to the interpretation of descriptive data based on the currently available statistics, and to the development of causal hypotheses when needed. If epidemiologists are not available locally, collaboration with other institutions (usually, National Institutes of Health, or WHO) is necessary. Episodes which are unravelled because of the lack of epidemiological skill are regrettable.
If an epidemiological study is believed to be necessary, however, attention should be addressed to some preliminary questions: To what use will predictable results be put? Might the desire for a more refined inference resulting from the planned study unduly delay clean-up procedures or other preventive measures? Must the proposed research programme first be fully documented and evaluated by the multidisciplinary scientific team (and perhaps by other epidemiologists)? Will there be adequate provision of details to the persons to be studied to ensure their fully informed, prior and voluntary consent? If a health effect is found, what treatment is available and how will it be delivered?
Finally, conventional prospective cohort mortality studies ought to be implemented when the accident has been severe and there are reasons to fear later consequences. Feasibility of these studies differs between countries. In Europe, they range between the possibility of nominal “flagging” of persons (e.g., rural populations in Shetland, UK, following the Braer Oil Spill) and the need for systematic contacts with the victims’ families in order to identify dying persons (e.g., TOS in Spain).
Screening for Prevalent Conditions
Offering affected people medical attention is a natural reaction to an accident which may have caused them harm. The attempt to identify all those in the exposed population who exhibit conditions related to the accident (and give them medical care if needed) corresponds to the conventional concept of screening. Basic principles, potentialities and limitations common to any screening programme (regardless of the population to which it is addressed, the condition to be identified and the tool used as a diagnostic test) are as valid after an environmental accident as in any other circumstance (Morrison 1985).
Estimating participation and understanding reasons for non-response are just as crucial as measuring sensitivity, specificity and predictive value of the diagnostic test(s), designing a protocol for subsequent diagnostic procedures (when needed) and the administration of therapy (if required). If these principles are neglected, short- and/or long-term screening programmes may produce more harm than benefit. Unnecessary medical examinations or laboratory analyses are a waste of resources and a diversion from providing necessary care to the population as a whole. Procedures for ensuring a high level of compliance have to be carefully planned and evaluated.
Emotional reactions and uncertainties surrounding environmental accidents may further complicate things: physicians tend to loose specificity when diagnosing borderline conditions, and some “victims” may consider themselves entitled to receive medical treatment regardless of whether or not it is actually needed or even useful. In spite of the chaos which often follows an environmental accident, some sine qua non for any screening programme should be borne in mind:
- Procedures should be laid down in a written protocol (including second level diagnostic tests and therapy to be provided to those who are found to be affected or sick).
- One person should be identified as responsible for the programme.
- There should be a preliminary estimate of specificity and sensitivity of the diagnostic test.
- There should be coordination between clinicians participating in the programme.
- Participation rates should be quantified and reviewed at regular intervals.
Some a priori estimates of efficacy of the whole programme would also help in deciding whether or not the programme is worth implementing (e.g., no programme for anticipating the diagnosis of a lung cancer should be encouraged). Also, a procedure should be established in order to recognize additional complaints.
At any stage, screening procedures may have a value of a different type—to estimate the prevalence of conditions, as a basis for an assessment of the consequences of the accident. A major source of bias in these estimates (which becomes more severe with time) is the representativeness of the exposed persons submitting themselves to the diagnostic procedures. Another problem is the identification of adequate control groups for comparing the prevalence estimates which are obtained. Controls drawn from the population may suffer from as much selection bias as the exposed person’s sample. Nevertheless, under some circumstances, prevalence studies are of the utmost importance (particularly when the natural history of the disease is not known, such as in TOS), and control groups external to the study, including those assembled elsewhere for other purposes, may be used when the problem is important and/or serious.
Use of Biological Materials for Epidemiological Purposes
For descriptive purposes, the collection of biological materials (urine, blood, tissues) from members of the exposed population can provide markers of internal dose, which by definition are more precise than (but do not replace totally) those obtainable through estimates of the concentration of the pollutant in the relevant compartments of the environment and/or through individual questionnaires. Any evaluation ought to take into account possible bias ensuing from the lack of representativeness of those members of the community from whom the biological samples were obtained.
Storing biological samples may prove useful, at a later stage, for the purpose of ad hoc epidemiological studies requiring estimates of internal dose (or early effects) at the individual level. Collecting (and properly preserving) the biological samples early after the accident is crucial, and this practice should be encouraged even in the absence of precise hypotheses for their use. The informed consent process must ensure that the patient understands that his or her biological material is to be stored for use in tests hitherto undefined. Here it is helpful to exclude the use of such specimens from certain tests (e.g., identification of personality disorders) to better protect the patient.
Conclusions
The rationale for medical intervention and epidemiological studies in the population affected by an accident ranges between two extremes—assessing the impact of agents which are proved to be potential hazards and to which the affected population is (or has been) definitely exposed, and exploring the possible effects of agents hypothesized to be potentially hazardous and suspected to be present in the area. Differences between experts (and between people in general) in their perception of the relevance of a problem are inherent to humanity. What matters is that any decision has a recorded rationale and a transparent plan of action, and is supported by the affected community.
Weather-Related Problems
It was long accepted that weather-related problems were a natural phenomenon and death and injury from such events were inevitable (see table 1). It is only in the past two decades that we have begun to look at factors contributing to weather-related death and injury as a means of prevention. Because of the short duration of study in this area, the data are limited, particularly as they pertain to the number and circumstances of weather-related deaths and injuries among workers. The following is an overview of the findings thus far.
Table 1. Weather-related occupational risks
|
Weather event |
Type of worker |
Biochemical agents |
Traumatic injuries |
Drowning |
Burns/heatstroke |
Vehicle accidents |
Mental stress |
|
Floods |
Police, Transport Underground Linemen Clean-up |
*
*** |
*
*
*
|
*
** *
|
*
|
|
* * * * |
|
Tornadoes |
Police, Transportation Cleanup |
*
** |
*
*** * |
|
|
* |
*
* |
|
Light forest fires |
Fire-fighters |
** |
** |
|
** |
*** |
* |
*degree of risk.
Floods, Tidal Waves
Definitions, sources and occurrences
Flooding results from a variety of causes. Within a given climatic region, tremendous variations of flooding occur because of fluctuations within the hydrological cycle and other natural and synthetic conditions (Chagnon, Schict and Semorin 1983). The US National Weather Service has defined flash floods as those that follow within a few hours of heavy or excessive rain, a dam or levee failure or a sudden release of water impounded by an ice or log jam. Although most flash floods are the result of intense local thunderstorm activity, some occur in conjunction with tropical cyclones. Forerunners to flash floods usually involve atmospheric conditions that influence the continuation and intensity of rainfall. Other factors that contribute to flash floods include steepness of slopes (mountain terrain), absence of vegetation, lack of infiltration capability of the soil, floating debris and ice jams, rapid snow melt, dam and levee failures, rupture of a glacial lake, and volcanic disturbances (Marrero 1979). River flooding can be influenced by factors which cause flash flooding, but more insidious flooding may be caused by stream channel characteristics, character of soil and subsoil, and degree of synthetic modification along its path (Chagnon, Schict and Semorin 1983; Marrero 1979). Coastal flooding can result from storm surge, which is the result of a tropical storm or cyclone, or ocean waters driven inland by wind-generated storms. The most devastating type of coastal flooding is the tsunami, or tidal wave, which is generated by submarine earthquakes or certain volcanic eruptions. Most recorded tsunamis have occurred in the Pacific and Pacific coast regions. The islands of Hawaii are particularly prone to tsunami damage because of their location in the mid-Pacific (Chagnon, Schict and Semorin 1983; Whitlow 1979).
Factors influencing morbidity and mortality
It has been estimated that floods account for 40% of all the world’s disasters, and they do the greatest amount of damage. The most lethal flood in recorded history struck the Yellow River in 1887, when the river overflowed 70-foot-high levees, destroying 11 cities and 300 villages. An estimated 900,000 people were killed. Several hundred thousand may have died in China’s Shantung Province in 1969 when storm surges pushed flood tides up the Yellow River Valley. A sudden flood in January 1967 in Rio de Janeiro killed 1,500 people. In 1974 heavy rains flooded Bangladesh and caused 2,500 deaths. In 1963 heavy rains caused an enormous landslide that fell into the lake behind the Vaiont Dam in Northern Italy, sending 100 million tons of water over the dam and causing 2,075 deaths (Frazier 1979). In 1985 an estimated 7 to 15 inches of rain fell in a ten-hour period in Puerto Rico, killing 180 people (French and Holt 1989).
River flooding has been curtailed by engineering controls and increased forestation of watersheds (Frazier 1979). However, flash floods have increased in recent years, and are the number one weather-related killer in the United States. The increased toll from flash floods is attributed to increased and more urbanized populations on sites that are ready targets for flash floods (Mogil, Monro and Groper 1978). Fast-flowing water accompanied by such debris as boulders and fallen trees account for the primary flood-related morbidity and mortality. In the United States studies have shown a high proportion of car-related drownings in floods, due to people driving into low-lying areas or across a flooded bridge. Their cars may stall in high water or be blocked by debris, trapping them in their cars while high levels of fast-flowing water descend upon them (French et al. 1983). Follow-up studies of flood victims show a consistent pattern of psychological problems up to five years after the flood (Melick 1976; Logue 1972). Other studies have shown a significant increase in the incidence of hypertension, cardiovascular disease, lymphoma and leukaemia in flood victims, which some investigators feel are stress related (Logue and Hansen 1980; Janerich et al. 1981; Greene 1954). There is a potential for increased exposure to biological and chemical agents when floods cause disruption of water purification and sewage-disposal systems, rupture of underground storage tanks, overflowing of toxic waste sites, enhancement of vector-breeding conditions and dislodgement of chemicals stored above ground (French and Holt 1989).
Although, in general, workers are exposed to the same flood-related risks as the general population, some occupational groups are at higher risk. Clean-up workers are at high risk of exposure to biological and chemical agents following floods. Underground workers, particularly those in confined places, may be trapped during flash floods. Truck drivers and other transportation workers are at high risk from vehicle-related flood mortality. As in other weather-related disasters, fire-fighters, police and emergency medical personnel are also at high risk.
Prevention and control measures and research needs
Prevention of death and injury from floods can be accomplished by identifying flood-prone areas, making the public aware of these areas and advising them on appropriate prevention actions, conducting dam inspections and issuing dam safety certification, identifying meteorological conditions that will contribute to heavy precipitation and runoff, and issuing early warnings of floods for a specific geographic area within a specific time frame. Morbidity and mortality from secondary exposures can be prevented by assuring that water and food supplies are safe to consume and are not contaminated with biological and chemical agents, and by instituting safe human waste disposal practices. Soil surrounding toxic waste sites and storage lagoons should be inspected to determine if there has been contamination from overflowing storage areas (French and Holt 1989). Although mass vaccination programmes are counterproductive, clean-up and sanitation workers should be properly immunized and instructed in appropriate hygienic practices.
There is a need to improve technology so that early warnings for flash floods can be more specific in terms of time and place. Conditions should be assessed to determine whether evacuation should be by car or on foot. Following a flood a cohort of workers engaged in flood-related activities should be studied to assess the risk of adverse physical and mental health effects.
Hurricanes, Cyclones, Tropical Storms
Definitions, sources and occurrences
A hurricane is defined as a rotating wind system that whirls counterclockwise in the northern hemisphere, forms over tropical water, and has sustained wind speeds of at least 74 miles per hour (118.4 km/h). This whirling accumulation of energy is formed when circumstances involving heat and pressure nourish and nudge the winds over a large area of ocean to wrap themselves around an atmospheric low-pressure zone. A typhoon is comparable to a hurricane except that it forms over Pacific waters. Tropical cyclone is the term for all wind circulations rotating around an atmospheric low over tropical waters. A tropical storm is defined as a cyclone with winds from 39 to 73 mph (62.4 to 117.8 km/h), and a tropical depression is a cyclone with winds less than 39 mph (62.4 km/h).
It is presently thought that many tropical cyclones originate over Africa, in the region just south of the Sahara. They start as an instability in a narrow east to west jet stream that forms in that area between June and December, as a result of the great temperature contrast between the hot desert and the cooler, more humid region to the south. Studies show that the disturbances generated over Africa have long lifetimes, and many of them cross the Atlantic (Herbert and Taylor 1979). In the 20th century an average of ten tropical cyclones each year whirl out across the Atlantic; six of these become hurricanes. As the hurricane (or typhoon) reaches its peak intensity, air currents formed by the Bermuda or Pacific high-pressure areas shift its course northward. Here the ocean waters are cooler. There is less evaporation, less water vapour and energy to feed the storm. If the storm hits land, the supply of water vapour is cut off entirely. As the hurricane or typhoon continues to move north, its winds begin to diminish. Topographical features such as mountains may also contribute to the breakup of the storm. The geographic areas at greatest risk for hurricanes are the Caribbean, Mexico, and the eastern seaboard and Gulf Coast states of the United States. A typical Pacific typhoon forms in the warm tropical waters east of the Philippines. It may move westward and strike the Chinese mainland or veer to the north and approach Japan. The storm’s path is determined as it moves around the western edge of the Pacific high-pressure system (Understanding Science and Nature: Weather and Climate 1992).
The destructive power of a hurricane (typhoon) is determined by the way storm surge, wind and other factors are combined. Forecasters have developed a five-category disaster potential scale to make the predicted hazards of approaching hurricanes clearer. Category 1 is a minimum hurricane, category 5 a maximum hurricane. In the period 1900-1982, 136 hurricanes struck the United States directly; 55 of these were of at least category 3 intensity. Florida felt the effects of both the highest number and the most intense of these storms, with Texas, Louisiana and North Carolina following in descending order (Herbert and Taylor 1979).
Factors influencing morbidity and mortality
Although winds do much damage to property, the wind is not the biggest killer in a hurricane. Most victims die from drowning. The flooding that accompanies a hurricane may come from the intense rain or from the storm surges. The US National Weather Service estimates that storm surges cause nine of every ten hurricane-associated fatalities (Herbert and Taylor 1979). The occupational groups most heavily impacted by hurricanes (typhoons) are those related to boating and shipping (which would be affected by the unusually rough seas and high winds); utility line workers who are called into service to repair damaged lines, often while the storm is still raging; fire-fighters and police officers, who are involved in evacuations and protecting the property of evacuees; and emergency medical personnel. Other occupational groups are discussed in the section on floods.
Prevention and control, research needs
The incidence of deaths and injuries associated with hurricanes (typhoons) has dropped dramatically in the past twenty years in those areas where sophisticated advanced warning systems have been put into effect. The principal steps to follow for preventing death and injury are: to identify meteorological precursors of these storms and track their course and potential development into hurricanes, to issue early warnings to provide for timely evacuation when indicated, to enforce stringent land use management practices and building codes in high-risk areas, and to develop emergency contingency plans in high-risk areas to provide for an orderly evacuation and adequate shelter capacity for evacuees.
Because the meteorological factors contributing to hurricanes have been well studied, a good deal of information is available. More information is needed on the variable pattern of incidence and intensity of hurricanes over time. The effectiveness of existing contingency plans should be assessed following each hurricane, and it should be determined if buildings protected from wind speed are also protected from storm surges.
Tornadoes
Formation and patterns of occurrence
Tornadoes are formed when layers of air of different temperature, density and windflow combine to produce powerful updrafts forming huge cumulonimbus clouds which are transformed into rotating tight spirals when strong cross winds blow through the cumulonimbus cloud. This vortex draws even more warm air into the cloud, which makes the air spin faster until a funnel cloud packing explosive force drops out of the cloud (Understanding Science and Nature: Weather and Climate 1992). The average tornado has a track approximately 2 miles long and 50 yards wide, affecting about 0.06 square miles and with wind speeds as high as 300 mph. Tornadoes occur in those areas where warm and cold fronts are apt to collide, causing unstable conditions. Although the probability that a tornado will strike any specific location is extremely small (probability 0.0363), some areas, such as the Midwest states in the United States, are particularly vulnerable.
Factors influencing morbidity and mortality
Studies have shown that people in mobile homes and in lightweight cars when tornadoes strike are at particularly high risk. In the Wichita Falls, Texas, Tornado Study, occupants of mobile homes were 40 times more likely to sustain a serious or fatal injury than those in permanent dwellings, and occupants of automobiles were at approximately five times greater risk (Glass, Craven and Bregman 1980). The leading cause of death are craniocerebral trauma, followed by crushing wounds of the head and trunk. Fractures are the most frequent form of non-fatal injury (Mandlebaum, Nahrwold and Boyer 1966; High et al. 1956). Those workers who spend a major part of their working time in lightweight automobiles, or whose offices are in mobile homes, would be at high risk. Other factors relating to clean-up operators discussed in the flood section would apply here.
Prevention and control
The issuing of appropriate warnings, and the need for the population to take appropriate action on the basis of those warnings, are the most important factors in preventing tornado-related death and injury. In the United States, the National Weather Service has acquired sophisticated instrumentation, such as Doppler radar, which permits them to identify conditions conducive to the formation of a tornado and to issue warnings. A tornado watch means that conditions are conducive to tornado formation in a given area, and a tornado warning means that a tornado has been sighted in a given area and those residing in that area should take appropriate shelter, which entails going to the basement if one exists, going to an inside room or closet, or if outside, going to a ditch or gully.
Research is needed to assess whether warnings are effectively disseminated and the extent to which people heed those warnings. It should also be determined whether the prescribed shelter areas really provide adequate protection from death and injury. Information should be gathered on the number of deaths and injuries to tornado workers.
Lightning and Forest Fires
Definitions, sources and occurrences
When a cumulonimbus cloud grows into a thunderstorm, different sections of the cloud accumulate positive and negative electric charges. When the charges have built up, the negative charges flow toward the positive charges in a lightning flash that travels within the cloud or between the cloud and the ground. Most lightning travels from cloud to cloud, but 20% travels from cloud to ground.
A lightning flash between a cloud and the ground can be either positive or negative. Positive lightning is more powerful and is more likely to start forest fires. A lightning strike will not start a fire unless it meets easily ignitable fuel like pine needles, grass and pitch. If the fire hits decaying wood, it can burn unnoticed for a long period of time. Lightning ignites fires more often when it touches the ground and the rain within the thunder cloud evaporates before it reaches the ground. This is called dry lightning (Fuller 1991). It is estimated that in dry, rural areas such as Australia and the western United States, 60% of forest fires are caused by lightning.
Factors causing morbidity and mortality
Most of the fire-fighters who die in a fire die in truck or helicopter accidents or from being hit by falling snags, rather than from the fire itself. However, fighting fire can cause heat stroke, heat exhaustion and dehydration. Heat stroke, caused by the body temperature rising to over 39.4°C, can cause death or brain damage. Carbon monoxide is also a threat, particularly in smouldering fires. In one test, researchers found that the blood of 62 of 293 fire-fighters had carboxyhaemoglobin levels above the maximum allowable level of 5% after eight hours on the fire line (Fuller 1991).
Prevention, control and research needs
Because of the danger and the mental and physical stress associated with fire-fighting, crews should not work for more than 21 days, and must have one day off for every 7 days worked within that time. In addition to wearing appropriate protective gear, fire-fighters must learn safety factors such as planning safety routes, keeping in communication, watching for hazards, keeping track of the weather, making sure of directions and acting before a situation becomes critical. The standard fire-fighting orders emphasize knowing what the fire is doing, posting lookouts and giving clear, understandable instructions (Fuller 1991).
Factors relating to prevention of lightning forest fires include limiting fuels such as dry underbrush or fire-susceptible trees like eucalyptus, preventing building in fire-prone areas and early detection of forest fires. Early detection has been enhanced by the development of new technology such as an infrared system which is mounted on helicopters to check whether lightning strikes reported from aerial lookout and detection systems have actually started fires and to map hot spots for ground crews and helicopter drops (Fuller 1991).
More information is needed on the number and circumstances of deaths and injuries associated with lightning-related forest fires.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."